
Abstract
Cochlear implantation surgery in the rare cases of incomplete partition type III is constrained by intraoperative difficulties that result from the deformed cochlea. Our case study describes the use of a supporting fascia pad that served as a track to preserve the direction of the electrode during insertion into the cochlear lumen.
Background
Inner ear malformations account for approximately 20% of congenital sensorineural hearing loss (SNHL). 1 Incomplete partition type III (IP-III) is a rare deformity that accounts for 2% of them. 2 Incomplete partition type III causes X-linked hereditary deafness due to POU3F4 gene mutation 3 with pathognomonic findings that appear on temporal bone high resolution computed tomography (HRCT) scan. 4 Patients with IP-III present with severe progressive SNHL, which makes them potential candidates for cochlear implantation surgery. 5 However, these surgeries are constrained by major intraoperative probable accidents such as electrode misplacement into the internal auditory canal (IAC) and severe cerebrospinal fluid (CSF) gusher. 6 In this article, we report the case of a child with IP-III anomaly and profound SNHL who underwent cochlear implantation surgery, where there was difficulty obtaining a forward intracochlear electrode insertion, as it deviated toward the IAC.
Case Presentation
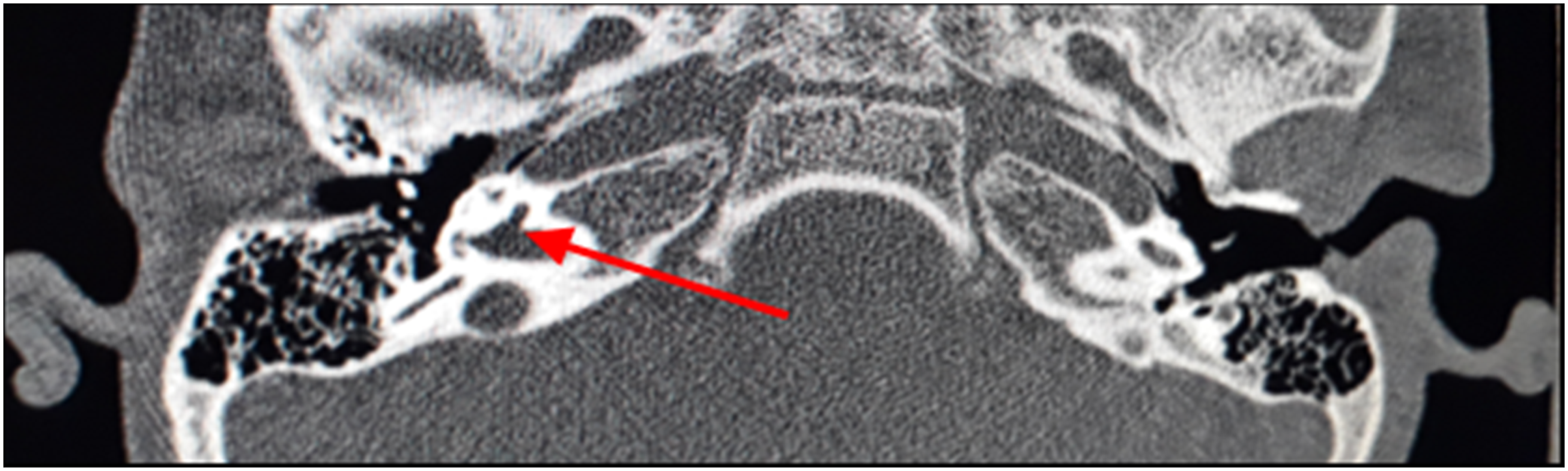
A three-year-old boy was brought to our centre because of profound bilateral SNHL that was first discovered three months earlier and did not completely resolve after using bilateral hearing aids for three months. His auditory brainstem response test did not detect the fifth wave till 90 decibels (dB) in both ears, while the negative cochlear microphonic test and the