
Abstract
Neurofibroma (NF) rarely arises in the retropharyngeal space (RPS) of patients with or without Neurofibromatosis type I (NF-I). The diffuse subtype of NF (DNF) is characterized by an infiltrative growth pattern and typically involves the skin and subcutaneous tissue of the head and neck. We describe the clinic-pathologic features of a DNF involving the RPS of an adult without NF-I. To date, this subtype of NF has never been reported at this site.
Keywords
Significance statement
Neurofibroma (NF) rarely arises in the retropharyngeal space (RPS) of patients with or without Neurofibromatosis type I (NF-I). The diffuse subtype of NF (DNF) is characterized by an infiltrative growth pattern and typically involves the skin and subcutaneous tissue of the head and neck. We describe the clinic-pathologic features of a DNF involving the RPS of an adult without NF-I. To date, this subtype of NF has never been reported at this site.
Text
The retropharyngeal space (RPS) is located deep to the pharynx and extends from the skull base to the mediastinum. 1 It contains adipose and lymphatic tissues and primary tumors arising at this site are very uncommon. 1
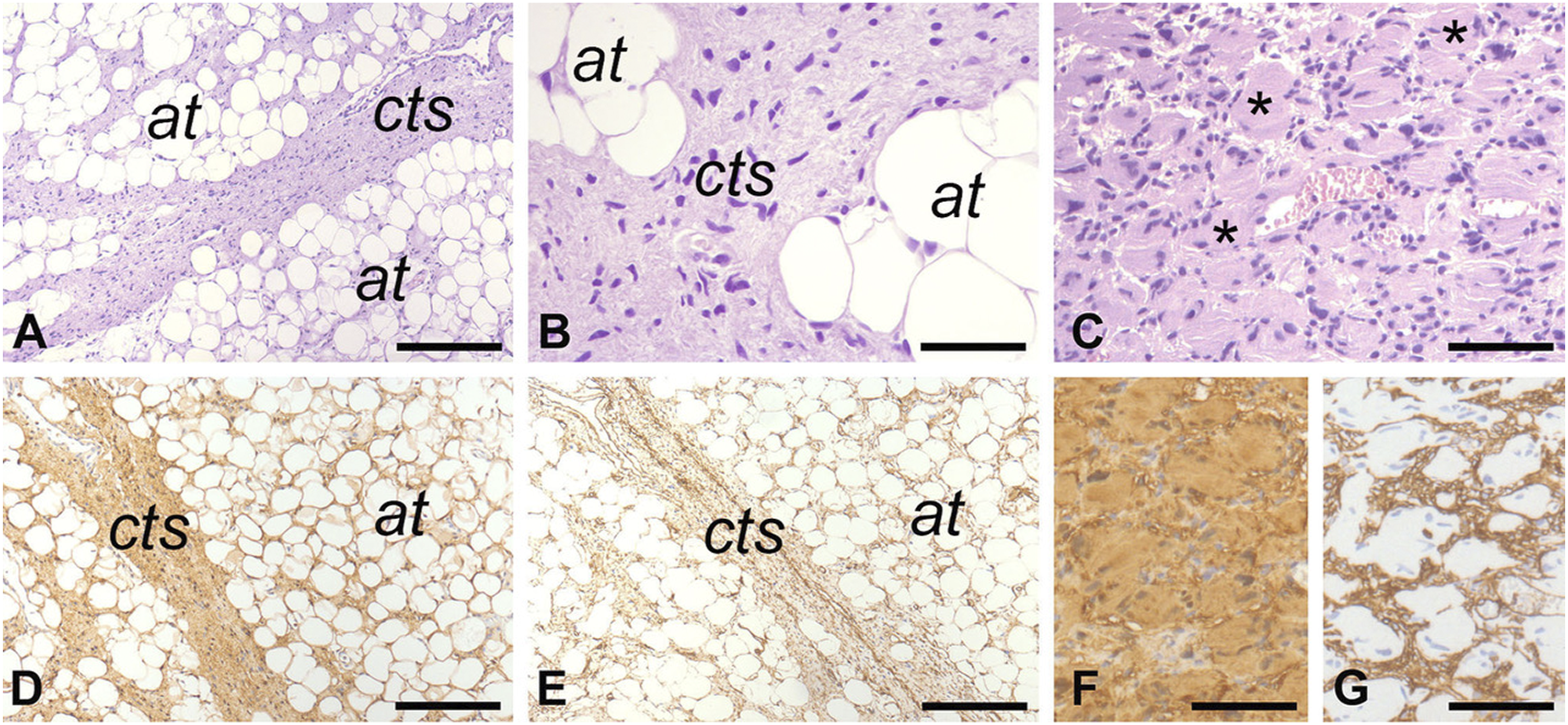
Herein we report a 61-year-old Caucasian male who presented with a space occupying lesion incidentally detected in the right side of the RPS by magnetic resonance imaging (MRI) performed for an episode of dysarthria. He was otherwise healthy and denied previous trauma, history of neurological disease or surgery on the head and neck area. Flexible fibreoptic rhinoscopy revealed a non-ulcerated swelling of the right posterior mucosa of the nasopharynx. Mobility of vocal folds was preserved and there was no palpable lymphadenopathy. Computed Tomography (CT) scan and MRI (Figure 1) revealed a poorly parameterizable RPS mass in the right petro-clival site. The mass involved posteriorly the clivus, whose cortical profile was thinned, infiltrated the prevertebral fascia, extended into the ipsilateral parapharyngeal space and reached anteriorly the nasopharynx and inferiorly the soft tissues of the laryngopharynx. In addition, it appeared indissociable from the internal and external carotid arteries and the internal jugular vein. As a nasopharynx biopsy was not conclusively representative of the lesion, a biopsy through a cervicotomic approach was performed. Histological examination (Figure 2A and B) revealed a tumor composed of bland spindle-shaped cells with wavy, round or fusiform nuclei within a loose matrix of fine fibrillary collagen. The neoplastic tissue expanded through connective tissue septa, entrapped small nerves, was associated with ecstatic blood vessels and infiltrated adipose tissue and the wall of the internal jugular vein. Clusters of pseudo-meissnerian bodies were focally recognized (Figure 2C). Necrosis and mitosis were not detected. Immunohistochemical analysis, performed as described previously,
