
Abstract
Intraosseous hemangiomas usually occur in the vertebrae and skull bones, whereas those arising within the nasal cavity are exceedingly rare. Here, we describe the case of a 40-year-old woman with nasal congestion who presented to our hospital with a tumor located in the left nasal cavity. Unenhanced paranasal computed tomography revealed an approximately 3 cm large mass originating from the anterior wall of the ethmoid sinus. Pre-operative imaging failed to reveal the etiology of the mass. The tumor was successfully resected using a trans-nasal endoscopic approach without pre-operative embolization. No complications occurred during the post-operative period, and there was no evidence of recurrence at the 3-month and 6-month follow-up. Histological examination of the resected specimen showed endothelium-lined blood-filled vascular spaces within the bony trabecule, suggesting a pattern typical of intraosseous cavernous hemangioma. Thus, although intraosseous hemangiomas of the nasal cavity are extremely rare, they must be considered when a bony mass is detected in the nasal cavity.
Introduction
Hemangiomas found in bones are referred to as intraosseous hemangiomas and they are located primarily in the vertebral column and skull bones. 1 In contrast, intraosseous hemangiomas of the nasal cavity are extremely rare. 2 Several cases of intraosseous hemangiomas arising from the nasal turbinate, ethmoidal sinus, and maxillary sinus have been reported in the literature.1–14 Here, we present a case of nasal intraosseous cavernous hemangioma in a 40-year-old woman with nasal obstruction as the only complaint. Based on histo-pathological examination, the nasal mass was diagnosed post-operatively as an intraosseous cavernous hemangioma. The diagnostic challenges and management of this rare lesion are discussed.
Case report
The patient provided informed written consent for the use of personal information. A 40-year-old woman presented to the ear, nose, and throat (ENT) department with complaints of a 2-month history of nasal congestion on the left side. Other symptoms such as post-nasal drip, rhinorrhea, decreased sense of smell, fever, unintentional weight loss, headaches, and epistaxis were absent. She had no history of facial trauma or nasal surgery.
