
Abstract
Sudden onset, bilateral facial paralysis is a rare clinical entity, representing less than 2% of all diagnoses of facial nerve paralysis. The differential for these patients is necessarily broad and includes numerous etiologies. Metastatic breast carcinoma to the bilateral parotid glands is also exceedingly rare with only 2 reported case reports noted in the literature, neither of which demonstrated facial nerve paralysis. Here, we report the only known occurrence of a patient presenting with synchronous bilateral facial nerve paralysis secondary to metastatic breast carcinoma to the bilateral parotid glands. This exceedingly rare clinical presentation was further confounded by the presence of autoimmune antibodies, highlighting the importance of the diagnostic process and maintaining broad clinical suspicion.
Introduction
Simultaneous bilateral facial paralysis is defined as paralysis of both sides of the face within 30 days. 1 It is an exceedingly rare clinical presentation, accounting for less than 2% of all patients with facial palsy with an estimated incidence of 1 per 5 000 000 people.1,2 Unlike unilateral facial paralysis which is a common clinical entity, bilateral is idiopathic in only 20% of patients. 3 The differential for these patients therefore remains broad and includes infectious, neoplastic, congenital, neurological, systemic, or traumatic etiologies, making these cases a diagnostic challenge. 1 In the present case report, our patient presented with bilateral facial nerve paralysis in the setting of known metastatic breast cancer, raising suspicion for a neoplastic etiology.
Breast cancer is the most commonly diagnosed cancer among women and one of the most important causes of death among them. 4 Despite advances in treatment, 12% of patients are reported to develop metastasis which is associated with a poor prognosis. 5 Metastasis from breast cancer is noted to occur anywhere in the body, most commonly to the bone, lungs, brain, regional lymph nodes, and liver. 6 However, metastasis to the bilateral parotid glands is exceedingly rare, with only 2 case reports noted in the literature, neither of which demonstrated bilateral facial nerve palsy. 7
Here, we report the first ever patient with metastatic breast carcinoma to the parotid glands presenting with simultaneous bilateral facial paralysis refractory to medical therapy.
Case Report
A 35-year-old female with past medical history of metastatic breast cancer presented to the otolaryngology clinic for evaluation of simultaneous bilateral parotid gland swelling, right greater than the left. She was initially seen in the emergency department 1-month prior with parotid gland swelling and diagnosed with bilateral parotitis. She was prescribed a 1-week course of amoxicillin which resulted in no clinical improvement. Upon her presentation to our clinic, she described bilateral facial tightness, difficulty closing her eyes, difficulty smiling, epiphora, and jaw pain after eating. She denied xerostomia but did admit to polydipsia. Physical examination demonstrated bilateral indurated parotid glands without overlying erythematous changes. Of note, our neurologic examination revealed bilateral facial paralysis with trace movement in the lower and midface mimetic musculature and incomplete eye closure with minimal movement in the frontal nerve branches consistent with House-Brackman grade IV dysfunction (Figure 1A and B).
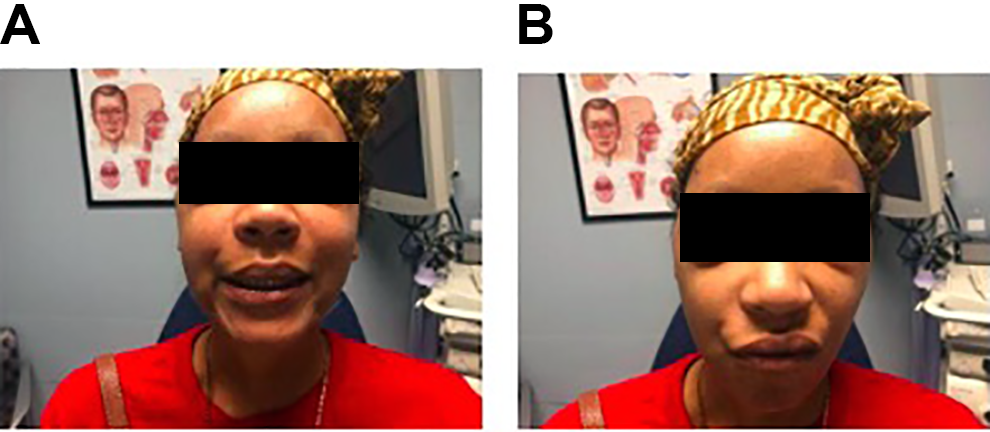
Patient now desires small black boxes over her eyes to de-identify her in both Figure 1A and 1B. A, Patient attempting to smile. B, Patient attempting to wrinkle nose.
