
Abstract
Eosinophilic chronic rhinosinusitis (ECRS) is a Type 2 inflammatory disease that manifests as chronic inflammation of the paranasal sinus. IL-4/IL-13 receptor monoclonal antibodies (dupilumab) to suppress Type 2 inflammation have become a good treatment option for patients who are refractory to surgery. Most patients respond normally, although significant side effects such as eosinophilic pneumonia may occur, requiring discontinuation of dupilumab. Here, we present a case in which dupilumab administration caused a side-effect of eosinophilic pneumonia. A 65-year-old woman presented with nasal obstruction and olfactory dysfunction due to a nasal polyp. Her symptoms temporarily improved with dupilumab; however, dupilumab was discontinued due to eosinophilic pneumonia. Discontinuation of dupilumab resulted in the rapid resolution of eosinophilic pneumonia and reappearance of nasal polyps. We, therefore, resumed dupilumab treatment in combination with low-dose steroids; eosinophilic pneumonia did not flare up, and the nasal polyps shrank steadily. There is no established treatment strategy in cases where a side effect of eosinophilic pneumonia arises while treating ECRS with dupilumab. Based on the described case, we recommend that a combination of a low-dose steroids and dupilumab be considered as a treatment option to counter the side-effect of eosinophilic pneumonia induced by dupilumab alone.
Keywords
Introduction
Eosinophilic chronic rhinosinusitis (ECRS) is a Type 2 inflammatory disease that manifests as chronic inflammation of the upper respiratory tract. 1 It is characterised by the development of refractory nasal polyps with eosinophilic infiltration. Although various molecules have been implicated in the pathogenesis of the disease, the exact ones responsible remain to be fully elucidated.2-4 In recent years, IL-4/IL-13 receptor monoclonal antibodies (dupilumab) to suppress Type 2 inflammation have become a good treatment option for patients who are refractory to surgery. 5 However, hyper-eosinophilia may occur after administration. 5 While the majority of patients recover spontaneously, some may experience serious side effects such as eosinophilic pneumonia. Severe complications may require discontinuation of dupilumab; no standardised treatment regimen for subsequent therapy is available.
Case Report
A 65-year-old woman had nasal obstruction and olfactory dysfunction for 30 years and had undergone two sinus surgeries. Following the second surgery, the patient experienced early flare-ups of nasal symptoms, and ECRS was diagnosed via pathological examination, laboratory tests and paranasal computed tomography (CT) by a family physician. The patient was prescribed dupilumab, and although the nasal polyp had markedly shrunk after five doses, the patient developed a slight fever, a dry cough and a shadow in the right lung field on a chest radiograph. Therefore, she was referred to the respiratory medicine department of the hospital. Laboratory tests requested by the respiratory physician showed increased blood eosinophil count (%), and chest CT showed an infiltrating shadow in the right middle lung field (Figure 1A). Bronchoalveolar lavage performed with bronchoscopy revealed 70% eosinophils. The patient was hospitalised based on a diagnosis of eosinophilic pneumonia and started on 30 mg/day of prednisolone. Thereafter, the steroid dose was tapered on an outpatient basis. Subsequently, she was referred to our department because of worsening intranasal findings and recurrence of nasal obstruction and olfactory symptoms when the prednisolone dose was reduced to 5 mg/day. The patient’s general condition was good; however, nasal polyps were detected on nasal endoscopy (Figure 1B). Based on these findings, we diagnosed the patient with an ECRS relapse and determined that the nasal polyps were resistant to steroids. In accordance with the patient’s