Physical examination revealed localized swelling in the external nose. Unenhanced paranasal CT and 3D reconstruction showed an approximately 3 cm large mass originating from the left anterior ethmoid sinus (Figure 1A, B, C). Anterior rhinoscopic examination revealed a firm, smooth erythematous mass with an intact surface that almost completely obstructed the left nasal cavity (Figure 1D). No other specific findings were evident upon examination of the head and neck. No erosion or destruction was observed in the surrounding tissues. Since the mass was pre-operatively considered a benign tumor, magnetic resonance imaging (MRI) and embolization were not performed. Computed tomography axial (A) coronal (B) view, and 3D reconstruction showing the ethmoid mass (C) Rhinoscopy revealed a firm, smooth erythematous mass with intact surface appearance that completely obstructs the left nasal cavity (D) intra-operative view of the trabecular bone debris within the mass itself (E) view of the nasal cavity after complete surgical excision of the mass (F) Part of the final specimen (G) bar = 1cm; H&E-stained sections demonstrating blood-filled vascular channels intermixed with thin strips of mature trabecular bone, as the characteristic of intraosseous hemangioma (H, I).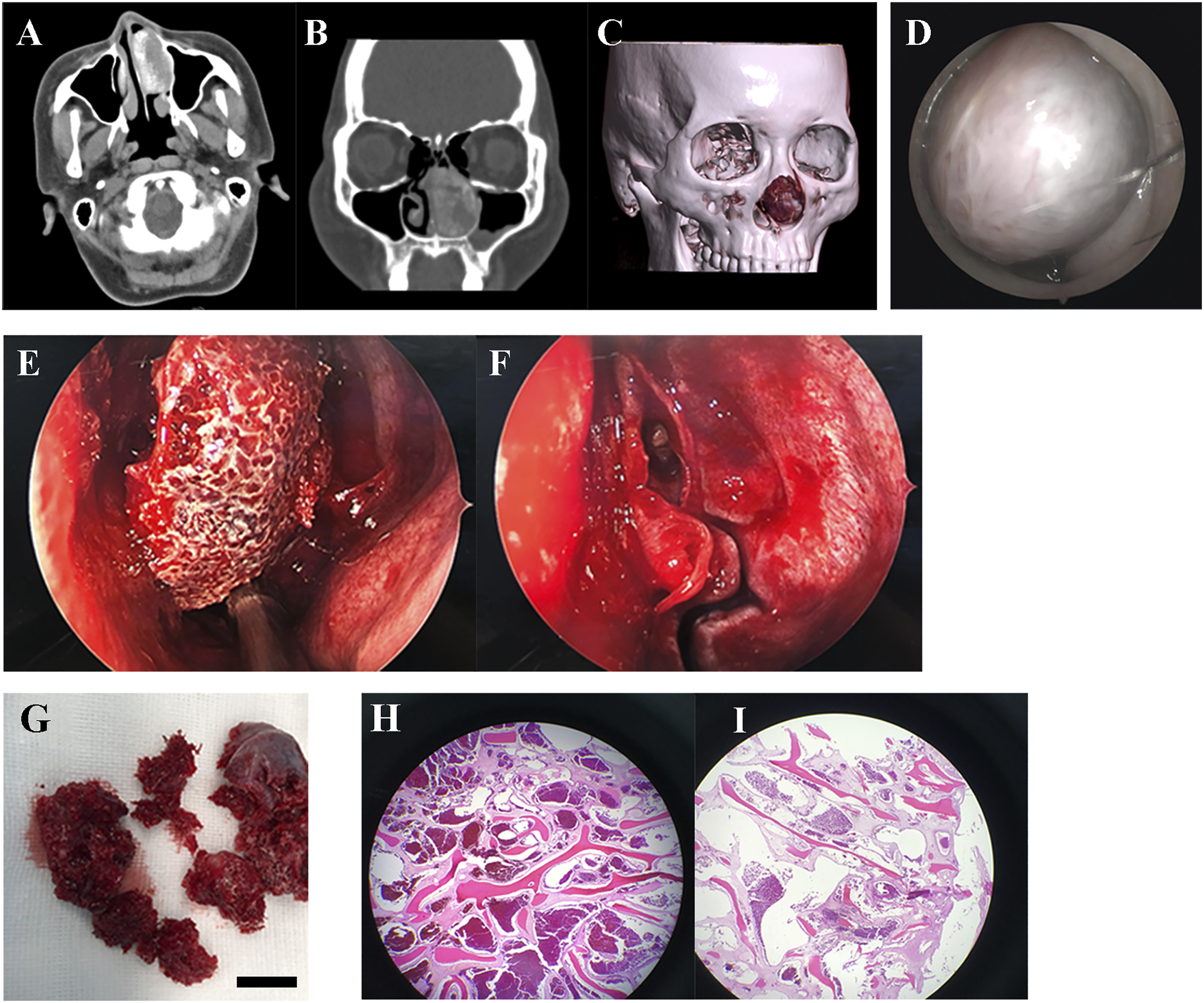
Endoscopic sinus surgery was performed under general anesthesia. The vascular appearing mass was attached to the anterior wall of the ethmoid sinus (Figure 1E). The tumor was complete resected en bloc (Figure 1F). Part of the final specimen is showed in Figure 1G and the cut surface of the tumor was grossly honeycombed. After excision, the nasal cavity was packed with a Merocel pad, which was removed on the third post-operative day. Intra-operative blood loss was <50 mL. No complications occurred during the post-operative period, and there was no evidence of recurrence at either the 3-month or 6-month follow-up. Histological examination revealed large dilated blood-filled vascular channels intermixed with background fibrotic stroma and thin strips of mature trabecular bone, consistent with a diagnosis of intraosseous cavernous hemangioma (Figure 1H, I).
Discussion
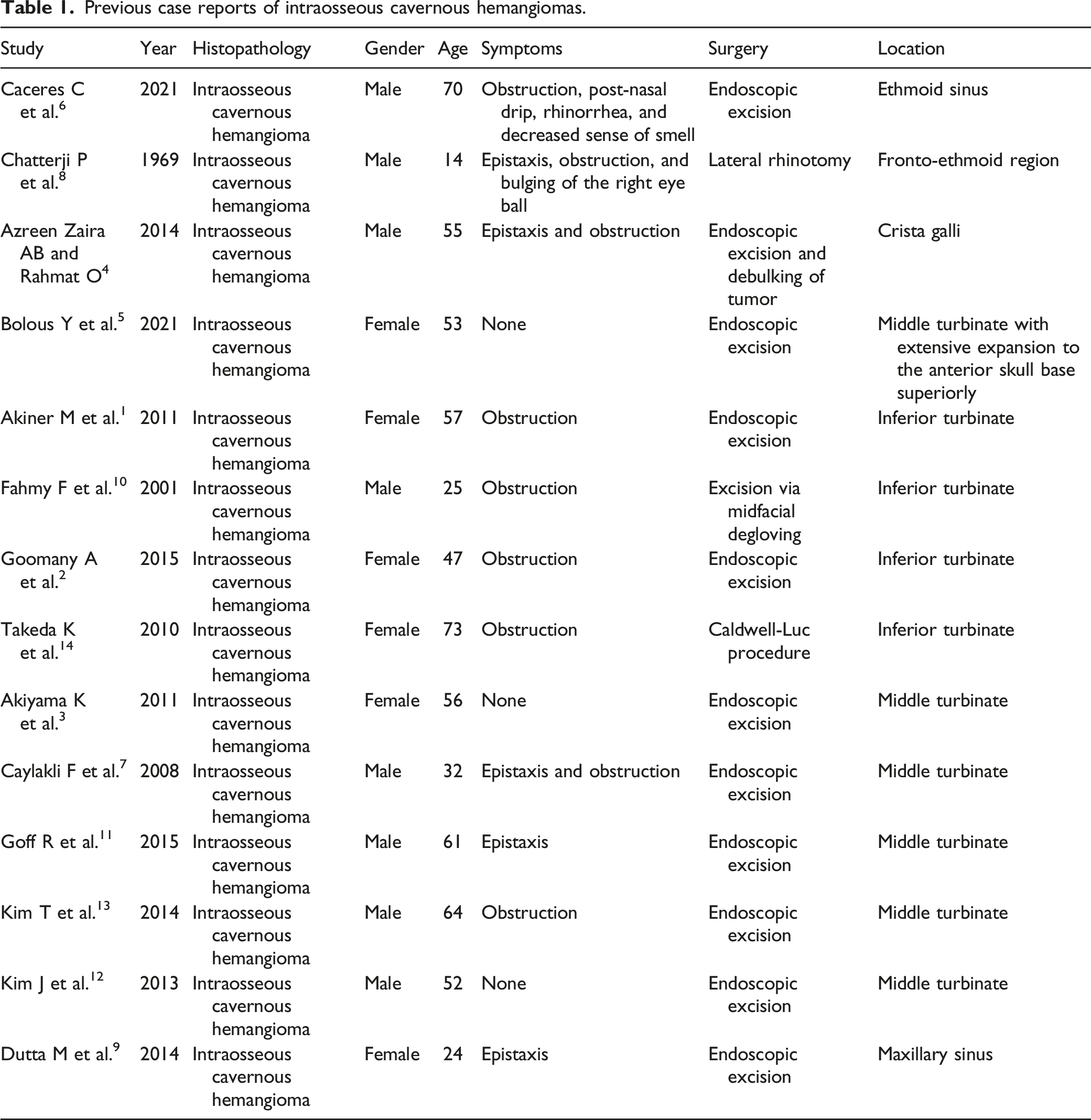
Previous case reports of intraosseous cavernous hemangiomas.
Almost all intraosseous hemangiomas of the skull are of the cavernous type. In addition, most cavernous hemangiomas occur in women at 40–50 years of age. 16 The etiology of intraosseous cavernous hemangioma is not fully understood. Local trauma and menopause have been proposed as possible causes, though a causal relationship has not yet been conclusively established.14,15 The patient in this case was a 40-year-old woman who had no history of facial trauma or nasal surgery.