2
-7
showed immunoreactivity of the neoplastic cells for S100 (Figure 2D) and CD34 (Figure 2E), but not for pan-cytokeratin, EMA, Smooth Muscle Actin, HMB45 and CD117. The pseudo-meissnerian bodies were immunoreactive for S100 (Figure 2F) and outlined by CD34 positive cells (Figure 2G). Mastcells (CD117+) were abundant within the lesional tissue. The overall expression of Ki-67 was less than 5%. These pathological findings were consistent with Diffuse Neurofibroma (DNF). Based on this diagnosis, clinical workup for Neurofibromatosis-type 1 (NF-1) was performed but it was negative. For the infiltrative growth pattern that reflected in the extensive involvement of cervical vascular structures, debulking of the tumor was proposed to the patient but he refused and decided to undergo treatment and follow-up elsewhere. Coronal image of CT scan before contrast agent injection is illustrated in A. The mass involves the skull base and the right parapharyngeal space (red arrow) and is associated with resorption of the jugular tubercle (white arrow), the occipital condyle (arrowhead) the bony portion of carotid canal and the petrous apex (green asterisk). The “eagle sign” (highlighted by red circle on the left side) is not recognizable and hypoglossal canal (red asterisk) and foramen ovale (yellow asterisk) are widened. After contrast agent injection (B), are appreciable the vascular characteristics of the structures around the lesion in the parapharyngeal space like the ectasia of the internal carotid artery (red asterisk). Furthermore, are evident the tortuous vessels that are part of the mass (red arrow). Post-contrast MRI T1-weighted coronal and T1-weighted axial Volumetric interpolated breath-hold examination (VIBE) images are shown in C and D respectively. The tumor (red arrow in C and D) involves the skull base and the right parapharyngeal space. The internal carotid artery is recognizable within the tumor (white asterisk in C). Low and high-power magnification histological views of the lesion are illustrated in A and B, respectively. The neoplastic tissue expands connective tissue septa and infiltrates into the adipose tissue. Pseudo-meissnerian bodies (asterisks) are illustrated in C. The neoplastic tissue is immunoreactive for S100 (D) and for CD34 (E). The pseudo-meissnerian bodies are highlighted by S100 (F) and outlined by CD34 immunoreactive cells (G). Bars: 150 µm in A, D and E, 80 µm in B and 100 µm in C, F and G. A-C: hematoxylin and eosin. In A, B, D and E, cts is for connective tissue septa and at is for adipose tissue.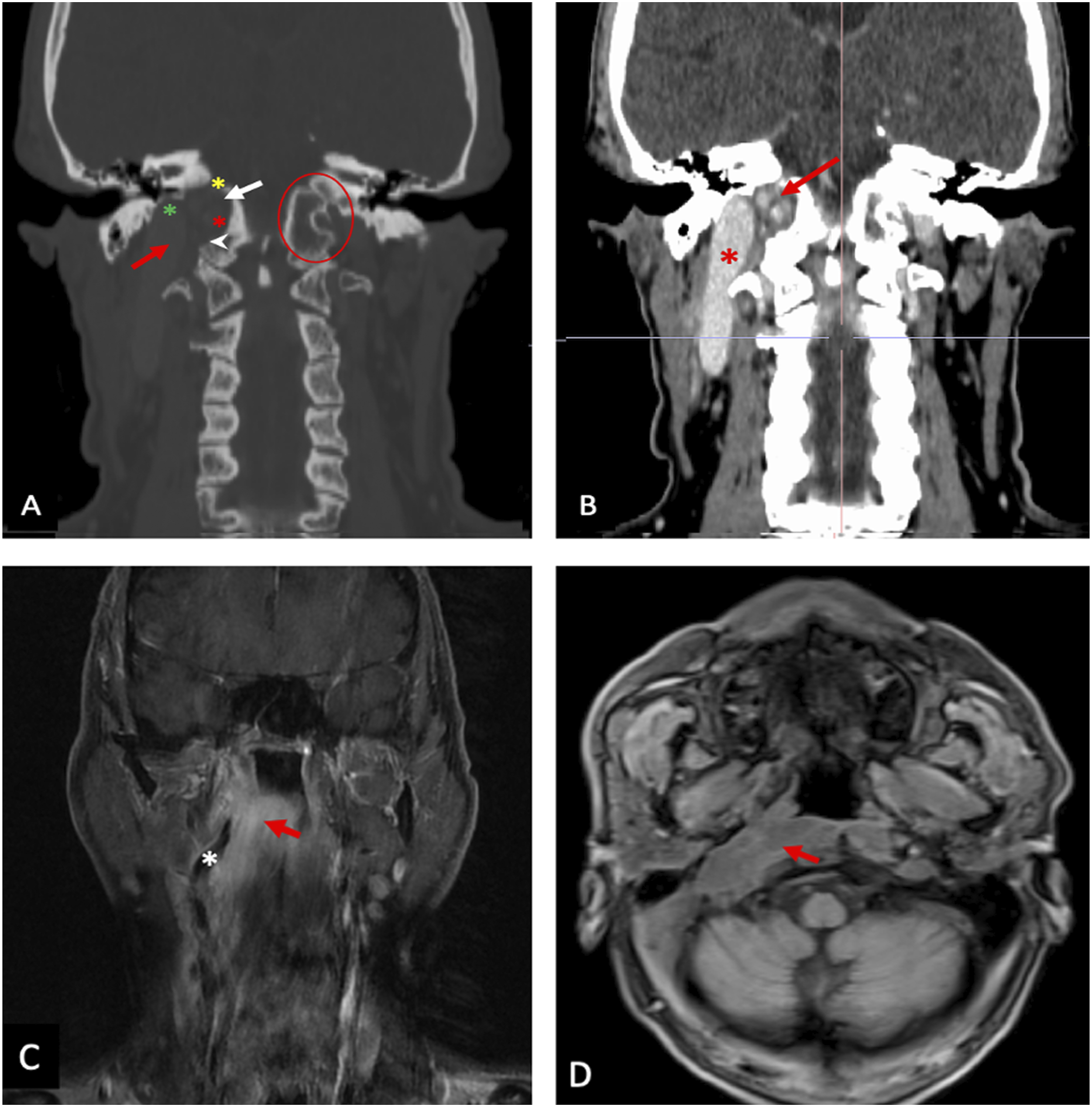
