
Abstract
Hydatidosis is a chronic zoonotic infection of humans caused by the infestation of larvae of the tapeworm Echinococcus granulosus. All parts of the body can be infected, especially the liver and lungs. Intraorbital hydatid cyst (HC) is a rare entity and accounts for less than 1% of all hydatid cysts. Total resection of the cyst can be very challenging due to the limited area within the orbit and the severe adhesion to adjacent structures. Several surgical approaches have been described in the literature depending on the size and location of the cyst. We reported a case of retrobulbar HC in a 10-year-old boy which was completely resected using the Lynch approach. Our case should be the second reported case from Syria and the first case that used the Lynch approach in the literature.
Introduction
Hydatidosis is a chronic parasitic helminthic disease that leads to the formation of cysts. 1 It most commonly affects children and adolescents in rural areas. 2 The pathogen is Echinococcus granulosus. Dogs are the definitive hosts, while intermediate hosts are sheep. During the parasitic cycle, humans can be accidental intermediate hosts.2,3 Hydatid cyst (HC) can form in almost all parts of the body and remain asymptomatic for a long period of time until it becomes large enough to compress adjacent elements. 4 However, the formation of HC within the orbit is very rare and accounts for less than 0.8 to 1% of all cases of hydatidosis. 2 Intraorbital HC usually presents with proptosis, visual impairment, ocular motility disturbance, and chemosis. 5 In this paper, we report a case of intraorbital HC that was surgically removed using the Lynch approach. To the best of our knowledge, this case should be the second intraorbital HC reported from Syria and the first one to use the Lynch approach in the literature.
Case report
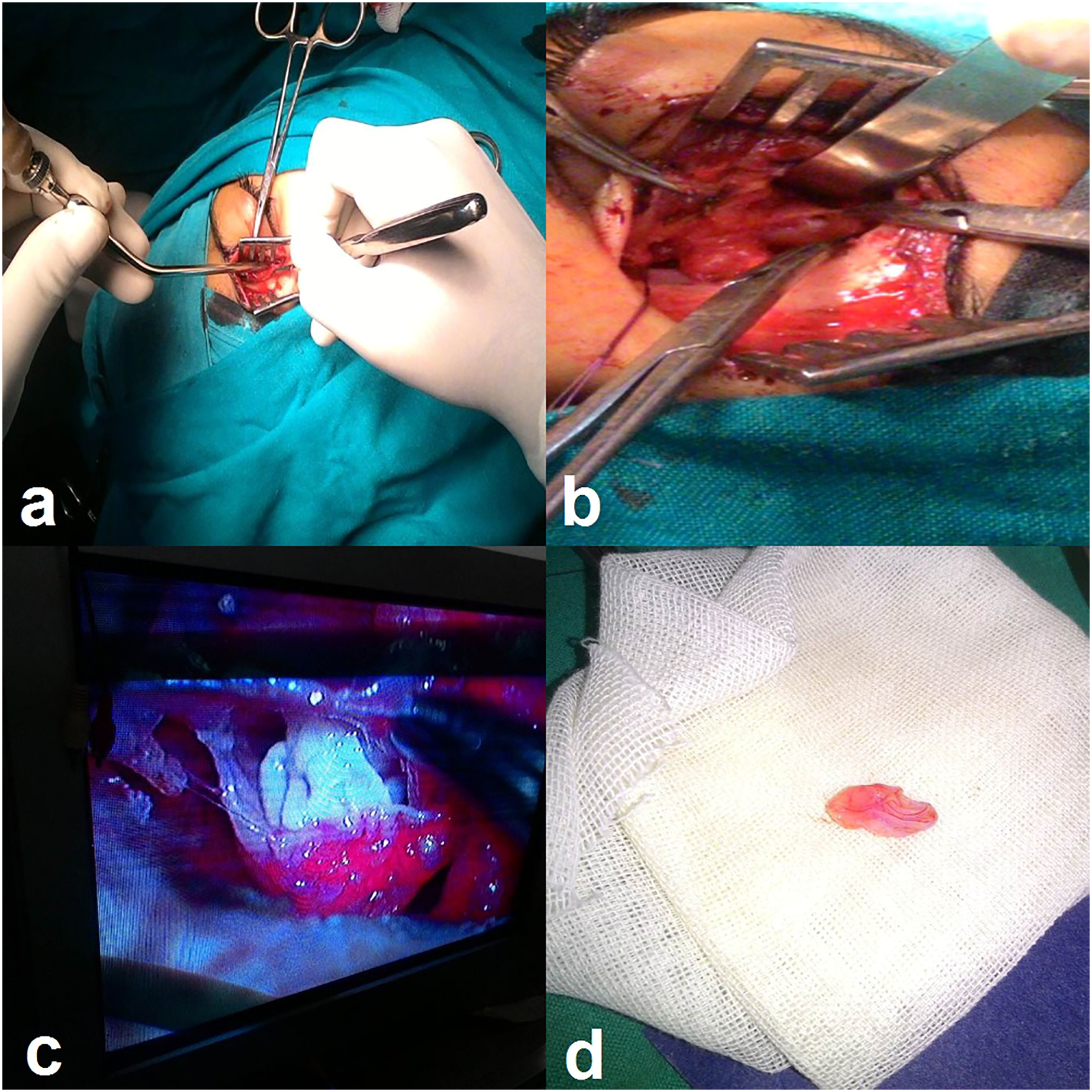
A 10-year-old Caucasian boy came to our ENT clinic with a history of progressive painless proptosis and diplopia with decreased vision in the left eye for 3 months. The patient lived in the eastern regions of Syria where there was frequent contact with sheep and dogs. When reviewing his medical history, we found that one of his relatives was affected by HC in the brain. On the ophthalmologic evaluation of the left eye, visual acuity was 5/10 and fundus examination showed swelling of the optic disc. The measurement of exophthalmos using the Hertel exophthalmometer was 28 mm. Eye movement was