results of otoacoustic emission indicated a problem with cochlear outer hair cells. The patient’s medical, surgical and family history were clear of any relevant condition. HRCT of the temporal bones demonstrated bilateral wide IAC (Figure 1) with bone deficiency between the lateral end of the bulbous IAC and the basal turn of the cochlea (Figure 2). The patient was diagnosed with incomplete partition type III (IP-III) based on these typical radiographic features and a cochlear implantation surgery for his right ear was scheduled. (A) A coronal view of a computed tomography scan for a patient with IP-III showing a wide connection between the lateral end of the bulbous IAC and basal turn (arrow), (B) An axial view of the wide IAC (arrow). IP-III, Incomplete partition type III; IAC, internal auditory canal. An axial view of a computed tomography scan for a patient with IP-III showing deficiency of bone between the lateral end of the wide IAC and the basal turn of the cochlea (arrow). IP-III, Incomplete partition type III; IAC, internal auditory canal.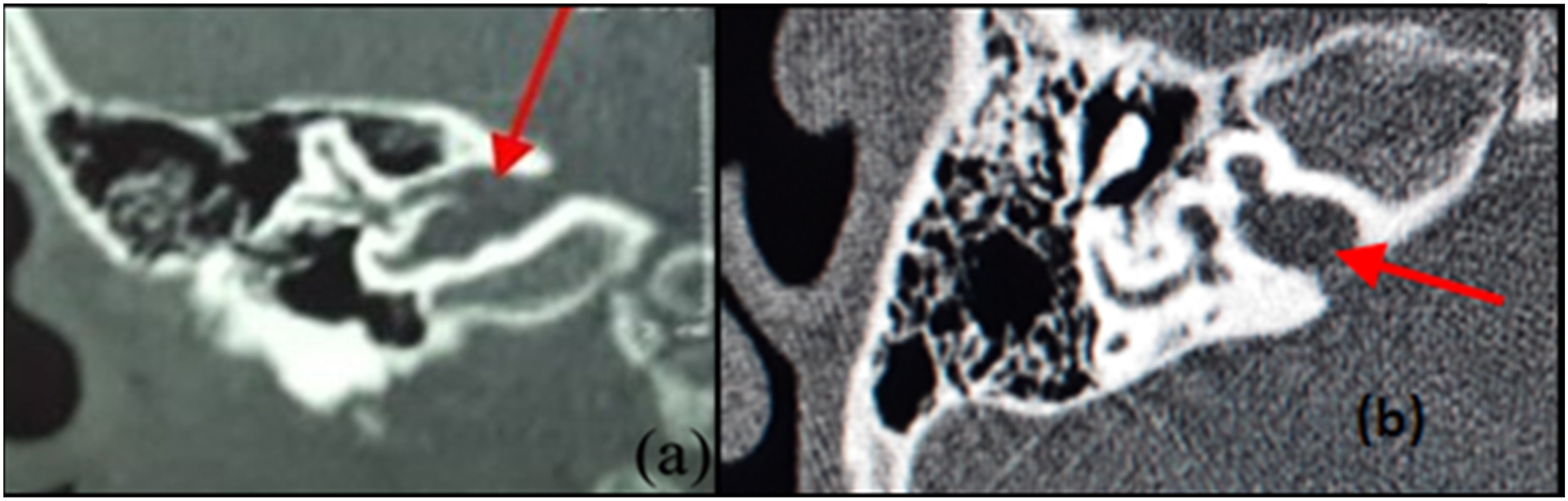
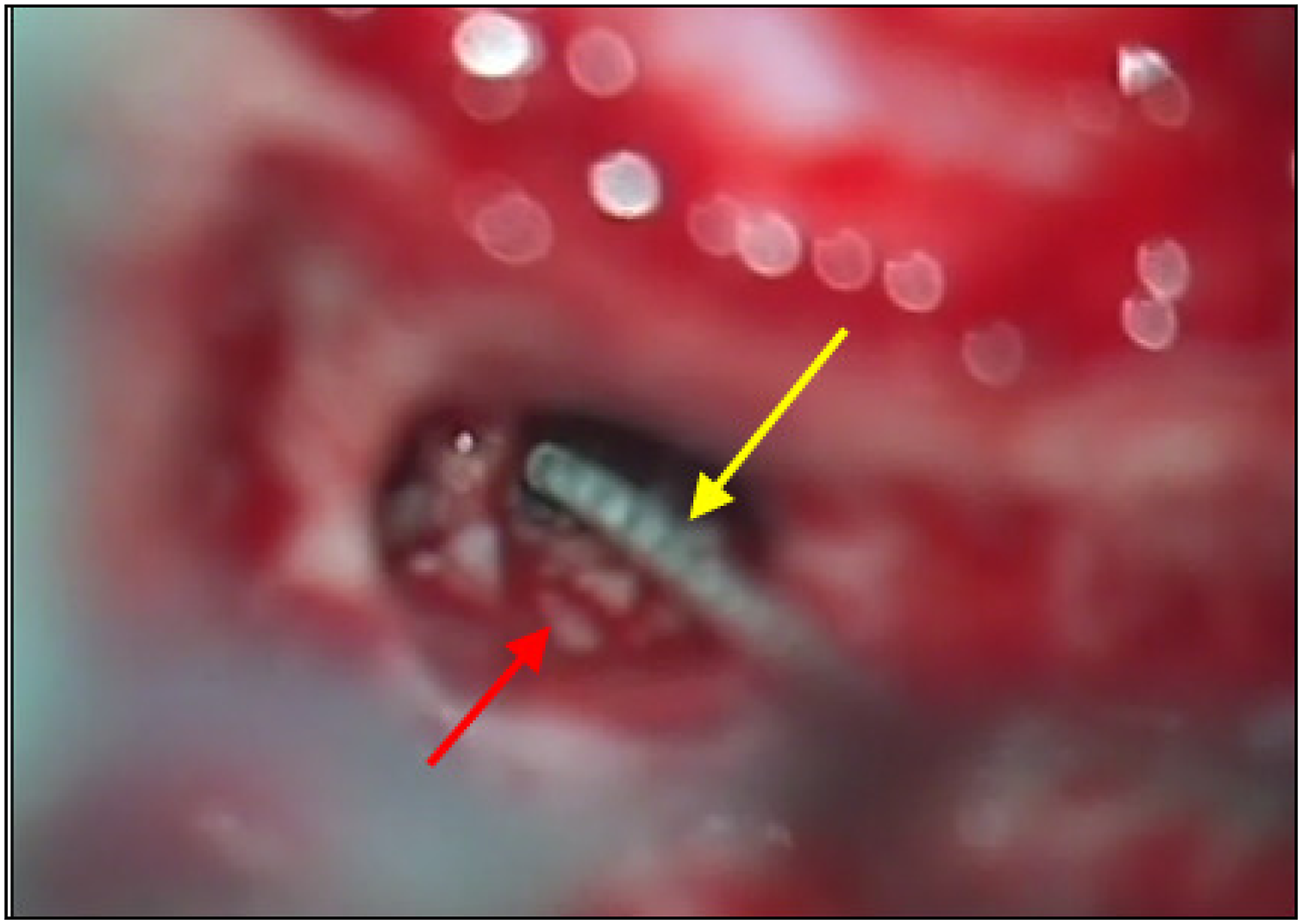
During surgery, a standard posterior tympanotomy approach was used. There were no anomalies in middle ear structures and the facial nerve. When opening the round window membrane an expected CSF gusher happened. So, the head of the operating table was elevated, and the gusher gradually decreased after two minutes. At that time, the insertion site at the round window opening was visible. In the beginning, there was difficulty obtaining a forward track of electrode insertion into the cochlear lumen, as it deviated toward the lateral basal turn wall. So, the surgeon used a piece of temporalis fascia as a supporting