
Abstract
Thyroid metastasis from cervical carcinomas is an extremely rare disease; therefore, only a few cases have so far been reported in the literature. Due to the lack of data and the heterogeneity of clinical cases, the percentage of patients affected by thyroid metastases eligible to undergo surgery is not easily predictable. This report describes a rare case of endometrioid adenocarcinoma metastasized to the thyroid gland. A 72-year-old woman was referred to the ENT department of our hospital (Ospedale Degli Infermi di Biella, Italy) presenting with dyspnea and rapidly worsening condition, in need of emergency surgery. The peculiarity of this case lies in the metastasis isotype rarity, in its voluminous dimension, and in its mediastinal localization, which required the intervention of a multidisciplinary team to establish successful treatment planning.
Keywords
Introduction
Metastasis to the thyroid gland is a rare clinical presentation in surgical practice. The incidence of primary non-thyroidal tumors which metastasize to the thyroid accounts for 1.4% to 3%, 1 probably owing to the high concentration of oxygen and iodine combined with the elevated arterial blood supply to the thyroid which may prevent tumor cells from anchoring and growing. 2
According to a recent Chinese study on secondary thyroid tumors, the most common sites of primary tumor reported in clinical series are lungs (20%), gastrointestinal tract (18.2%), breast (14.5%), and kidney (12.7%). 3 On the other hand, it seems that the disease affects the non-East Asian population in the same sites but with a different sickness rate: the most affected tumor location is kidney (41.57%), followed by lungs (11.61%), gastrointestinal tract (10.11%), and breast (9.36%). 4 Thyroid metastasis from cervical carcinomas is extremely rare; therefore, only a few cases have so far been reported in the literature.5-7
Due to the lack of data and the heterogeneity of clinical cases, the percentage of patients affected by thyroid metastases eligible to undergo surgery is not easily predictable. Dysphonia, dysphagia, hemoptysis, and stridor are among the most common signs in symptomatic patients; anyway, the lack of data in the literature complicates the evaluation of the incidence of symptomatology. 8 The percentage of patients presenting with thyroid metastasis, in need of tracheotomy due to dyspnea accounts for 3.6% 3 ; on the other hand, according to the literature, as many as 10% of patients die from disorders related to tracheal compression. 9
Because of the aggressive nature of the tumor, many of the patients who have been diagnosed with thyroid metastases are often treated with palliative intent. On the other hand, only selected patients are submitted to lobectomy or total thyroidectomy to achieve local control or search for a long-term cure. Some authors suggest performing thyroid lobectomy rather than total thyroidectomy, since this latter may minimize risks to laryngeal nerve and parathyroid glands; hence, it represents the least aggressive procedure. 8