restricted in adduction and elevation. The evaluation of the right eye was within normal limits. Magnetic resonance imaging (MRI) revealed a left retrobulbar cystic lesion with regular margins located between the optic nerve and the medial rectus muscle compressing the optic nerve. The cyst measured about 27 × 19 × 18 mm and was hypointense in the T1-weighted images (T1WI) and hyperintense in the T2-weighted images (T2WI) with hypointense in the FLAIR images and hyperintense in the STIR images (Figure 1). Paranasal-orbital computed tomography (CT) showed a well-defined cystic lesion with a homogeneous component and without bone erosion in the orbital walls. Laboratory tests were unremarkable. The chest radiograph and abdominal ultrasound showed no abnormalities. We decided to resect the cyst using the Lynch approach (Figure 2). Therefore, we made a curve skin incision placed approximately halfway between the bridge of the nose and the medial canthus. Then, a subperiosteal flap was elevated until we reached the retrobulbar region. We opened the periorbita and incised the retrobulbar fat. Unfortunately, the cyst was punctured during dissection. Finally, a complete eradication of the cyst membrane was performed (Figure 2). A heavy washing with hypertonic serum was performed to reduce the spread of hydatidosis. Pathological examination of the resected cyst confirmed the diagnosis of HC. The proptosis disappeared immediately after resection of the cyst. Visual acuity improved to 7/10 and then to 10/10 on the third and fifth postoperative days, respectively. The patient was discharged home after 7 days of surgery with a prescription of albendazole (15 mg/kg/day administered in divided doses q12 hr for 1 month). Unfortunately, we were unable to follow the patient due to the war conditions in Syria. MRI images in the T1 (a), T2 (b), FLAIR (c), and STIR (d) sequences reveal a well-defined cystic lesion in the retrobulbar region. Intra-operative photographs show the surgical incision using the Lynch approach (a, b, c) and the resected hydatid cyst (d).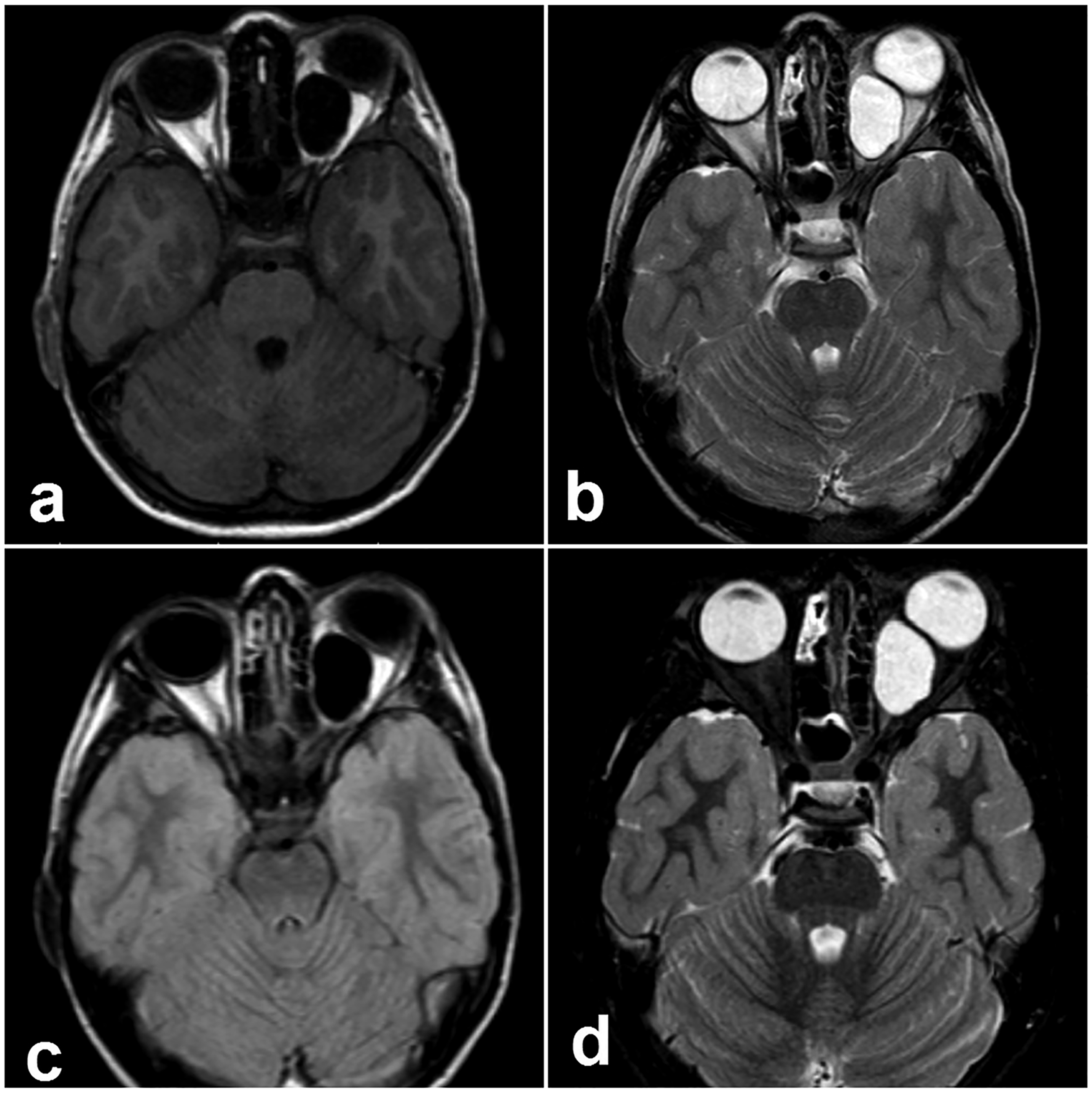
Discussion
