
Abstract
Background:
We report a case of an intraosseous cavernous hemangioma originating from the middle turbinate that expanded into the anterior skull base, without traversing the cribriform plate.
Methods:
The mass was found incidentally after a computed tomography head was ordered for unrelated reasons. On questioning, the patient denied any nasal symptoms. Magnetic resonance imaging showed an enhancing mass and the radiological imaging supported a broad differential.
Results:
The lesion was removed by endoscopic image-guided surgery, and the pathology was that of a benign intraosseous cavernous hemangioma. There was no residual hemangioma on postoperative imaging and the nasal mucosa healed well. This is the first report of an intraosseous cavernous hemangioma of the middle turbinate showing superior expansion to the anterior skull base.
Conclusion:
This case demonstrates the extent to which cavernous hemangiomas may expand into surrounding tissues. While these lesions are uncommon, they can be considered as part of a broad differential diagnosis of sinonasal tumors.
Keywords
Introduction
Vasoformative tumors are a broad spectrum of neoplasms that can be benign or malignant. Hemangiomas are benign localized tumors originating from vascular endothelium. 1 These are further subdivided by the size of the proliferating vascular spaces from smallest to largest: capillary, cavernous, and cellular. The pathologic appearance of cavernous hemangiomas has been described as large, dilated, blood filled spaces with a flattened endothelial lining. 2 Pathologic diagnosis of these lesions is important in order to rule out malignant vasoformative tumors with similar features such as angiosarcoma or spindle cell hemangioma. Sinonasal hemangiomas are uncommon. They are estimated to comprise 12.5% of all head and neck hemangiomas and about one-third of these are cavernous hemangiomas. 3 Here, we present the first case of an intraosseous hemangioma of the middle turbinate with extensive expansion superiorly to the anterior skull base.
Case
The patient provided informed written consent to use their personal information. Ethics approval was obtained from the Nova Scotia Health Authority Research Ethics Board. A 53-year-old female was referred to the Otolaryngology—Head and Neck Surgery clinic for a large hyperdense nasal mass found incidentally on computed tomography scan following blunt head trauma due to a fall. The mass filled the left nasal cavity, extending superiorly to the left cribriform plate. The patient denied nasal obstruction, discoloration of nasal discharge, or epistaxis. They also denied headache, facial pressure, or visual changes. She is known to have significant loss of vision since childhood in her right eye following a traumatic injury. Anterior rhinoscopy revealed a mass obstructing the left nasal passage. Nasal endoscopy revealed a smooth mass obscuring or encompassing the middle turbinate. Her physical examination was otherwise unremarkable.