Case Report
This report describes a rare case of endometrioid adenocarcinoma metastasized to the thyroid gland. A 72-year-old woman presenting with dyspnea was referred to the ENT department of our hospital (Ospedale Degli Infermi di Biella, Italy); her clinical condition was rapidly worsening; hence, an emergency treatment was necessary. The peculiarity of this case, which lies in the rarity of the metastasis istotype, in its voluminous dimension and in its mediastinal localization, required the intervention of a multidisciplinary team.
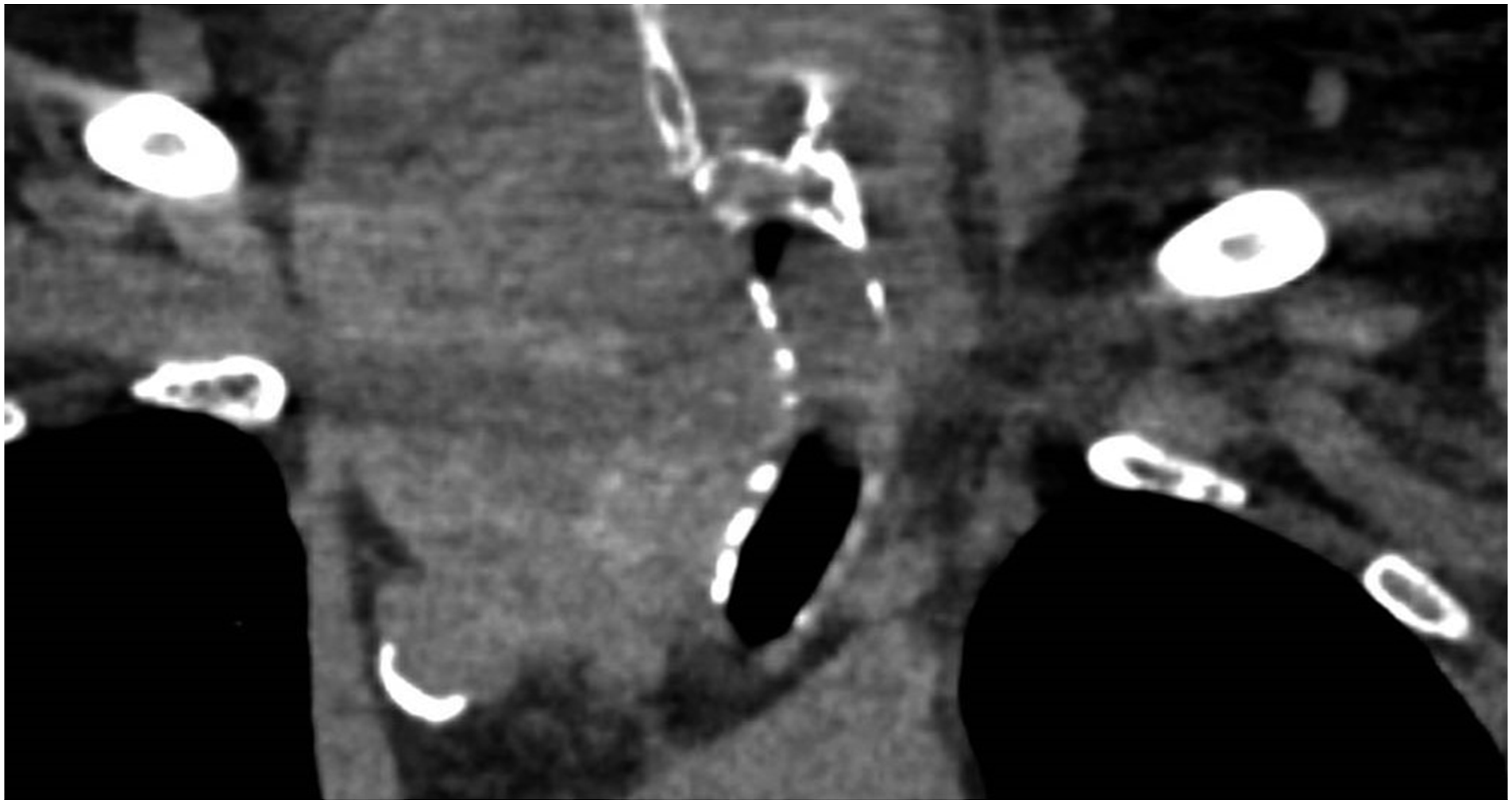
The patient had previously been diagnosed with high-grade endometrioid adenocarcinoma, as a result to which a hysterectomy and a subsequent RT had already been performed. At the time of admission to the ENT department, the patient claimed to suffer from dyspnea and respiratory fatigue during the previous weeks but rapidly worsening in the last 3 days. A laryngeal fibroscopy revealed the paralysis of the right hemilarynx with sufficient respiratory space at the glottic level, and a CT scan of the neck, urgently performed the same day, identified a mass in the region of the right thyroid lobe, with a maximum axial diameter of 69 mm, a craniocaudal extension of 65 mm, and a maximum anteroposterior diameter of 50 mm.
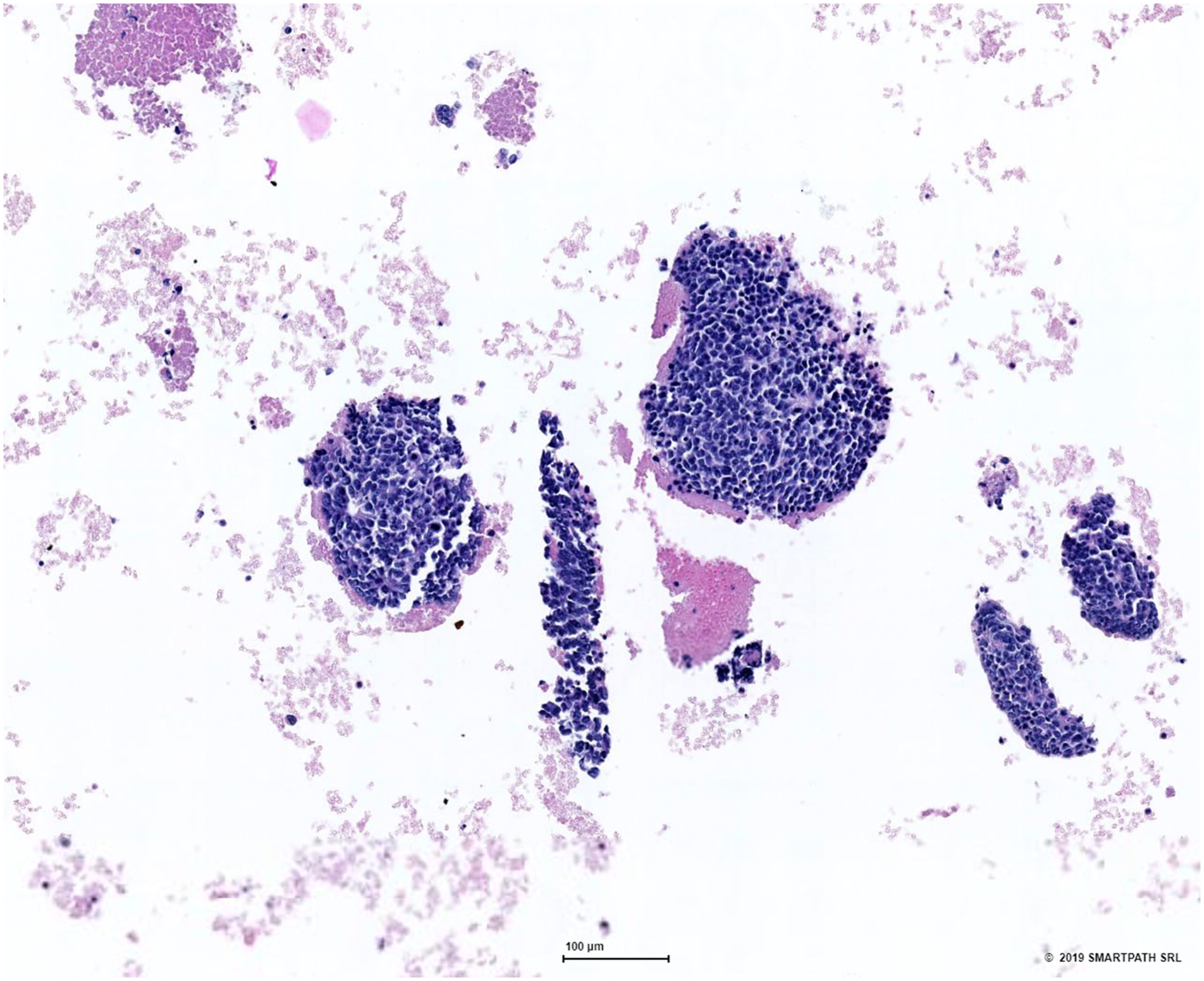
This lesion caused marked contralateral dislocation of the trachea with a reduced lumen at the cervico-mediastinal passage (Figure 1–2). The patient was then hospitalized and constantly monitored at the semi-intensive care unit. Afterward, the ultrasound-guided fine-needle aspiration reported the diagnosis of endometrial adenocarcinoma metastasis. (Figure 3) Computed tomography (CT) axial view showing the voluminous metastasis of the right lobe of the thyroid which displaces the trachea. Computed tomography (CT) coronal view showing the metastasis that occupies the mediastinum displacing the trachea. Microscopic findings of the tumor in the present case by fine-needle aspiration.
The case was subject to a multidisciplinary team analysis, and then the indication of a right thyroid lobectomy combined with sternotomy was identified as the optimal approach. The surgery was performed 2 days after the patient’s admission to the semi-intensive unit. Because of the surgical procedure, the patient’s dyspnea condition improved, and no intraoperative or postoperative complications occurred. A bronchoscopy performed on the third postoperative day revealed a clear widening of the lumen in the previously stenotic tracheal tract. Hence, the patient was discharged 5 days after the surgery.
During the 6 months of follow-up, the patient regularly reported good breathing; in addition, fibroscopy and bronchoscopy, routinely performed, revealed adequate respiratory space at the glottic and tracheal level. The thyroid localization of the endometrial adenocarcinoma was confirmed by the histological examination. Therefore, a new multidisciplinary team meeting was planned, and chemotherapy was identified as the optimal procedure to be performed.