Hydatid disease is a zoonotic infection of humans caused by the infestation of larvae of the tapeworm Echinococcus granulosus.6,7 All parts of the body can be infected with Hydatidosis. The liver and lungs are the most frequently affected organs.4,8 Orbital involvement is a very rare entity and accounts for less than 1% of hydatid cysts. However, in endemic areas, HC is the second most common cystic lesion of the orbit after dermoid cyst. 4 Primary intraorbital HC is very rare. However, it is generally formed as a secondary cyst after spreading from another organ of the body through a portal or systematic circulation.5,9 Regarding our case, it was a primary cyst since no involvement was found in other parts of the body. The formation of the intraorbital HC in the left orbit is more common than in the right orbit, and this is consistent with our case. 5 Intraorbital HC tends to be asymptomatic and slowly progressive until it reaches a large volume and compresses adjacent elements. Therefore, symptoms such as painful proptosis, visual loss, chemosis, palpebral edema, restriction of extraocular movements, and orbital cellulitis can become clear.3,4,10 However, proptosis in our patient was painless, nonaxial, and irreducible. MRI and CT are the most used imaging modalities for the evaluation of HC. On MRI, the cysts reveal low signal intensity on T1WI and high signal intensity on T2WI. However, the MRI characteristics can vary depending on the development phase of HC (viable/ infected /dead). Therefore, in some cases, the diagnosis can only be made by histopathology.5,8 The cornerstone of intraorbital HC management is total resection of the cyst without rupture of its membrane and with albendazole administration to reduce the chance of recurrence or dissemination. However, we could not eradicate the cyst without rupture due to its severe adhesion to adjacent structures. The preference surgical approach depends on the size and location of the HC within the orbit. Several approaches have been described in the literature including fronto-orbitozygomatic, simple enucleation, lateral orbitotomy, subciliary incision, and transcranial.5,9 We used the Lynch approach, which is a very difficult approach to eradicate the cyst, and this case can be the first case report to use such an approach. In conclusion, intraorbital HC is a rare entity, and physicians should keep these cases on the list of differential diagnoses for orbital cystic lesions. Complete resection of the HC without rupture of its membrane is crucial in reducing the chance of recurrence or dissemination.
Footnotes
Acknowledgements
The authors acknowledge the patient and his parents for their cooperation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Written informed consent was obtained from the patient’s parents to publish this case report.