Prior to her presentation in our clinic, a computed tomography (CT) neck with contrast was obtained for further evaluation and demonstrated heterogenous enhancement and enlargement of the bilateral parotid glands (Figure 2A). At this stage, a stepwise approach was discussed and planned with the patient. Given the patient’s age, gender, symptomatology, and examination findings, an antibody panel was initially explored to rule out autoimmune conditions like coincidental Sjogren or Sarcoidosis, as well as Lyme disease. Our patient was found to be positive for antinuclear antibodies and anti-SS-A/Ro antibodies (negative for Anti-SS-B/La). Given the concern for possible autoimmune etiology for her bilateral facial nerve paralysis, the patient was trialed on a 2-week course of prednisone.
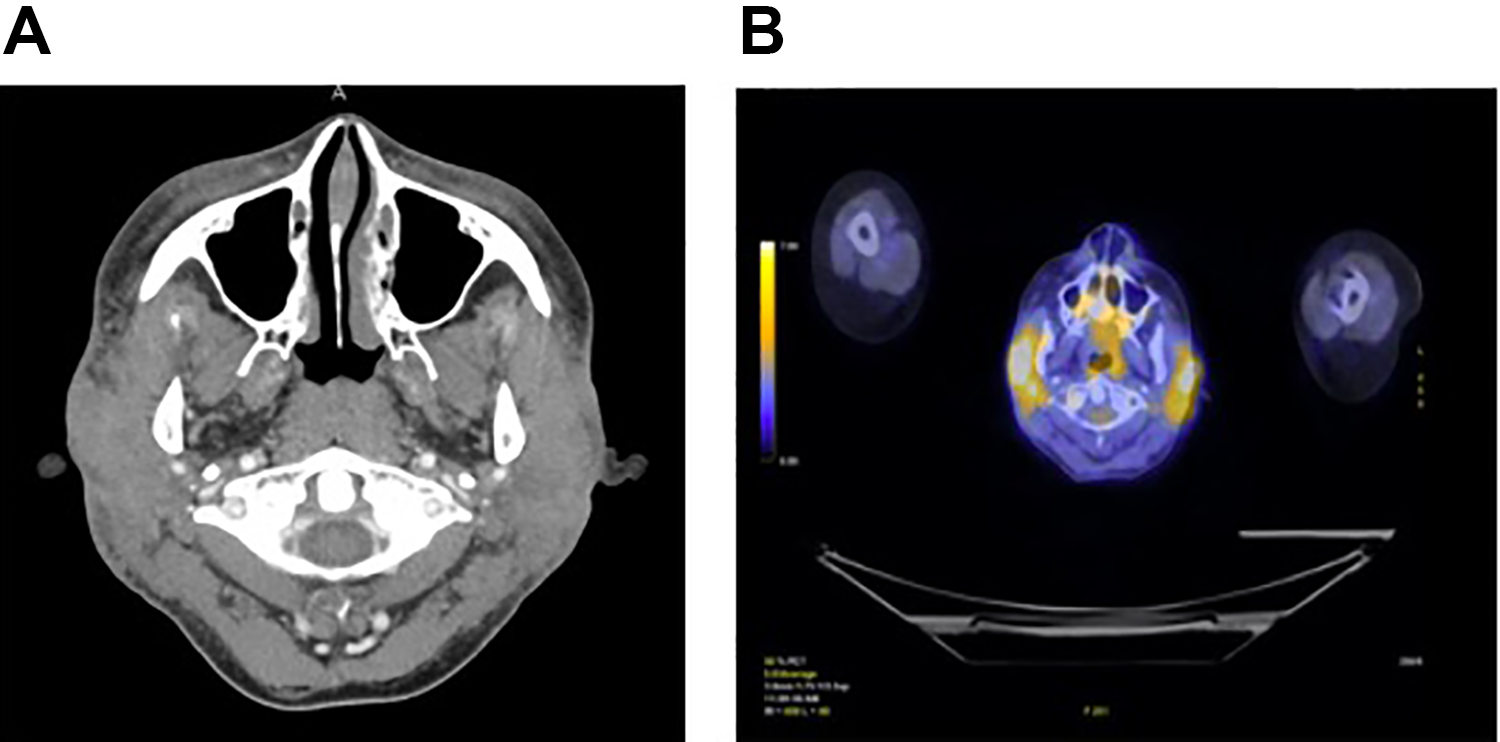
A, Computed tomography of the head with contrast—axial view, demonstrating heterogenous enhancement and enlargement of the bilateral parotid glands. B, PET imaging of the head and neck—axial view, demonstrating marked avidity of the bilateral parotid glands. PET indicates positron-emission tomography.