Discussion
No international guideline specifies universal strategies to be adopted in case of thyroid metastases; hence, medical and surgical planning (thyroidectomy or tracheotomy) must be tailored differently from patient to patient. Decision-making, based on the patient’s best interest, must consider all the practicable chances, including the possibility of achieving long-term survival. 5
Thyroidectomy or tracheotomy should always be considered and suggested in case of compression caused by the metastases, to relieve symptoms and to improve the quality of life.
If dyspnea worsens due to tracheal compression, a tracheotomy may be the best choice for patients presenting with thyroid metastases without mediastinal involvement as it solves the respiratory distress and it could prevent the tumor from spreading; anyway, it does not contribute to prolonging the patient’s life. 9
In contrast, according to the literature review, CLND (central lymph node dissection) is not the suggested procedure since the rate of lymph node metastasis in patients treated with CLND accounts for just 3%.3,9
In the present case, a quick and reliable preoperative diagnosis was provided by fine-needle aspiration cytology, performed in accordance with the literature 10,11.
Since the metastasis had already reached the mediastinum, neither a tracheotomy nor a tracheal stenting would have resolved the dyspnea; therefore, a right thyroid lobectomy with sternotomy was practiced.
The patient was hospitalized at the semi-intensive care to be constantly monitored while waiting for fine-needle aspiration and TC results. In accordance with the literature, a thyroid lobectomy was performed rather than a total thyroidectomy since it represents the least aggressive procedure able to minimize risk to the laryngeal nerve and parathyroid glands. 8
Considering the rarity of the disease, particular attention should be paid to the diagnosis process to avoid any incorrect detection and consequent treatment. Prognosis will depend on multiple factors, including the site and volume of metastases, the course of primary disease, and any comorbidity. Given the complexity of the case, the communication between the specialists involved in the management of such cases is essential: it is ensured by modern multidisciplinary team management, involving endocrinologists, head and neck surgeons, oncologists treating the primary tumor, radiologists, and pathologists. The setting is complex, and decisions must be made considering the risks and benefits of the surgical procedure to reach the best-shared conclusion as quickly as possible.
Footnotes
Acknowledgments
We would like to thank Anna Lanza for her assistance in drafting and correcting the English language.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.