
Abstract
The thyroid metastasis from cervical cancer is extremely rare compared to other organs. It is sometimes difficult to distinguish primary tumors from metastases, as most metastatic thyroid nodules are asymptomatic. In this case, a 54-year-old woman had undergone radical hysterectomy due to cervical tumor of stage IB1 mixed adenoneuroendocrine carcinoma (MANEC) 5 years ago. After 3 years, ultrasound examination revealed a suspicious malignant nodule in the left lobe of thyroid gland at regular postoperative follow-up. This patient had no obvious clinical symptoms. The ultrasonography (US)-guided core needle biopsy (CNB) of the thyroid nodule was performed on the patient. The immunohistochemistry analyses revealed that it was poorly differentiated small-cell neuroendocrine carcinoma (SCNEC). Subsequently, the patient underwent left hemithyroidectomy plus isthmusectomy. The postoperative pathology and immunohistochemistry, combining with clinical history, confirmed that the thyroid nodule was a metastasis from cervical MANEC. Conventional chemotherapy and regular follow-up were carried out after the operation. The patient was readmitted 1 year later for pancreatic metastatic lesions and died 1 month after surgery. Early detection of metastatic cancer is potentially helpful, and when necessary, ultrasound-guided puncture biopsy can be utilized to further diagnose metastatic thyroid cancer.
Keywords
Introduction
Neuroendocrine neoplasms (NENs) of the uterine cervix, known as an aggressive histological type, are the rare form of endocrine neoplasms, accounting for 1%–1.5% of cervical cancer reported.1,2 Neuroendocrine neoplasms are mainly occur in the pancreas, gastrointestinal tract, and lungs, having no unified classification framework for all organ systems. 3 According to tumor differentiation and proliferation, the World Health Organization classifies NENs of the digestive system into Neuroendocrine tumor (NET) G1, NET G2, NET G3, Small-cell neuroendocrine carcinoma (SCNEC), Large-cell neuroendocrine carcinoma (LCNEC), and Mixed neuroendocrine-non-neuroendocrine neoplasms (MiNENs) in 2017. Mixed adenoneuroendocrine carcinomas (MANECs) are now grouped into the conceptual category of MiNENs.4,5 Mixed adenoneuroendocrine carcinoma is proposed to be a malignant tumor, composed of glandular epithelial and neuroendocrine cells in morphology, and each component accounts for at least 30% of the tumor mass. 6 The cervical MANEC reported is very limited, and there was much less case reported about the metastasis to the thyroid from uterine cervical MANEC to date. Herein, we report a case of the thyroid metastasis diagnosed with MANEC from the uterine cervix after radical hysterectomy.
Case Presentation
A 54-year-old woman was admitted to the hospital for a thyroid nodule on the left lobe of the thyroid, which was detected by thyroid ultrasound before 20 d. Family history was not contributory. Five years ago, the patient had undergone radical hysterectomy for cervical cancer, postoperative pathology: (cervix) poorly differentiated MANEC; immunohistochemical expression: P16 (+), CEA (+), CK-L (+), CK (+), Syn and CD56 and CgA (some cells +), P63 (−), Ki67 (40% +). And, she had hyperthyroidism more than 10 years treated with oral methimazole all the time. The physical examination revealed that there was no redness or swelling of the bilateral neck skin, no palpable mass or obvious swollen lymph nodes were touched on the neck, and the trachea is centered.