request and after consultation with a respiratory physician, we started dupilumab with low-dose prednisolone (10 mg/day), with the patient’s informed consent. After dupilumab resumption, a reduction in the polyp size and symptoms was observed (Figure 1C). Prednisolone dose reduction was started 12 weeks after resumption of dupilumab administration. The dose of prednisolone was reduced to 3 mg/day 10 months later; however, no relapse of eosinophilic pneumonia occurred (Figure 1D). The combination of low-dose steroids and dupilumab provided good control in a patient with a history of eosinophilic pneumonia. (A) Chest computed tomography at the first visit to the department of respiratory medicine. An infiltrative shadow is seen in the right lung lobe. (B) Intranasal findings at the first visit to our department. Polyp formation is seen in the nose. (C) Intranasal findings at 10 months after initiation of dupilumab and low-dose steroids. A rapid reduction in the polyp size was observed. (D) Clinical course and chest computed tomography at 6 months after initiation of dupilumab and low-dose steroids. No relapse of eosinophilic pneumonia occurred.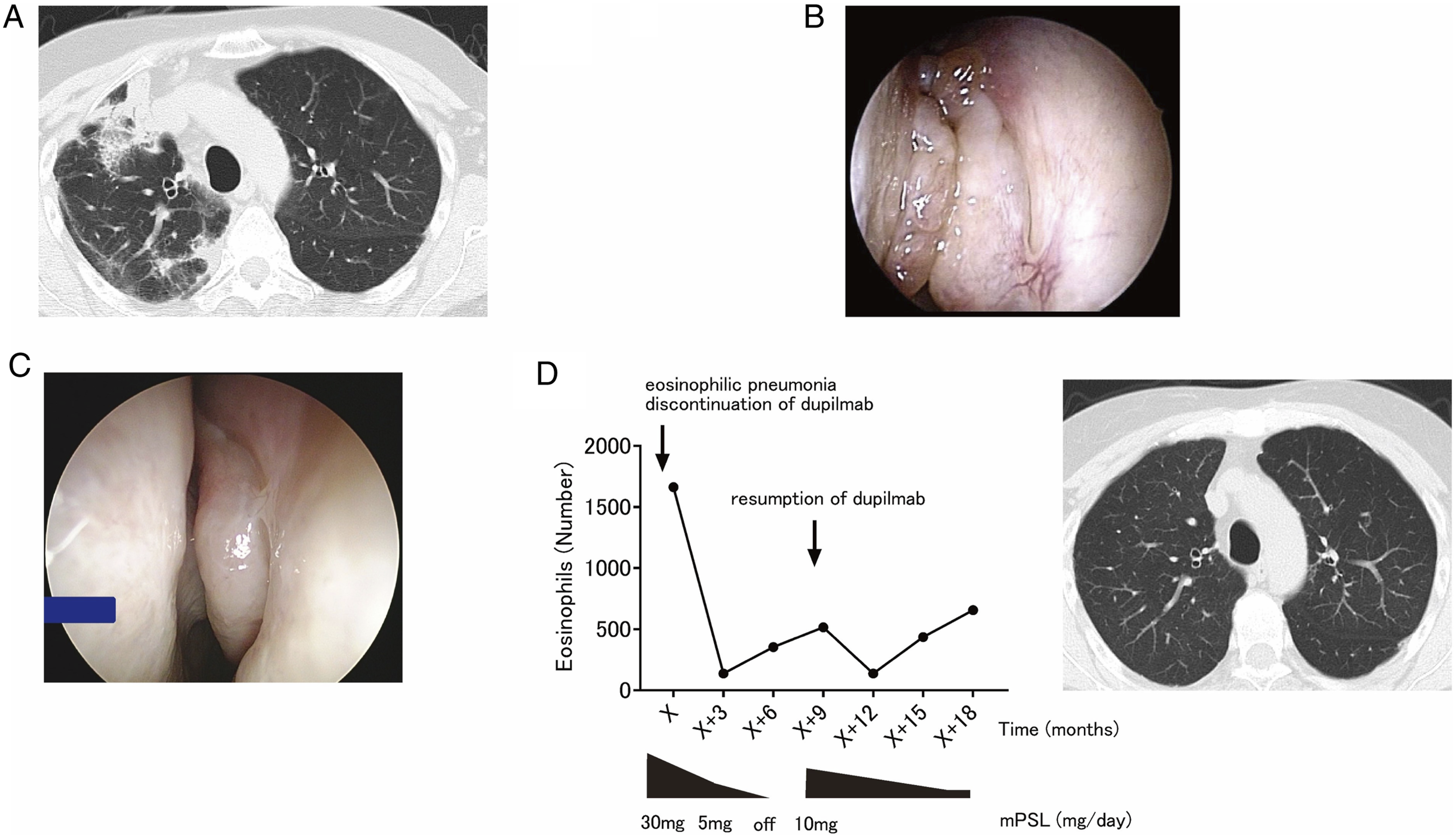
Discussion
ECRS is characterised by the formation of refractory nasal polyps with strong eosinophilic infiltration. The most common treatment is surgery or oral steroid therapy; however, relapse may occur early after surgery, and long-term oral steroid therapy must be carefully monitored for side effects. In recent years, considerably effective antibody drugs against various cytokines, such as dupilumab, have become available. Dupilumab is an effective treatment option for patients who show no improvement after surgery or who have been on long-term oral steroids. Hyper-eosinophilia is often observed after dupilumab administration and may be caused by a transient cessation of eosinophil influx from the blood to the tissues, induced by suppression of eotaxin-3 and vascular-cell adhesion molecule 1, which are regulated by the IL-4/IL-13 pathway.6,7 The disease resolves asymptomatically in most cases, but severe complications such as eosinophilic pneumonia may occur. In those cases, treatment with dupilumab should be discontinued. In our case, the patient’s symptoms improved promptly after treatment with dupilumab. However, it had to be discontinued due to the complication of eosinophilic pneumonia. Because nasal symptoms recurred after discontinuation, alternate treatment options were considered. However, no consensus was reached for the optimal treatment plan. We presented the patient with two treatment options: either reoperation, including reboot surgery, to remove the entire sinus mucosa, or a combination of low-dose steroids and dupilumab; the patient chose resumption of dupilumab. 8 Accordingly, ECRS was controlled without a recurrence of eosinophilic pneumonia, and the steroid dosage was steadily reduced.
A limitation of this report is that it documents a single case. However, to the best of our knowledge, this is the first report to reveal that dupilumab administered in combination with low-dose steroids prevents severe side effects.
In conclusion, we encountered a case in which dupilumab administration caused eosinophilic pneumonia. The patient’s eosinophilic pneumonia showed rapid improvement after the discontinuation of dupilumab and the initiation of steroid therapy, though the underlying ECRS worsened. In patients who develop severe side effects of dupilumab, treatment with low-dose steroids at dupilumab re-administration should be advised.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
This study was approved by the ethics committee of Osaka University (No.16329) and informed consent was obtained from the patient for the publication of their data.
Data Availability
The data and findings of this study are available from the corresponding author upon reasonable request.