The diagnosis of intraosseous hemangiomas is very difficult, since they often present as a slowly enlarging, hard mass, with the patient often remaining asymptomatic until the tumor becomes large enough. 3 In a previous case report of intraosseous hemangioma of the ethmoid sinus, the patient complained of nasal obstruction, post-nasal drip, rhinorrhea, and anosmia. 6 In contrast, the only presenting complaint in our patient was nasal obstruction. CT scans are helpful in establishing a diagnosis since intraosseous hemangiomas have a characteristic “honeycomb” appearance of the cavernous spaces within the lesion, and a “sunburst” pattern of radiating trabeculations. 17 Other radiographic examinations are also helpful in diagnosing intraosseous hemangiomas. MRI is useful to further define the extent of invasion into surrounding tissues and to detect intracranial, intra-orbital, or perineural extension. 8 Angiography typically shows increased vascularity in the tumor area. 14
Common treatment options for nasal cavity intraosseous hemangiomas include surgery, radiotherapy, sclerotherapy, and embolization. Complete surgical excision with margins of sound uninvolved bones is the treatment of choice and has been adopted in most cases. 18 In addition, an endoscopic approach should be used once appropriate to minimize the extent of surgical invasion. 3 Radiotherapy is also an effective treatment therapy for hemangiomas; however, long-term side effects, including malignancy, region growth impairment, and scarring, render it reserved only for unresectable lesions. 7 Pre-operative embolization and sclerotherapy have been reported to reduce intra-operative bleeding; however, these are palliative procedures 5 and are not necessary when complete surgical resection can be performed. 3
In summary, we report a rare case of intraosseous hemangioma arising from the ethmoid sinus. The mass was excised en bloc using an endonasal endoscopic approach without any complications or recurrence. Although intraosseous hemangiomas of the nasal cavity are extremely rare, they must be considered when a bony mass is detected in the nasal cavity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was reviewed and approved by the Independent Ethics Committee of Minhang Branch, Zhongshan Hospital, Fudan University (2022-053-01K) and conducted in compliance with the Declaration of Helsinki.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available since the medical records and data are the patient’s privacy, but are available from the corresponding author on reasonable request under the consent of the patient.