To rule out invasion of the skull base, the patient was scheduled for a magnetic resonance imaging (MRI) with gadolinium enhancement. The mass was isointense to skeletal muscle on T1-weighted imaging and hyperintense on T2-weighted imaging. The mass showed intense enhancement with gadolinium (Figure 1). The superior aspect of the mass contacted the cribriform plate on the left, but there was no evidence of dural involvement. The differential diagnosis on the MRI report included inverting papilloma and carcinoma; our concern was that this could also be an esthesioneuroblastoma or a hemangiopericytoma.
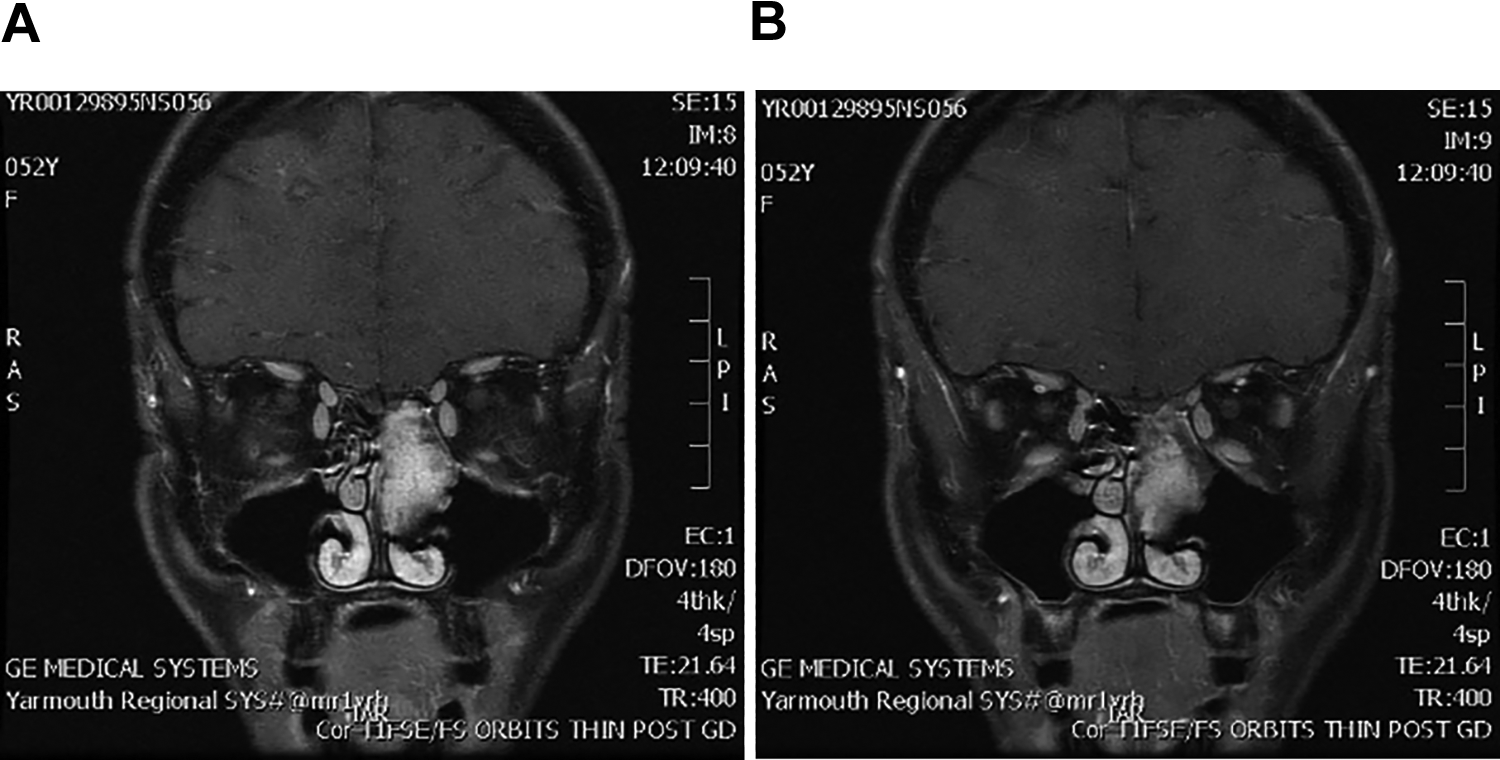
A and B, T1-weighted post-gadolinium contrast coronal MRI showing an enhancing left nasal mass reaching up to the cribriform with no evidence of breach or dural enhancement. MRI indicates magnetic resonance imaging.
Because of concern that the mass may be highly vascular (by its marked enhancement on MRI) as well as its close contact to the cribriform plate, the patient was consented to an endoscopic image-guided excision with possible repair of cerebrospinal fluid (CSF) leak if the dura were breached.
Intraoperatively, a markedly enlarged left middle turbinate was visualized endoscopically when the patient was placed under general anesthesia (Supplementary Figure 1). The mass was extending superiorly flush with the cribriform plate but not invading or deforming it. The mass was excised by sequential superior, posterior, medial, and lateral incisions. The superior attachment was cauterized then incised leaving a few millimeters below the skull base. No CSF leak was encountered intraoperatively. The mass was freed after ensuring hemostasis by cauterizing its vascular posterior pedicle near the sphenopalatine foramen. A left ethmoidectomy was necessary in order to reach around the markedly expanded turbinate. There was minimal blood loss. The remainder of the expanded turbinate was then crushed and removed piecemeal as it was not possible to deliver it intact through the left nostril. Uncinectomy was done to expose the maxillary sinus ostium.
Histopathologic examination showed multiple fragments of tissue with an extensive proliferation of thin-walled vascular structures and underlying thin fibrous septa, surrounding trabecular bone, in keeping with intraosseous cavernous hemangioma (Figure 2). There was neither endothelial cell atypia nor mitotic activity to suggest a malignant process. Some overlying intact nasal mucosa was identified.