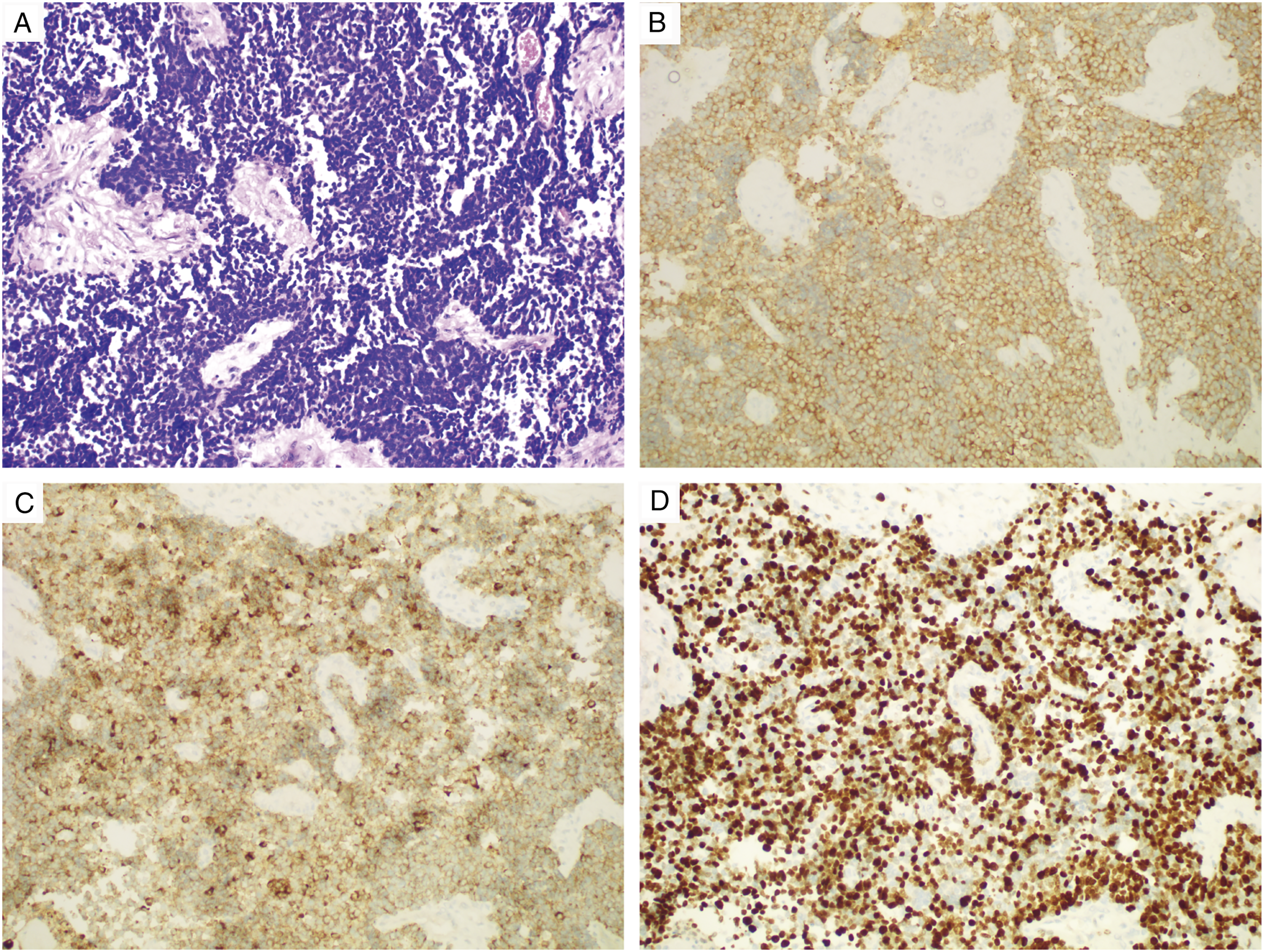
Ultrasonography (US) showed a hypoechoic nodule of about 11 mm x 8 mm in the deep lower layer of the left lobe thyroid, with irregular shape, unclear boundary, around blood flow signals in Color Doppler flow imaging (CDFI), and no lymphadenopathy (Figures 1A andB). On Two-Dimensional Shear Wave Elastography (2D SWE), the value of maximum elasticity (Emax) was 4.1 m/s (49.9 kPa) (Figure 1C). Taken together, the nodule was considered as a malignant nodule, which belongs to TI-RADS 4c. Later, core needle biopsy (CNB) was performed under ultrasound guidance with an 18-gauge core needle. Immunohistochemical analyses revealed that tumor cells stained positive for P16, Syn, CEA, CgA, CK, and Ki67 (70%+) and weakly positive for TTF1, indicating the diagnosis of poorly differentiated SCNEC (Figure 2). Ultrasound Imaging. (A) 2D ultrasound images showed a hypoechoic nodule of about 11 mm x 8 mm in the deep lower layer of the