pad under the electrode and slid the electrode through the round window, and into the cochlea (Figure 3 and 4). A straight short compressed 15 mm electrode (MED-EL SONATA) was completely inserted, and Stenver’s radiograph view showed the typical coiled appearance of a fully inserted electrode into the cochlea without kinking or deviation toward IAC. Telemetry confirmed that the full electrode was inside the cochlear lumen, and the auditory response telemetry confirmed total activation of all channels. Then, the surgeon sealed the opening of the round window and packed it tightly with fascia. No CSF leakage was noticed. A preinsertion photograph of the right ear showing the supporting fascial pad (red arrow) that was put under the electrode (yellow arrow). A postinsertion photograph of the right ear showing the electrode through the round window (yellow arrow) and fascial pad (red arrow).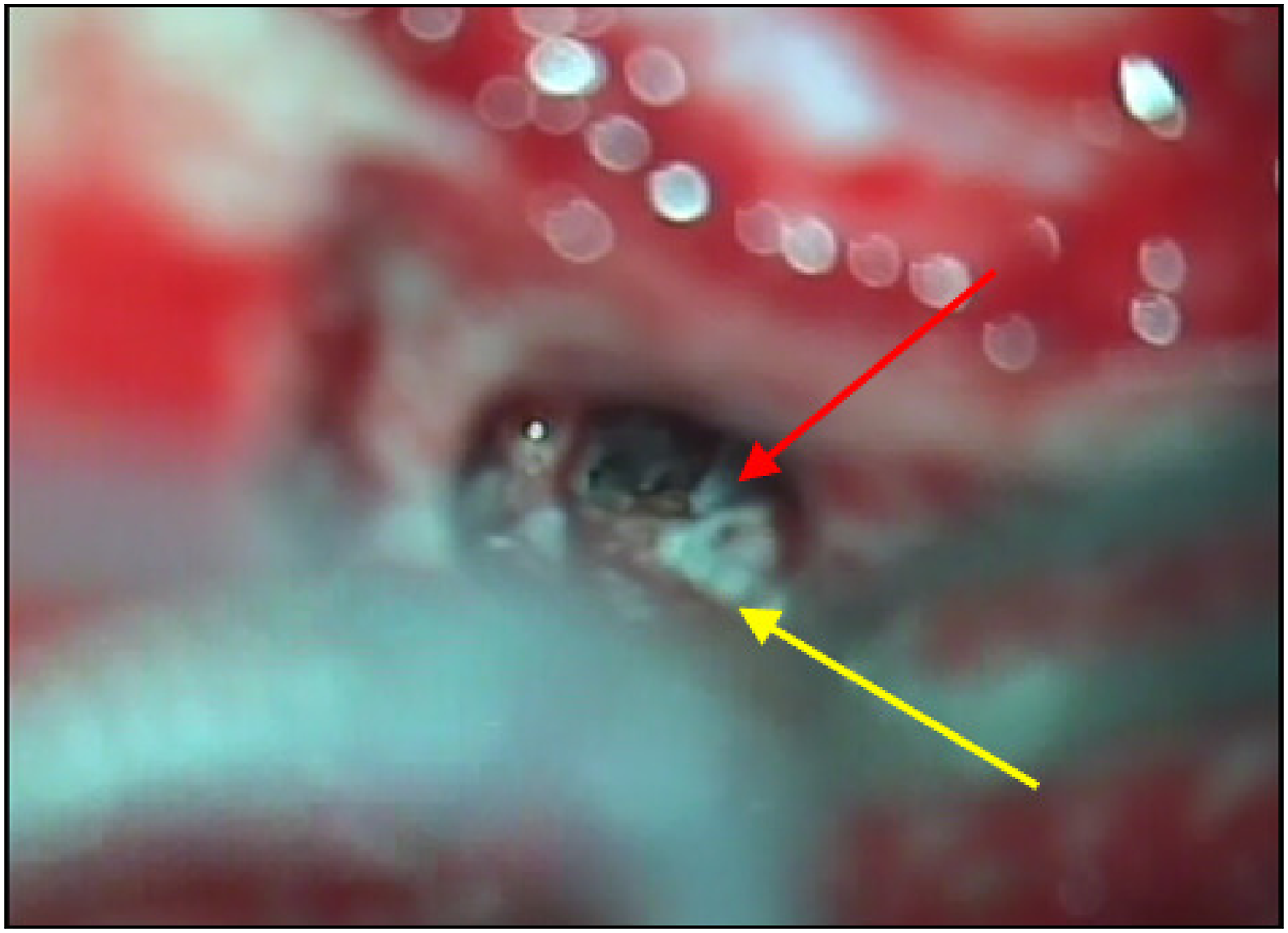
The patient’s postoperative course was uneventful. He received preoperative and postoperative prophylactic antibiotics. The follow-up assessment of facial nerve function was normal, and free field audiometry with cochlear implant showed a threshold of 40–50 dB after six months of surgery.
Discussion
Interscalar septa are present while the modiolus is completely absent in IP-III, and there is usually a large defect at the short base of the cochlea, which causes a wide entry to the IAC.7,8 Therefore, maintaining a straightforward intracochlear path while inserting the electrode is difficult, and there is a high risk to misplace the electrode into the IAC. This misplacement leads to a worsened hearing loss and carries a high risk of facial nerve stimulation, especially with the use of full banded electrodes. 