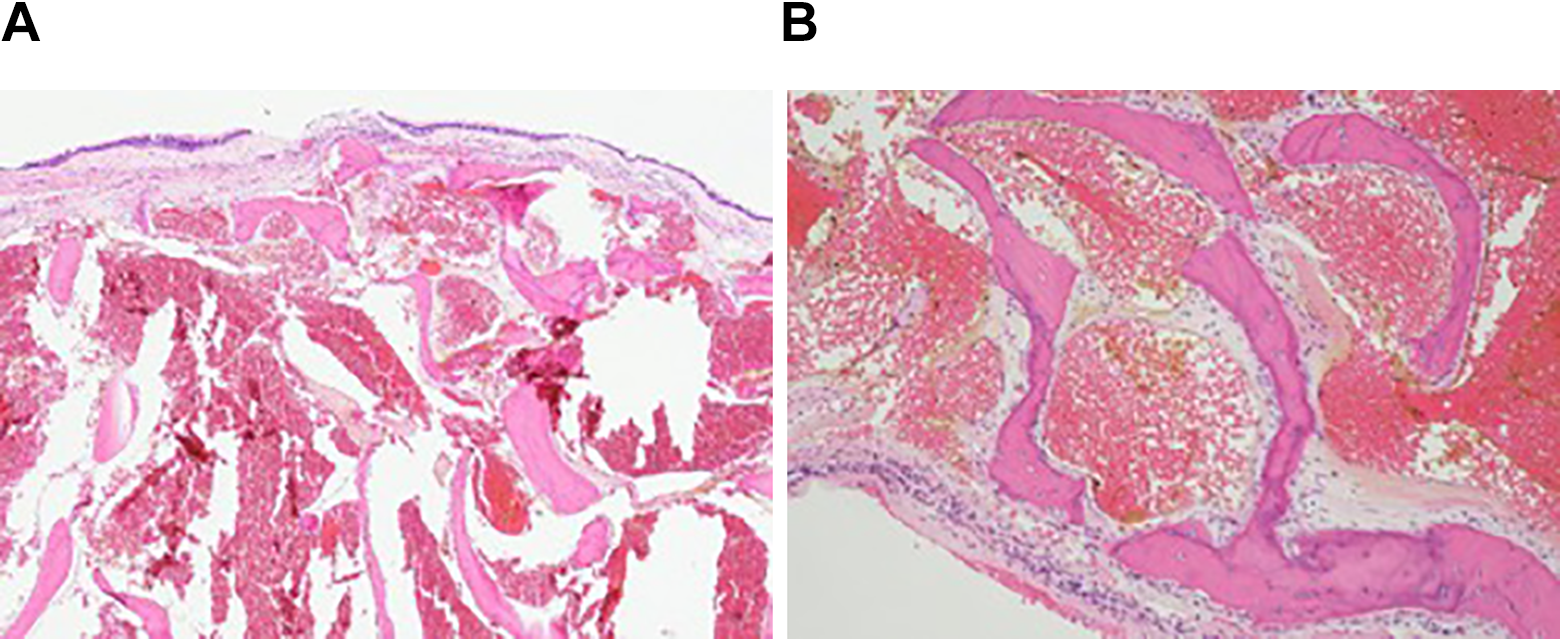
A, Low power photomicrograph showing numerous dilated vascular spaces, packed with red blood cells and intervening fragmented trabecular bone. Note the overlying intact respiratory mucosa in the upper part of the field (H&E, ×40). B, Higher power image showing bone surrounding dilated thin-walled blood vessels, with a flattened, benign endothelial lining (H&E, ×100).
The patient recovered from surgery with no complications, only nasal obstruction that resolved. She was relieved to learn that the lesion was benign and that it was completely excised. Upon follow-up, the middle turbinate stump completely healed with no evidence of scabbing or scarring.
Discussion
Previous cases have been reported of cavernous hemangiomas originating from the inferior turbinate,4-7 middle turbinate,8-12 maxillary sinus, 13 and nasal septum.14,15 Small case series reveal that the nasal septum and inferior turbinate may be the most common sites of origin.3,16 These sinonasal lesions are unified by presentation with nonspecific symptoms, namely epistaxis or nasal obstruction and possibly by association with trauma.8,17 The cavernous hemangiomas previously reported as originating from the middle turbinate were localized producing septal deviation and remodeling of the maxillary antrum. Our case is the first showing extensive superior expansion, reaching the anterior skull base. Esthesioneuroblastoma and hemangiopericytoma were considered in the differential of this mass. The proximity of the tumor to the cribriform plate supported the presumptive diagnosis of esthesioneuroblastoma. These tumors arise from the olfactory epithelium and typically present with nasal obstruction. 18 Additionally, the significant vascularity of this tumor in this case was consistent with a diagnosis of hemangiopericytoma which are typically slow-growing and exhibit few symptoms. 19 We recognize that preoperative palpation of the mass in clinic may have been beneficial in showing its bony consistency. This was avoided, however, for fear of causing significant bleeding considering the enhancement of the mass on MRI. 20
Conclusion
This case represents a unique presentation of a cavernous hemangioma of the middle turbinate that reached the anterior skull base. While sinonasal cavernous hemangiomas are uncommon, they can be considered part of a broad differential for sinonasal masses.
Supplemental Material
Supplemental Material, sj-docx-1-ear-10.1177_0145561320984581 - Intraosseous Cavernous Hemangioma of the Middle Turbinate: A Case Report
Supplemental Material, sj-docx-1-ear-10.1177_0145561320984581 for Intraosseous Cavernous Hemangioma of the Middle Turbinate: A Case Report by Yousef Bolous, Martin Bullock, David B. Clarke and Emad Massoud in Ear, Nose & Throat Journal
Supplemental Material
Supplemental Material, sj-jpg-2-ear-10.1177_0145561320984581 - Intraosseous Cavernous Hemangioma of the Middle Turbinate: A Case Report
Supplemental Material, sj-jpg-2-ear-10.1177_0145561320984581 for Intraosseous Cavernous Hemangioma of the Middle Turbinate: A Case Report by Yousef Bolous, Martin Bullock, David B. Clarke and Emad Massoud in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.