
Abstract
Background
Transoral supraglottic laryngectomy (TSL) has been widely applied in the treatment of supraglottic cancers. The aim of this study is to evaluate a simplified technique for excising properly selected supraglottic tumors with a transoral coblation-assisted system.
Methods
Eight patients with T1-3N2M0 supraglottic cancer were treated with TSL with the coblation-assisted system.
Results
Tumors in all patients were en bloc resected with negative surgical margins and the selective neck dissection was also performed. The mean operation time for TSL was 39 minutes (25–65 minutes). The average time for the removal of the nasogastric tube was 8.6 days (1–28 days). All patients were extubated and shifted to the ward after operation. None of the patients required tracheotomy.
Conclusion
Coblation-assisted TSL is a relatively simple, easy approach with low risk. It could be a feasible and safe procedure for patients with properly selected supraglottic cancer.
Keywords
Introduction
Laryngeal carcinoma is a common malignancy of the head and neck.1,2 Supraglottic carcinoma is the dominant type of laryngeal tumor, while alcohol and smoking are the common risk factors.1,3 Patients with supraglottic carcinoma often present with non-specific throat pain, dysphagia, and neck lymphadenopathy as the primary disease features with poor overall survival.4,5 Transoral laser microsurgery (TLM) has been widely applied in the treatment of supraglottic cancers and has achieved promising outcomes. Meanwhile, transoral supraglottic laryngectomy (TSL) has been found to have better short-term and long-term swallowing function compared to open supraglottic laryngectomy (OSL) and chemoradiotherapy.6-8 Since a surgical robot can provide 3-dimensional high-definition visualization, the transoral robotic surgery has further improved the scope of transoral resection.9,10 In recent years, radiofrequency coblation has been gradually applied in endoscopic laryngeal surgery.11,12 It has several advantages, such as manual dexterity, small surgical trauma, quick postoperative recovery, easy bleeding, and low cost. However, whether RF coblation could be used to treat supraglottic cancers remains unclear. In this study, we aimed to evaluate the outcomes of RF ablation and the complications in patients with supraglottic cancers.