DNF is a distinct subtype of neurofibroma most commonly occurring in the head and neck region of middle-aged adults. 8 -10 It typically involves dermis and subcutaneous tissue, in which it spreads along connective tissue septa entrapping dermal adnexal structures and infiltrating between adjacent adipocytes, and as the other clinic-pathologic subtypes of NF (i.e., localized and plexiform), it may occur in the context of with NF-1. 8,10 Even though rarely, DNF may involve superficial and deep soft tissues and viscera 11,12 and may undergo, in particular in patients with NF-I, to transformation into malignant peripheral nerve sheath tumor. 9 A characteristic histologic feature of DNF, considered by some authors a diagnostic requirement, is the presence, as observed in our case, of eosinophilic, lamellar organoid stuctures reminiscent of Meissner bodies (i.e., pseudo-meissnerian bodies). 8,10
NFs have been reported in the RPS. 13 -15 However, as far as we know, the diffuse subtype has never been reported at this site. As NFs cannot be easily separated from the nerve of origin, complete excision of the neoplasm may require sacrifice of the nerve itself. 14 Although this treatment may be acceptable for lesions involving dermis and subcutaneous tissue, deep-seated NF, in particular the diffuse subtype due to its infiltrative pattern of growth, may often be only debulked or treated conservatively. 14 In these cases, the risk of recurrence is high and close clinical and radiological follow-up is mandatory. The role of additional and novel therapeutic approaches 16 in patients not amenable to radical surgical resection remain to be assessed.
Footnotes
Acknowledgments
The authors gratefully acknowledge Prof. Angelo P. Dei Tos (Department of Medicine, University of Padua, School of Medicine, Padua, Italy) who reviewed the histological slides and confirmed the pathologic diagnosis.
Authors’ note
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request. All the clinic-pathologic investigations detailed in the manuscript have been conducted in accordance with the Declaration of Helsinki and its later amendments or comparable ethical standards. Written informed consent for publication of data and images was obtained from the patient.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.