left lobe thyroid, with irregular shape, unclear boundary (red arrow). (B) Color Doppler flow imaging (CDFI) revealed blood flow signals around the nodule (red arrow). (C) 2D SWE showed the maximum elasticity (Emax) value of the nodule was 4.1 m/s (49.9 kPa). Specimen removed from the left lobe thyroid. (A) HE staining: the neoplastic cells the neoplastic cells were arranged in nests, with scanty cytoplasm, eosinophilia and obvious nucleus. (B,C) Immunohistochemical staining: tumor cells showed positive for synaptophysin (Syn), chromogranin A (CgA). (D) KI67 expression was about 70%. (A,B,C,D) x 200.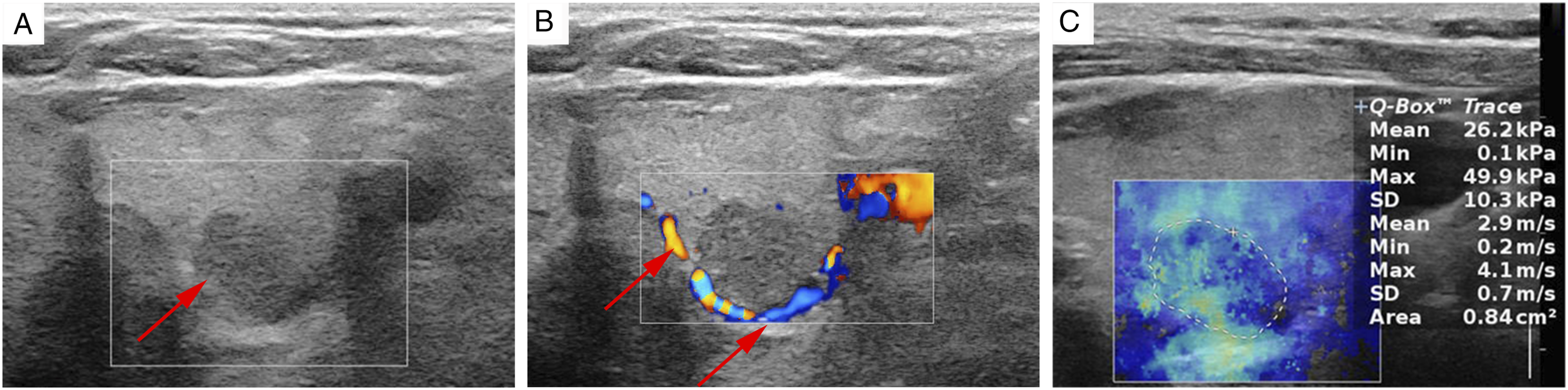
To exclude other metastatic lesions, 18F-fluorodeoxyglucose Positron emission tomography/computed tomography (18F-FDG-PET/CT) was performed. PET/CT scans revealed a slightly low-density nodule of the left lobe thyroid and irregular pleural thickening at the levels of rib 8 and 9 on the left side, both with obviously increased 