Methods
Patients
Clinical characteristics of eight patients before and after surgery.
Abbreviations: SCC, squamous-cell carcinoma; NECs, neuroendocrine carcinoma.
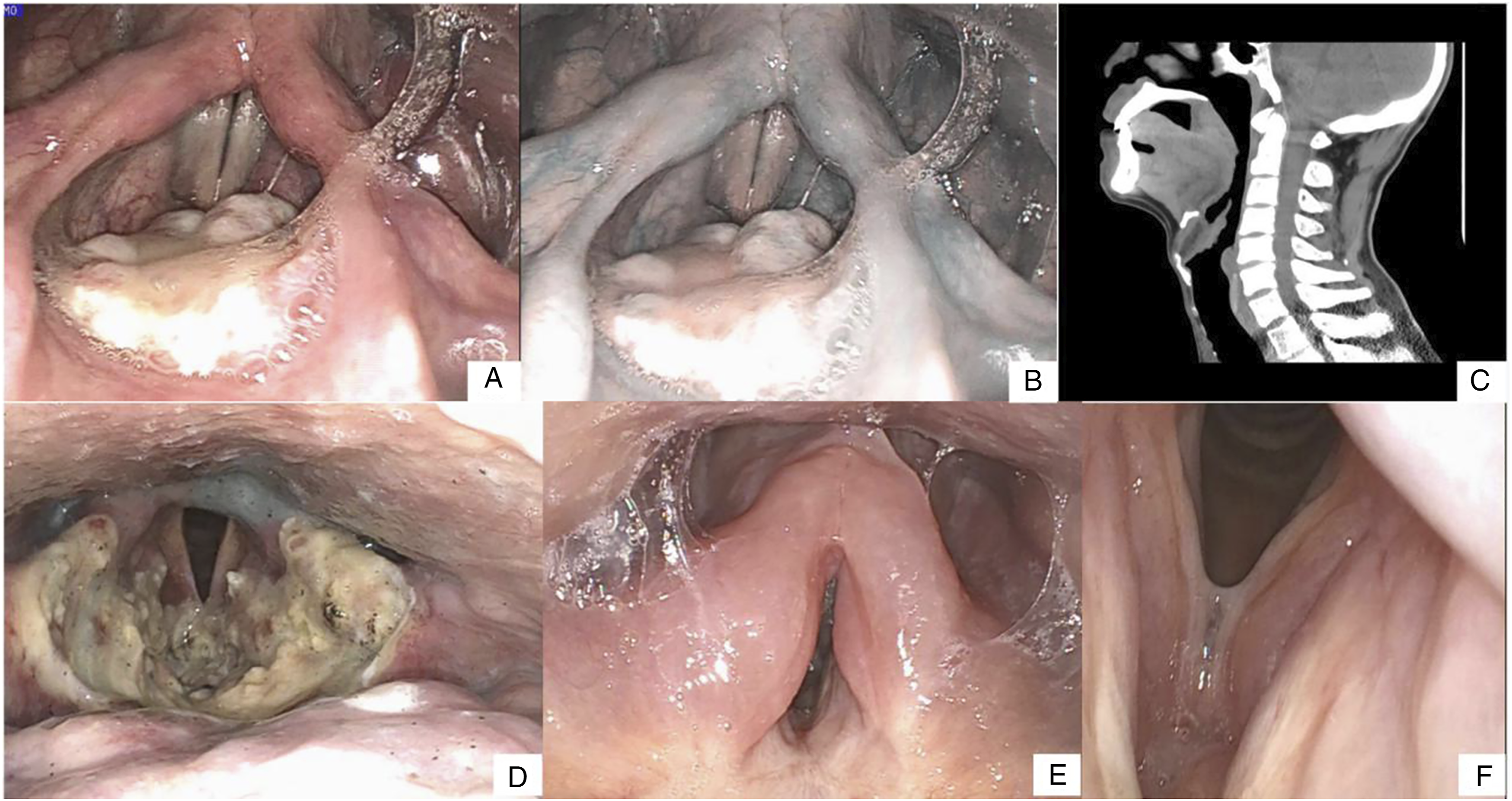
(A–B) T1 supraglottic tumors located solely on the laryngeal side of the epiglottis. (C) CT image showing an epiglottic tumor and no infiltration of the pre-epiglottic space. (D) Fiberoptic endoscopic evaluation of swallowing showed the functional oral intake scale with mild laryngeal penetration/aspiration. (E–F) Follow-up showed no recurrence and pharyngeal residue.
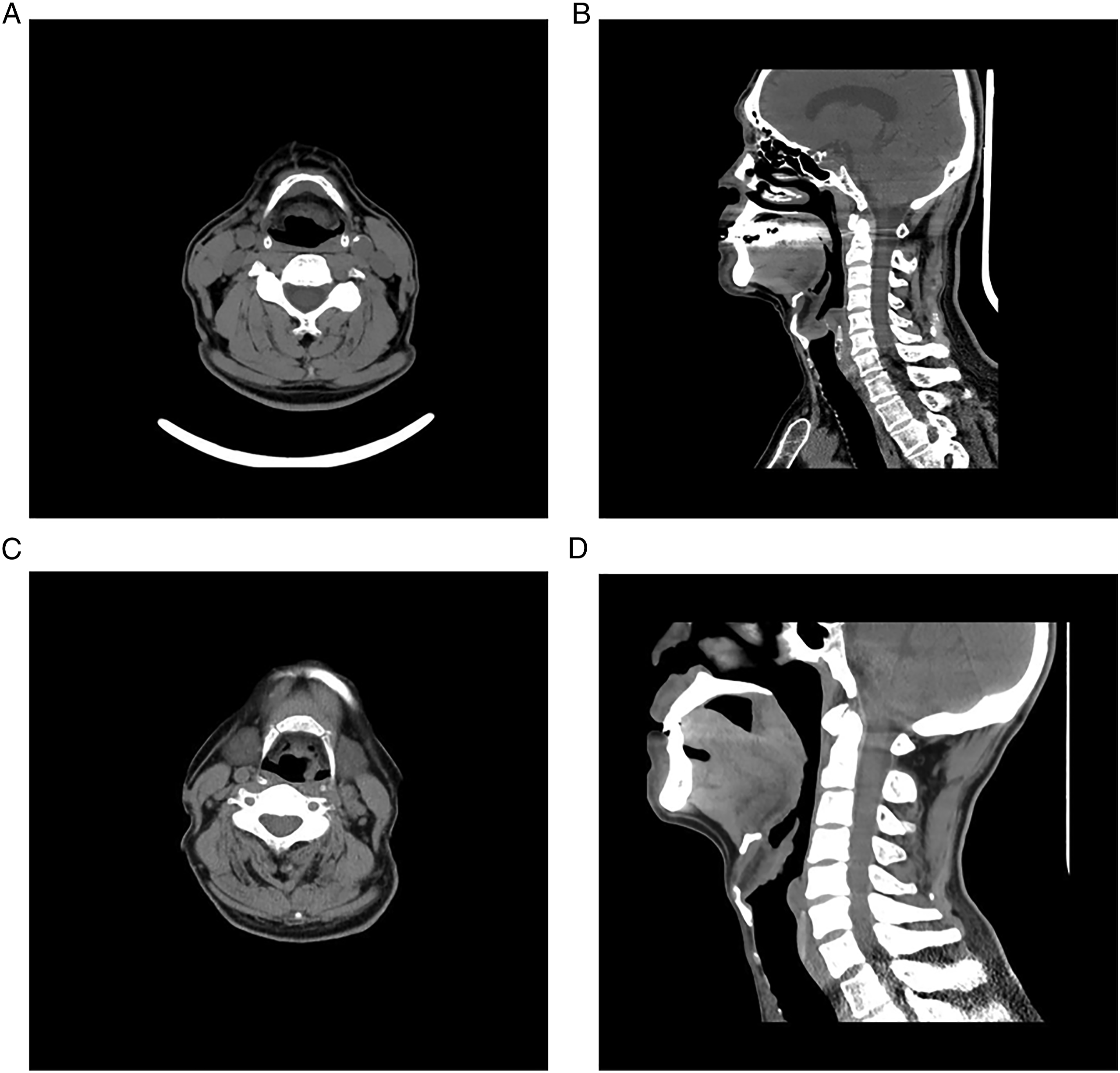
Patients with T1-3 supraglottic tumors by X-ray examination. (A–B) The tumor was confined to the epiglottis and did not invade the anterior epiglottic space. (C–D) Invasion of epiglottis and crinkle wall of arytenoepiglottis.
Surgical procedure
The procedures were similar with the techniques described by Remacle et al.
13
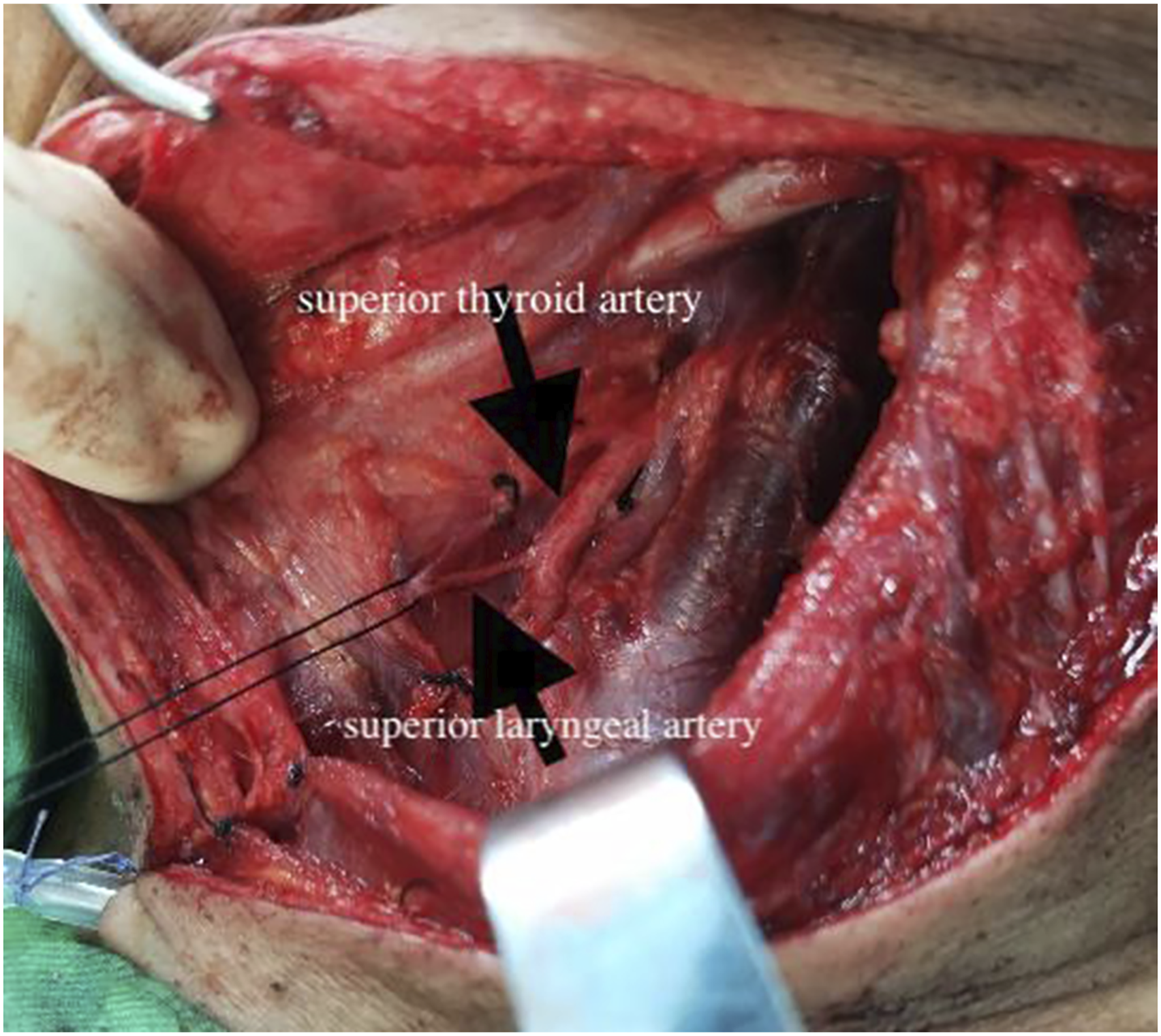