Ultimately, the patient did not experience any clinical improvement, and metastatic carcinoma was more strongly considered. An updated positron-emission tomography/CT was completed and demonstrated new marked avidity of the bilateral parotid glands (Figure 2B). Further workup with fine-needle aspiration (FNA) of her parotid tissue was also completed. Pap-stained cytology slides and H&E-stained cell block slides of the FNA showed small groups and clusters of cohesive, highly atypical cells with ample cytoplasm and enlarged, hyperchromatic nuclei, prominent nucleoli, and atypical mitoses (Figure 3A). These atypical cells were shown by immunohistochemistry to stain strongly positive with GATA3 (Figure 3B). Taken together with the patient’s history, these findings are strongly suggestive of a metastasis from the breast.
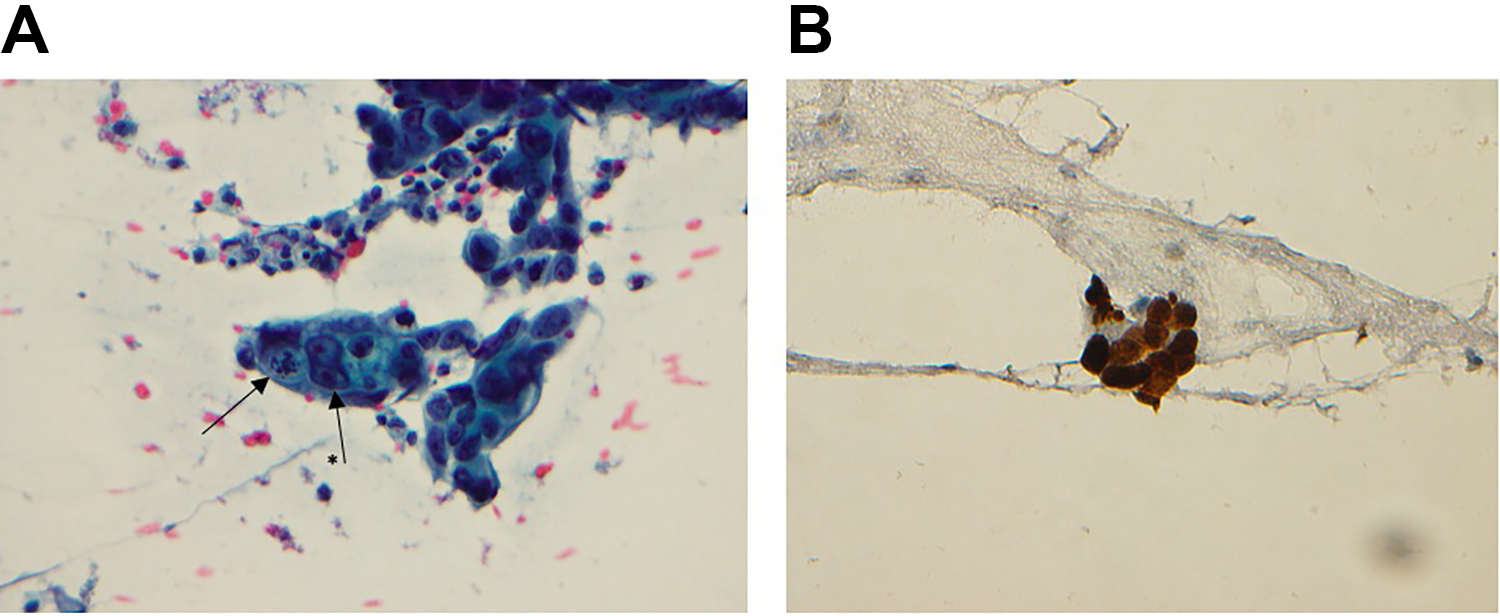
A, Pap-stained slide at ×400 magnification. Arrow demonstrating large atypical mitosis and arrow with * denotes binucleate cell. B, GATA3-stained slide at ×400 magnification.
