
Abstract
Synovial sarcoma (SS) comprises less than 1% of head and neck cancers, and less than five cases of adult primary tracheal SS have been described. This case describes a patient encountered at a community-based academic hospital, and retrospective chart review was performed for data collection. A woman in her forties presented with shortness of breath due to a superior mediastinal mass found to be an unresectable primary tracheal SS. Primary treatment resorted to curative-intent radiation therapy. Subsequent metastasis required systemic chemotherapy with pazopanib. To the best of our knowledge, this is the first reported case of this nature and adds to understanding the presentation, diagnosis, natural history, and treatment outcomes of primary tracheal SS. This case was exempt from review by the institutional review board and complied with privacy policy standards.
Introduction
Soft tissue sarcomas comprise approximately 1% of head and neck cancers, and synovial sarcoma (SS) comprises only a fraction of those cases. 1 Primary tracheal SS is exceedingly rare, with only 5 adult cases reported.2-5 Tumors are considered unresectable if they involve greater than half the length of the trachea or invade critical mediastinal structures, and their treatment resorts to primary radiation therapy (RT) rather than surgical resection. 1 We present a case of unresectable primary tracheal SS that subsequently metastasized and required systemic chemotherapy. Though the treatments were not novel in oncologic care, this case is unique among other reports of primary tracheal SS in that it was unresectable and metastasized after primary treatment. This case report presents the treatment response and survival outcome of previously undescribed unresectable primary tracheal SS.
Case Report
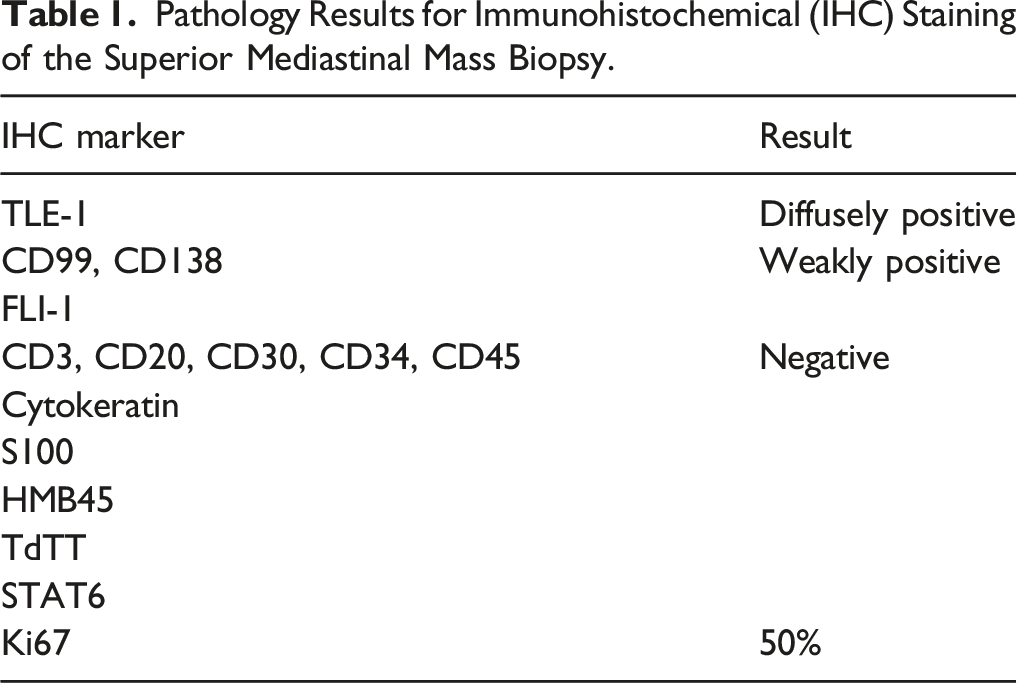
A woman in her 40s presented with worsening wheezing and shortness of breath. Workup included chest CT angiography that showed atelectasis of the left lower lobe and narrowing of the left main bronchus from a 36×30.3×40.3 mm superior mediastinal mass. The mass had irregular margins and central hypodensity suggestive of complex fluid or necrotic material (Figure 1). The patient was intubated before undergoing MRI that showed a 1 cm increase in mass size since imaging 5 years prior. Bronchoscopy identified a fungating, friable mass obstructing greater than 80% of the tracheal lumen. Cytology revealed a spindle cell neoplasm with necrosis, and pathology showed a malignant round blue cell neoplasm. Histopathologic and immunohistochemical staining showed a poorly differentiated SS (Table 1). Fluorescence in-situ hybridization panel and molecular marker results were negative for SS18 and EWSR1. However, a genetic fusion panel showed the pathognomonic SS18-SSX fusion on next generation sequencing analysis, confirming the diagnosis of SS. The tumor was unresectable due to mediastinal extension, and the patient underwent repeat debulking with tracheal stent placement before extubation and discharge. Initial metastasis workup was unremarkable, and she completed curative-intent RT using a total dose of 50 Gray (Gy) at 2 Gy/fraction with restoration of the airway diameter. Two months later, PET CT showed bone and lung metastasis, and the patient began systemic therapy with pazopanib 400 mg daily 8 months after initial presentation. Chest X-ray (A) and CT scan (B,C) with a yellow arrowing indicating the superior mediastinal mass. Pathology Results for Immunohistochemical (IHC) Staining of the Superior Mediastinal Mass Biopsy.