The supraglottic region was exposed with a bivalved laryngopharyngoscope after general anesthesia. Laryngeal plasma cutter (JXHZ G33E61, Beijing, China) was used after a sufficient view was obtained. The power of ablation by the plasma system was routinely adjusted to Gear 7 and the power of electric coagulation hemostasis was adjusted to Gear 5. The incision was initiated over the bilateral aspects of the pharyngoepiglottic folds (Figure 3A)). To reduce the bleeding and obtain a clear operation field during the operation, bilateral superior laryngeal vascular bundles were firstly identified (Figure 3B) and cauterized with monopolar electrical coagulation (Figure 3C). The dissection proceeded anteriorly and laterally for resection of the pre-epiglottic space. The epiglottis in continuity with the tumor was en bloc removed (Figure 3D–E)). The aryepiglottic folds were then transected superior and lateral to the arytenoid, with an oblique incision for transecting the posterior vestibular fold and entering the ventricle. The transection continued anteriorly at the ventricular apex until the petiole and anterior commissure were encountered. The pre-epiglottic dissection was associated with the transection inferior to the epiglottic petiole to allow for removal of bilateral laryngeal ventricles (Figure 3F). In all cases, the procedures were terminated after negative margins were obtained (R0 resection). Bilateral selective neck dissections (levels II, III, and IV) were routinely performed when the lesion passed through the midline of the larynx. Bilateral superior laryngeal arteries were ligated once again to prevent postoperative bleeding during neck dissection (Figure 4). During the bilateral neck dissection, supraglottic tumors were removed and coblation was performed at the same time. All patients were extubated after completion of the procedure and did not require temporary tracheostomies. The fiberoptic endoscopic evaluation of swallowing (FEES) was used to evaluate the swallowing function on postoperative days 2–5. If the FEES score was more than 5 indicating nonomal feeding for all nutritional intake, the patient could resume oral feeding. If the FEES score was less than 5, the patient was administrated with tube feeding diet and eating exercise. The patients