9 In this case, the use of a straight short, compressed electrode type with a supporting fascia pad that was put under the electrode helped in achieving a safe and complete intracochlear insertion. The fascia served as a track to preserve the electrode forward direction while sliding it into the cochlea.
The absent bony plate of the lamina cribrosa at the fundus of the IAC weakens the area and permits direct confluence of CSF and perilymph. Consequently, it can lead to gushers when opening the round window membrane and when creating cochleostomy, in addition to a high risk of persistent postoperative CSF leakage and subsequent meningitis. Therefore, the surgical sealing of the round window in cases of IP-III is more challenging. 10 However, this risk was mitigated by using fascia to tightly pack and seal the round window opening in our surgery. A special type of electrodes with cork type stopper may have better outcomes in cases of IP-III because its unique design can efficiently close the opening around the electrode, and prevent any CSF leakage. 11
Conclusion
Incomplete partition type III carries higher intraoperative challenges during cochlear implantation because of the deformed cochlea. Yet, choosing an appropriate electrode type and the use of a supporting fascia pad can help in achieving a complete intracochlear insertion and in minimizing the surgical risks associated with IP-III.
Supplemental Material
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to this article.
Funding
The author(s) received no financial support for the conduction and publication of this report.
Informed Consent
A signed informed consent was obtained from the parents of the patient to publish this report.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.