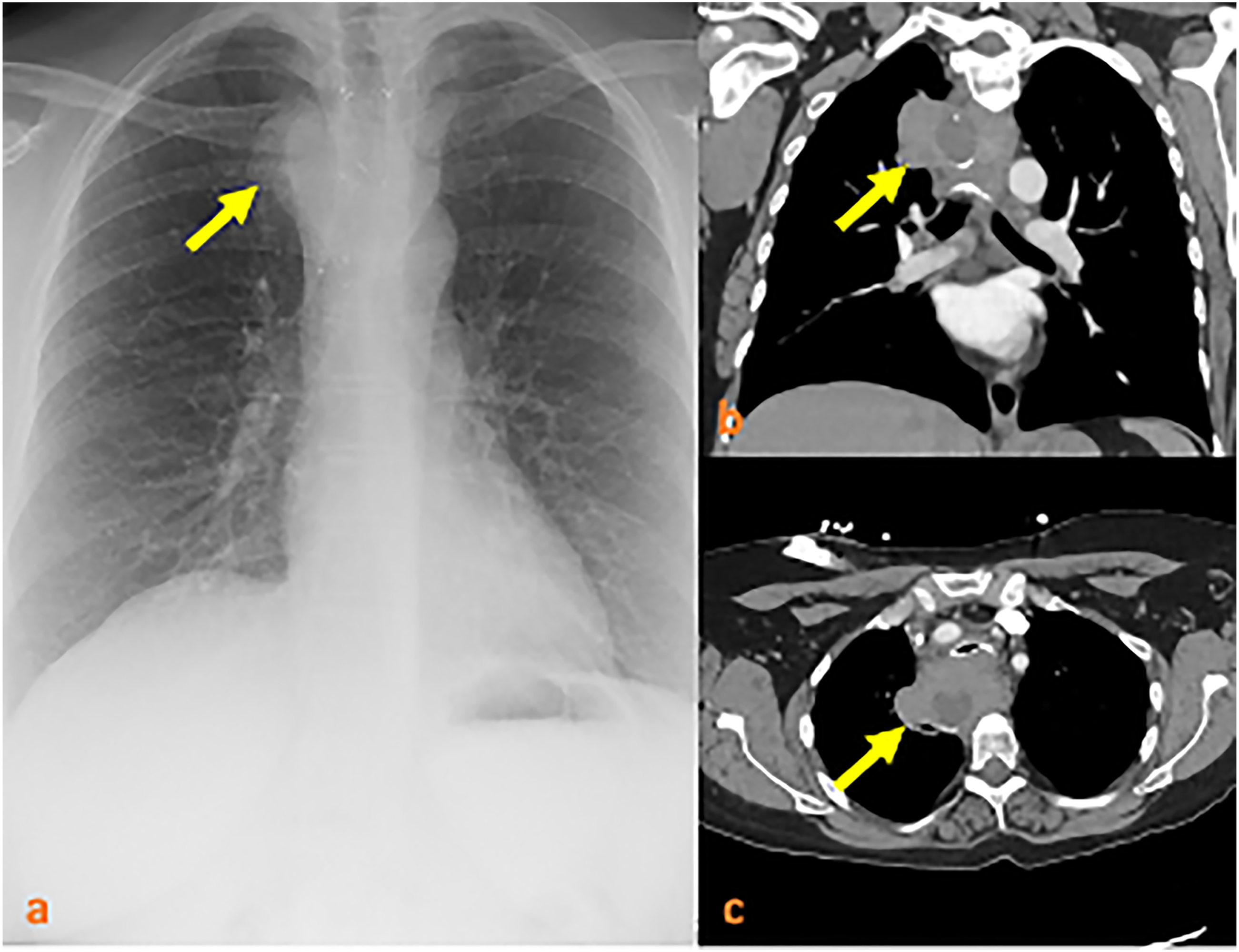
Discussion
To the best of our knowledge, this case presents the first documented unresectable primary tracheal SS. Primary tracheal SS is exceedingly rare, and no treatment guidelines currently exist. However, surgical resection is the treatment of choice for other head and neck sarcomas, with adjuvant RT reserved for recurrent or intermediate- to high-grade tumors. 1 Treatment of unresectable cases includes RT and confers a worse prognosis than treatments including surgery. 1
Current literature on primary tracheal SS suggests that treatments used in other head and neck sarcomas are effective. Corrales et al. (2011) and Kumar et al. (2020) report cases of primary tracheal SS in 48-year-old and 26-year-old women, respectively. Both underwent surgical resection and maintained locoregional control without metastasis for 1 year.2,3 Sykes et al. (1997) described primary tracheal SS in a 20-year-old man who underwent surgical resection and 62 Gy of external beam RT and remained well 8 months post-op. 4 Ye et al. (2020) report primary tracheal SS in a 19-year-old man treated with surgical resection and 63 Gy of adjuvant proton beam therapy who remained without recurrence for 18 months. 5
Ultimately, current literature suggests that treatment protocols for other head and neck sarcomas confer a reasonable prognosis in primary tracheal SS. The mediastinal invasion of our patient’s tumor deemed it unresectable, and treatment resorted to RT. Despite excellent initial response, the tumor metastasized and required systemic chemotherapy. This case presented the first of unfavorable outcomes reported in primary tracheal SS. There are no guidelines for the treatment of primary tracheal SS, though surgical resection could be considered the treatment of choice and is supported by favorable outcomes in reported cases. This case presented an unresectable primary tracheal SS that initially demonstrated favorable response to second-line therapy but subsequently metastasized and required systemic treatment. It contributes to the understanding of the presentation, diagnosis, natural history, and treatment outcomes of primary tracheal SS.
Footnotes
Authors Contributions
Joann M. Butkus: study design, data collection, analysis, and article writing/editing.
Mackenzie Kramer: study design, data collection, and article writing/editing.
Daniel Eichorn: data collection and article writing/editing.
Ali Raza R. Shaikh: data collection.
Rajesh R. Patel: article writing/editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This report was exempt from review by Thomas Jefferson University’s institutional review board and complies with all privacy policy standards.