were discharged after removal of the cervical drainage tube 1–3 days after surgery. Postoperative radiotherapy was considered for patients who had multiple metastatic lymph nodes or perineural/lymphatic/vascular invasion. Postoperative radiotherapy was usually initiated at 2–4 weeks postoperatively. The FEES and VHI-10 were used to evaluate the swallowing and phonation functions at the end of all treatments. (A) Exposure of the supraglottic region. (B–C) Bilateral superior laryngeal vascular bundles were identified and cauterized. (D–E) Transection of the epiglottis with tumor en bloc. (F) Surgical field after removal of the specimen. The superior laryngeal arteries were ligated once again during neck dissection.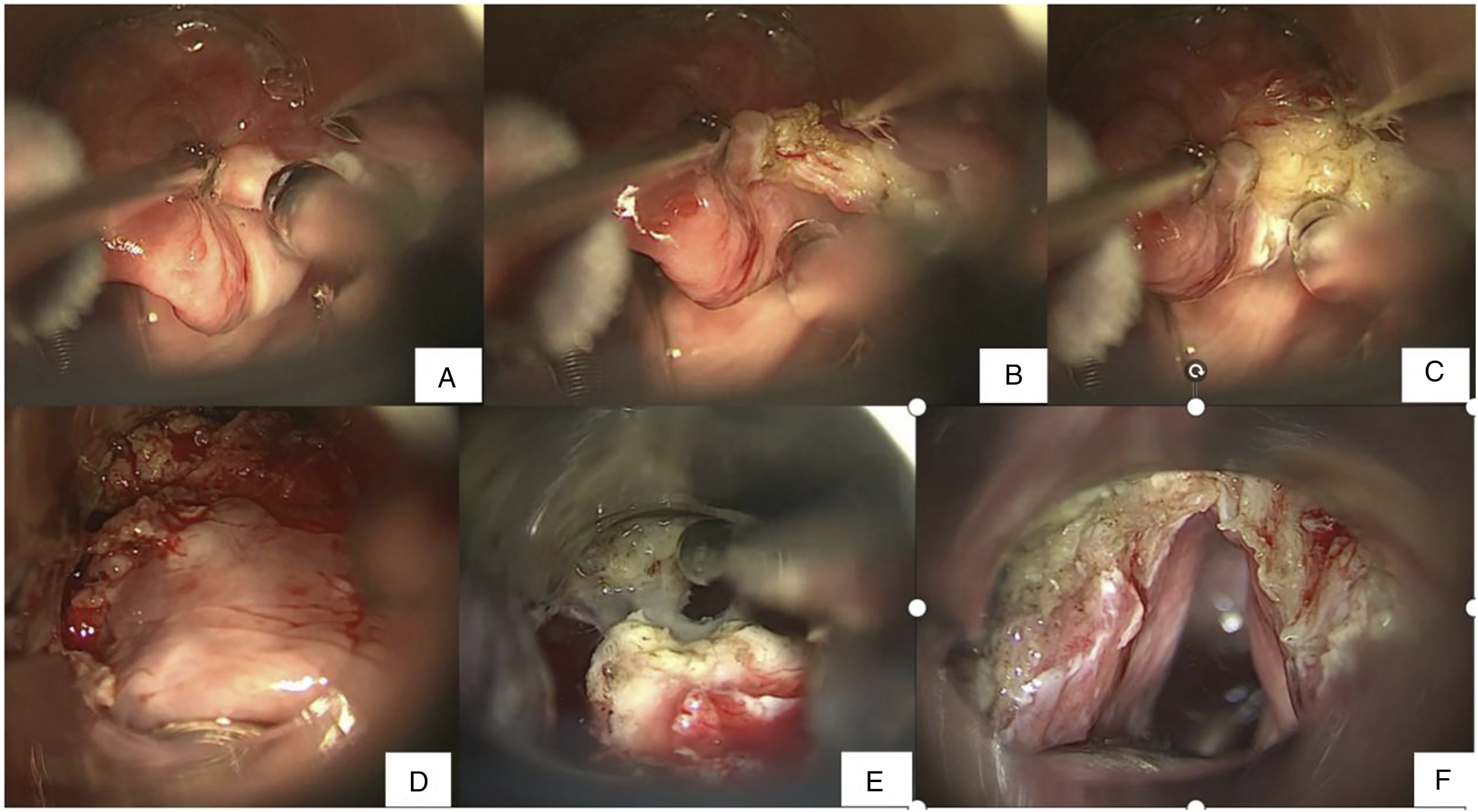
Results
The treatment outcomes and functional results of eight patients who received transoral supraglottic laryngectomy.
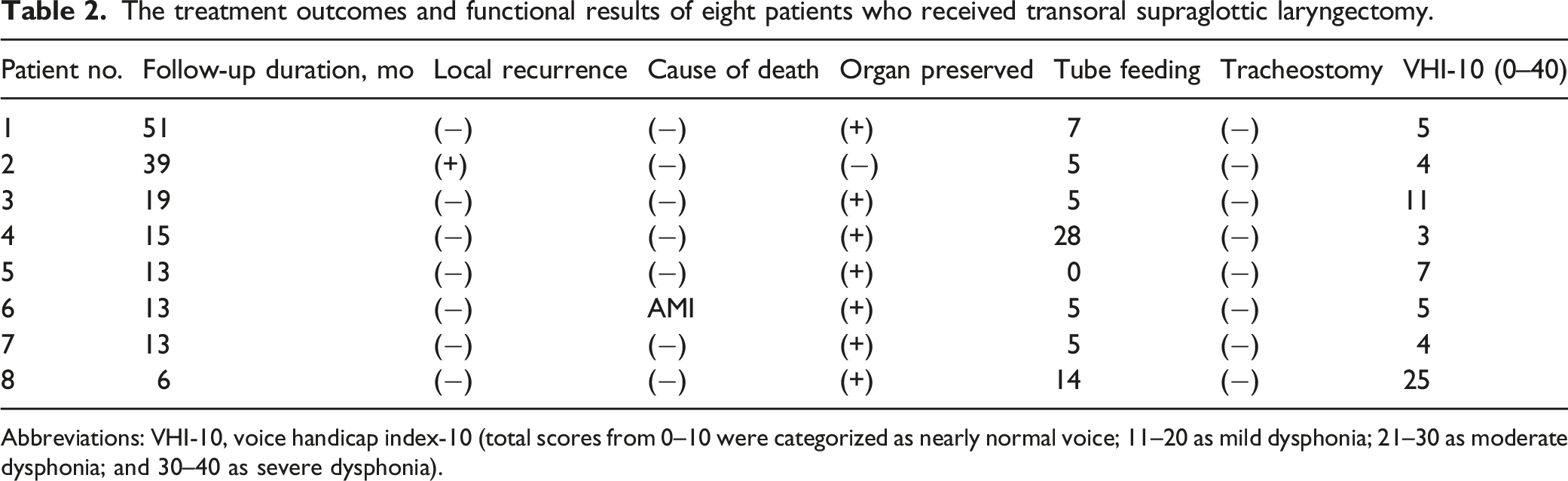
Abbreviations: VHI-10, voice handicap index-10 (total scores from 0–10 were categorized as nearly normal voice; 11–20 as mild dysphonia; 21–30 as moderate dysphonia; and 30–40 as severe dysphonia).