18F-FDG uptake (Figure 3). The preliminary diagnosis of thyroid metastases from the original cervical MANEC was made based on US-guided CNB pathological results and clinical history. Subsequently, the patient underwent left hemithyroidectomy plus isthmusectomy, as well as ipsilateral central neck lymph node dissection. The postoperative pathological findings were consistent with CNB. 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG-PET/CT) showing a slightly low-density nodule of the left lobe thyroid and irregular pleural thickening at the levels of rib 8 and 9 on the left side, both with obviously increased 18F-FDG uptake (red arrow).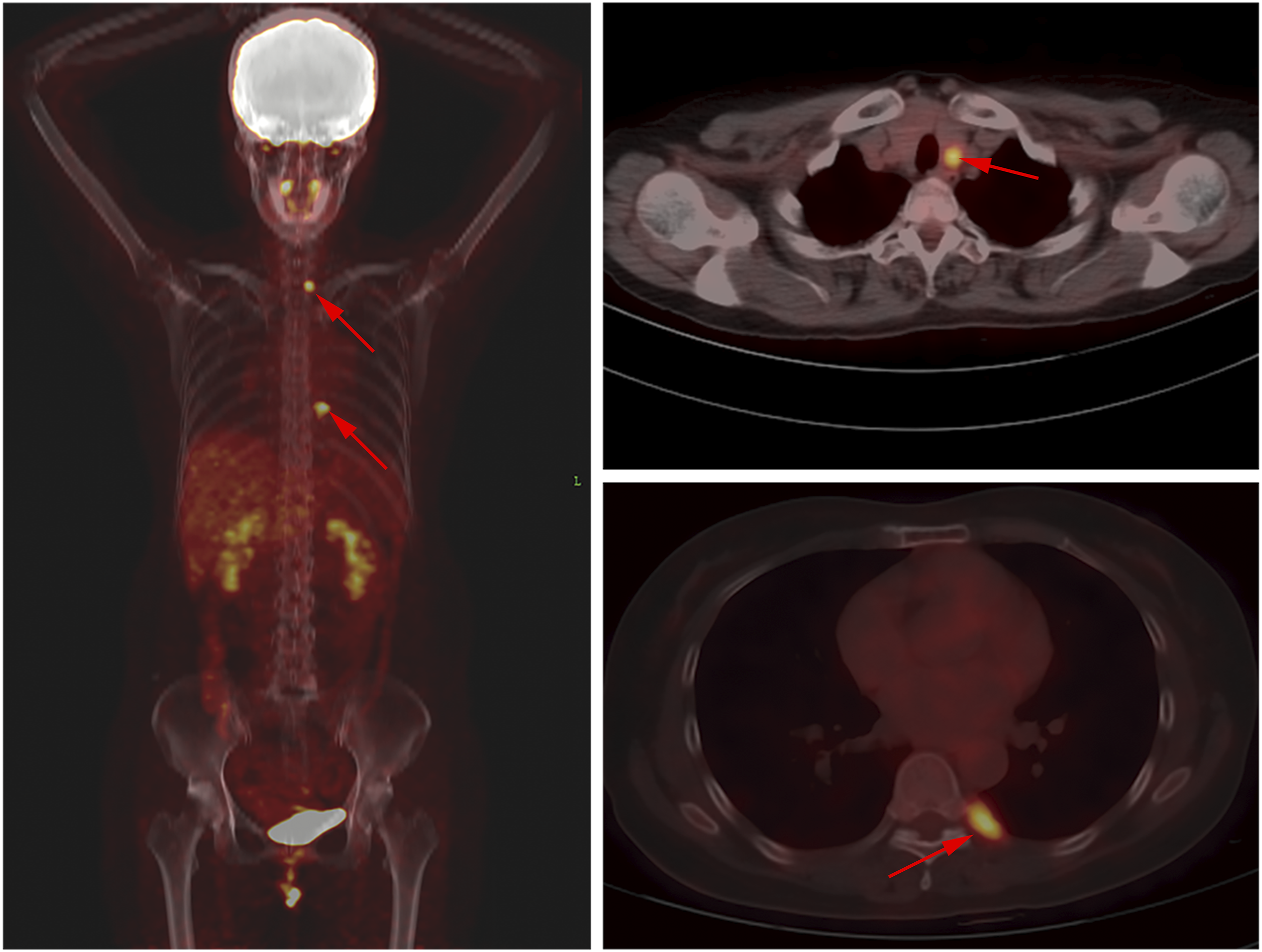
Postoperatively, the patient recovered well without complications. Conventional chemotherapy and regular follow-up were carried out after the operation. One year later, the patient was readmitted to the hospital with pancreatic metastatic lesions and died 1 month after surgery.