She was subsequently seen in the oncology clinic and underwent several additional rounds of chemotherapy for this disease progression. A repeat evaluation 6 months after her initial presentation to our clinic revealed progression with dermal and epidermal erosion of her tumor metastases within her bilateral parotid glands and persistent bilateral near-complete paralysis (Figure 4).

Photos taken from the clinic, 6 months following presentation with erosive skin changes.
Discussion
Acute unilateral facial paralysis is a common clinical entity that is most often idiopathic, otherwise known as Bell’s palsy with an estimated incidence of 10 to 40 per 100 000.3,8 It is traditionally considered a diagnosis of exclusion. As part of the diagnostic workup and management, it is important to rule out known and treatable causes of paralysis with proper history, examination, and consideration of radiographic evaluation. Clinical practice guidelines have been published to guide this evaluation. 9
Simultaneous acute bilateral facial palsy in comparison is significantly less common.2,3,9 Only 20% of these patients are diagnosed with an idiopathic etiology. 2 Most commonly, bilateral facial nerve palsy is secondary to Borrelia burgdorferi (Lyme disease) accounting for approximately 35% of all cases. 3 Other infectious etiologies of bilateral facial paralysis include infectious mononucleosis, HIV, syphilis, and influenza virus. 3 Noninfectious etiologies to consider include trauma, Sarcoidosis, Amyloidosis, Sjogren syndrome, Guillain-Barre syndrome, Heerfordt-Waldenström Syndrome (Uveoparotid Fever), and Melkersson-Rosenthal Syndrome.10-12
Maintaining a broad differential and careful consideration of the patient’s history and examination is crucial to management of bilateral facial paralysis. With our patient, symptoms refractory to both antibacterial and steroid therapy, coupled with her history of metastatic breast cancer, suggested the final etiology of her presentation. This is the first report describing bilateral facial paralysis as the presenting symptom of metastatic breast carcinoma.
The prognosis of unilateral facial palsy is generally good with 71% of idiopathic cases resolving within 6 months without treatment. 8 However, the prognosis for bilateral facial nerve palsy is variable depending on the underlying etiology. If the etiology is identified early and treated appropriately, patients can experience excellent recovery with an estimated complete recovery in 80% of patients. 2 This may vary based on numerous factors include etiology, age, comorbidities, and the degree of facial paralysis. Unfortunately for our patient, metastatic disease entails a more challenging management strategy, generally implemented by our hematology/oncology colleagues, and carries a worse prognosis for recovery.
Conclusion
Bilateral spontaneous facial paralysis is a rare clinical presentation and often represents an underlying systemic disease versus the more common unilateral paralysis. Despite metastatic spread of breast adenocarcinoma to the bilateral parotid glands being extremely rare, we report a unique presentation with bilateral facial paralysis. For the patient presented herein, this diagnosis was necessarily high on the differential given the patient’s presentation. Patients who present in this manner warrant a detailed workup, taking into account pertinent patient history and examination.
Supplemental Material
Supplemental Material, sj-pdf-1-ear-10.1177_0145561320982693 - Spontaneous Bilateral Facial Paralysis Secondary to Metastatic Breast Cancer
Supplemental Material, sj-pdf-1-ear-10.1177_0145561320982693 for Spontaneous Bilateral Facial Paralysis Secondary to Metastatic Breast Cancer by Jackson King, Farrukh R. Virani, Ryan Thomas and Lane Squires in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.