Discussion
Coblation radiofrequency is a minimally invasive technique for soft tissue treatment which has been used since late 1990s. 14 Its precise, non-thermally disruptive properties make it an attractive alternative therapy for recurrent respiratory papillomatosis in the tracheobronchial tree. 15 The plasma layer produces a high-density energy field to break molecular bonds within targeted tissue and allows for efficient soft tissue excision while preserving the integrity of the adjacent normal tissues. 16 It works at a relatively low temperature (between 40°C and 70°C) to precisely remove the targeted tissue in a gentle fashion without causing unpredictable thermal damage; thus, the postoperative tissue reaction is mild. The wand of coblation radiofrequency is flexible and can be curved to excise the segments that cannot be excised due to the straight line of CO2 laser. Coblation radiofrequency has been applied effectively in the many other ENT procedures, such as tonsillectomy, small tumors in the oral pharynx or laryngopharynx, glottic cancer, snoring, and sinus surgery.15,17,18 In addition, the cost of coblation is much lower than that of laser or robotic surgery; therefore, it can be widely performed in some poor areas.
The effect of TLM on supraglottic cancers has confirmed. TLM may retain the integrity of extralaryngeal muscles and pharyngeal mucosa; thus, the intervention for swallowing function is minimal without tracheotomy in most cases.19,20 Except for laser and robotic surgery, we found that coblation radiofrequency might also be an option for treating TSL. Although the sample size of this study was small, we showed that this surgical method was successful in removing the epiglottis and en bloc tumor, and complete supraglottic laryngectomy with the transoral coblation-assisted system was successfully performed. The resection range, including the endolaryngeal mucosal and soft tissue, was comparable to that of the classical OSL, except for thyroid cartilages. All patients complied with the basic principles of oncologic surgery and achieved negative surgical margins. The hyoid bone and anterior cervical muscle tissue were not disturbed. Therefore, the patients treated with coblation-assisted TSL could achieve higher levels of voice- and swallowing-related quality of life. The FEES showed that most of the granules were shunted into bilateral piriform fossae through the rear end of the tongue after operation, which could largely avoid the occurrence and development of aspiration. Six patients resumed oral feeding within 7 days after transoral coblation-assisted TSL, and two patients resumed oral feeding after 2–4 weeks of postoperation. None of the patients required tracheotomy. In addition, severe bleeding is one of the potentially life-threatening complications of endoscopic surgery. Bilateral endoscopic electrocoagulation of the superior laryngeal arteries was performed, and they were once again ligated during neck dissection to avoid serious hemorrhagic complications.
The application of coblation in the treatment of supraglottic cancers was decided by the situation of patients and tumor. Due to different degrees of aspiration after supraglottic horizontal partial laryngectomy, patients must have good lung function to tolerate aspiration pneumonia caused by aspiration. FEV1/FVC is required to be >50%. Besides, poor blood glucose control in diabetes patients is also an important factor affecting the prognosis of the patients. Finally, the exposure of endoscopic surgery is important; thus, it is necessary to eliminate the conditions that may lead to difficult exposure, such as closed teeth, giant tongue, small jaw, and so on. The stage and range of the tumor are important determinants of the surgical method and difficulty. Coblation in the treatment of supraglottic cancers has advantages of short recovery time of swallowing function, retention of pronunciation function, low tracheotomy rate, postoperative complications, cost, and short hospital stay.
Conclusion
In conclusion, TSL for early supraglottic carcinoma is a new trend. In current study, we report our preliminary experience with coblation-assisted TSL, which is relatively simple and easy to perform with a low risk. It could be a feasible and safe procedure for patients with properly selected supraglottic cancer.
Footnotes
Author contributions
Jing Zhao carried out study design, literature research, clinical studies, and data acquisition and analysis and contributed to manuscript preparation, editing and review; Jinrang Li was the guarantor of integrity of the entire study and helped to study concepts.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study is approved by the Ethics Committee of The Sixth Medical Center of PLA General Hospital.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Data availability
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.