Discussion
Cervical cancer is the fourth leading cause of death in women, after breast, lung, and colon cancer worldwide, and is a global public health problem.7,8 The main routes of the metastasis are direct local extension and lymphatic metastasis. The most common sites of metastasis are the vagina, parametrium, and pelvic lymph nodes. 9 Distant hematogenous metastases are relatively rare and include the pancreas, lungs, and bones.10,11 Non-thyroidal metastases to the thyroid were infrequent, accounting for only 1.6% of all identified thyroid malignant tumors, performed by Stergianos et al. 12 There are 2 hypotheses to explain this phenomenon: the high iodine concentration and oxygen saturation in the thyroid tissue obstruct malignant cell growth and high-velocity arterial blood flow of the thyroid impedes adhesion and implantation of malignant cells. 13 The most common primary sites of thyroid metastasis are kidney, followed by breast and lung. Origin of cervix is extremely rare. 14
More than 95% of cervical tumors originate from epithelial cells, including squamous cell carcinoma (SCC), adenosquamous, and adenocarcinoma carcinoma. 15 Neuroendocrine neoplasms of the uterine cervix account for only .9%–1.9% of cervical cancers, which is a very aggressive NET.1,2 Mixed adenoneuroendocrine carcinomas, with the morphologically recognizable glandular epithelial and neuroendocrine phenotype, belong to NENs. 6 This case is the first to report MANECs as primary uterine cervical cancer metastasizing to the thyroid gland.
It is sometimes difficult to diagnose thyroid metastasis due to mostly asymptomatic and indistinguishable from primary tumors. It was reported that most patients presented with new or growing thyroid nodule, dysphagia, neck swelling, hoarse voice, and cough. 16 Ultrasonography with excellent diagnostic performances is the best diagnostic method for thyroid gland, although no specific feature diagnoses thyroid metastases. Typical ultrasonographic appearances of metastases to thyroid gland include no clear boundary and intra-nodular vascularization. 13 Two-Dimensional Shear Wave Elastography is a novel non-invasive diagnostic tool in evaluating of thyroid nodules, with the advantage of simultaneous anatomic B-mode US imaging. Several studies have shown good results of SWE combined with B-mode US in the evaluation of thyroid `nodules, with reports of higher elasticity in benign than that of malignant nodules.17,18 To investigate whether metastatic lesions have an effect on thyroid function, Chung et al. reported that most of the patients with non-thyroid metastases were euthyroid (87.6%) through reviewing 170 reports. 19 Hypothyroidism may associate with the tumor cells massive infiltration. 20
Ultrasound-guided fine-needle aspiration cytology (FNAC) of a thyroid nodule is a valuable method to make a definitive diagnosis of most thyroid nodules. Therefore, FANC is widely and successfully used as a screening tool for those thyroid nodules at high risk. 14 However, Chung et al. reported the false-negative rate of 28.7% for FNAC in the diagnosis of metastatic thyroid tumors. 19 In contrast to FNAC, CNB obtains more adequate tissue samples for histopathological diagnosis, including immunohistology, which could acquire more sensitive and less false negative diagnose than FNAC. In our case, the ultrasound–guided CNB results had provided an accurate preoperative diagnosis of thyroid lesions and helped to determine the optimal treatment regimen.
There are different opinions about surgical procedures for patients with metastatic thyroid tumors. Although no statistical differences were found in survival rates between subtotal and total thyroidectomy, in a review it was recommended that patients with small, multiple, bilateral nodules should be treated by total thyroidectomy to prevent tumor recurrence. 21 In addition, another review reported that patients who underwent thyroid lobectomy almost did not suffer tumor recurrence when the surgical tumor tissue margins were negative. So, there was no significant difference in survival rates and prognosis between subtotal and total thyroidectomy. 22 In our reported case, the patient subsequently underwent left hemithyroidectomy and isthmusectomy, as well as ipsilateral central neck lymph node dissection due to a solitary left thyroid nodule and localized pleural lesion without extensive distant metastases.
Conclusion
Thyroid metastasis from cervical cancer is extremely rare and is indistinguishable from primary tumors. Therefore, it is significant to improve the diagnosis rate of metastatic thyroid cancer, and if necessary, ultrasound–guided puncture biopsy can be utilized to further diagnose metastatic thyroid cancer.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.