
Abstract
Objective:
This study compared the effects of radiofrequency (RF) coblation and cold steel (CS) surgery for the treatment of Reinke’s edema (RE).
Methods:
A retrospective analysis was conducted on 61 patients with RE, with 33 (54.1%) in the CS surgery group and 28 (45.9%) in the RF coblation group. The primary endpoints were the bilateral operation time and dyspnea severity, assessed preoperatively and at 1 and 3 months postoperatively. Secondary endpoints included subjective and objective vocal assessments, laryngovideostroboscopy (LVS) images, and Voice Handicap Index-10 (VHI-10) scores obtained before and at 1 and 3 months postoperatively.
Results:
The average bilateral operation time was significantly shorter in the RF coblation group (24.2 ± 3.9 min) compared to the CS group (38.4 ± 5.2 min) (P = .041). All patients experienced a decrease in their Dyspnea Severity Index (DSI) scores postoperatively, with no significant differences observed between the two groups at any time point. However, improvements in the grade of hoarseness, roughness, and asthenia were significantly greater in the RF coblation group than in the CS group (P < .001). There were no statistically significant differences in breathiness and strain between the two groups. The average VHI-10 score significantly decreased from preoperative values in both groups (P < .001), with no significant differences observed between the two groups at any time point.
Conclusions:
The RF coblation procedure is a reliable and safe method for RE surgery, offering an effective treatment choice for RE.
Introduction
Reinke’s edema (RE) of the vocal fold is a relatively rare clinical finding in laryngology, which may result in symptoms such as hoarseness, pharyngeal discomfort, and in severe cases, aphonia, and dyspnea. 1 Commonly associated with smoking and laryngopharyngeal reflux disease (LPRD), RE can also occur due to vocal abuse.2,3 Treating patients with RE poses a significant challenge. While voice therapy and proton-pump inhibitors (PPIs) are typically the initial course of action, failure to improve with conservative treatment often necessitates surgical intervention. 4
Several surgical options exist, such as “cold steel” (CS) microlaryngeal phonosurgery, 5 CO2 laser-assisted microlaryngosurgery,6-8 or microdebrider surgery,8,9 each aiming to preserve part of the mucosal lining and minimize damage to the deeper structures of the vocal fold. However, none of these methods have been conclusively determined to be superior to the others in terms of voice improvement.7,10
Although laser surgery is widely used in laryngeal procedures, its applicability for treating RE has been questioned due to the potential risk for heat dispersion damaging the surrounding healthy tissue, leading to scarring.6,11 It also requires a larger medical team to ensure effectiveness and safety, thereby increasing procedural costs and inconvenience.11,12 Moreover, the use of lasers can potentially cause complications such as facial and mucosal burns, vocal fold webs, stenoses, and glottic incompetence. 11
Radiofrequency (RF) coblation is an emerging technology that can cut soft tissue and provide hemostasis at a lower temperature (40°C-70°C), 12 and its use in laryngeal surgery is increasing.12-15 Recently, RF coblation has been adopted in our department to treat RE. To the best of our knowledge, there are few reports on the use of RF coblation in treating RE. Therefore, we compared the voice outcomes following CS surgery and RF coblation for RE.
Materials and Methods
The study protocol was approved by the Institutional Ethical Review Board of Yiwu Central Hospital, China, and informed consent was obtained from all participants.
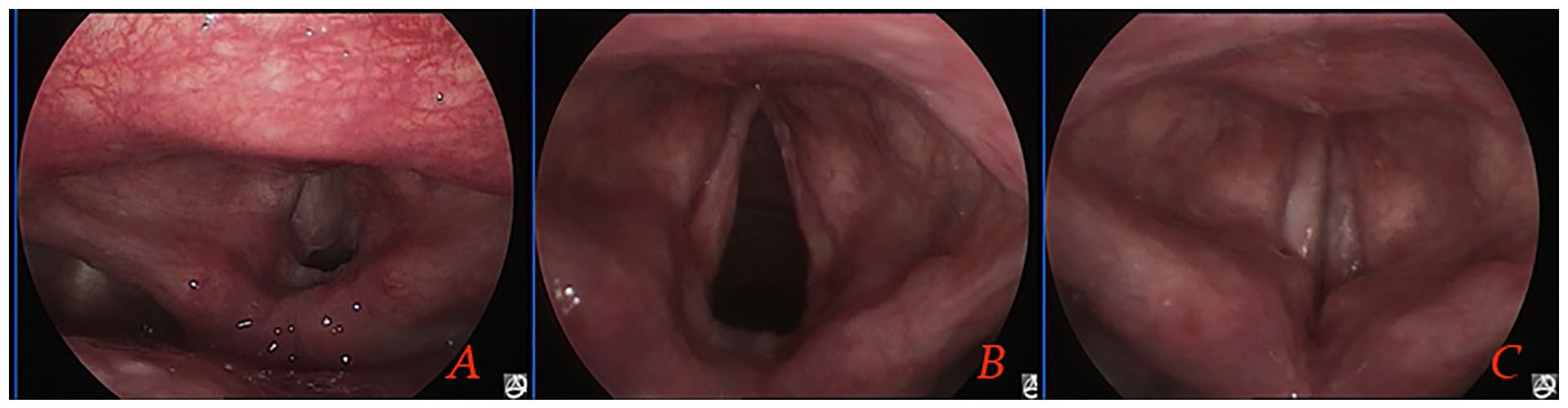
We conducted a retrospective study of clinical data and surgical records of patients with bilateral RE of grade 3 or 4 severity (Figure 1). These patients underwent surgery in the Department of Otolaryngology between May 2013 and September 2021. The severity of the disease was graded according to the classification described by Bryson: 16 grade 2 signifies an expanded polypoid lesion occupying 25% to 50% of the glottic airway; grade 3 denotes an expanded polypoid lesion covering 50% to 75% of the glottic airway; grade 4 represents an obstructive lesion, irrespective of laterality, that occupies more than 75% of the glottic airway. The principal manifestations of these grades were persistent or progressively worsening hoarseness, with or without dyspnea. Inclusion criteria included a smoking history of at least 5 years, with or without concomitant LPRD, treatment with preoperative PPIs, and voice therapy before or after surgery. Patients who had undergone any previous laryngeal surgery were excluded.
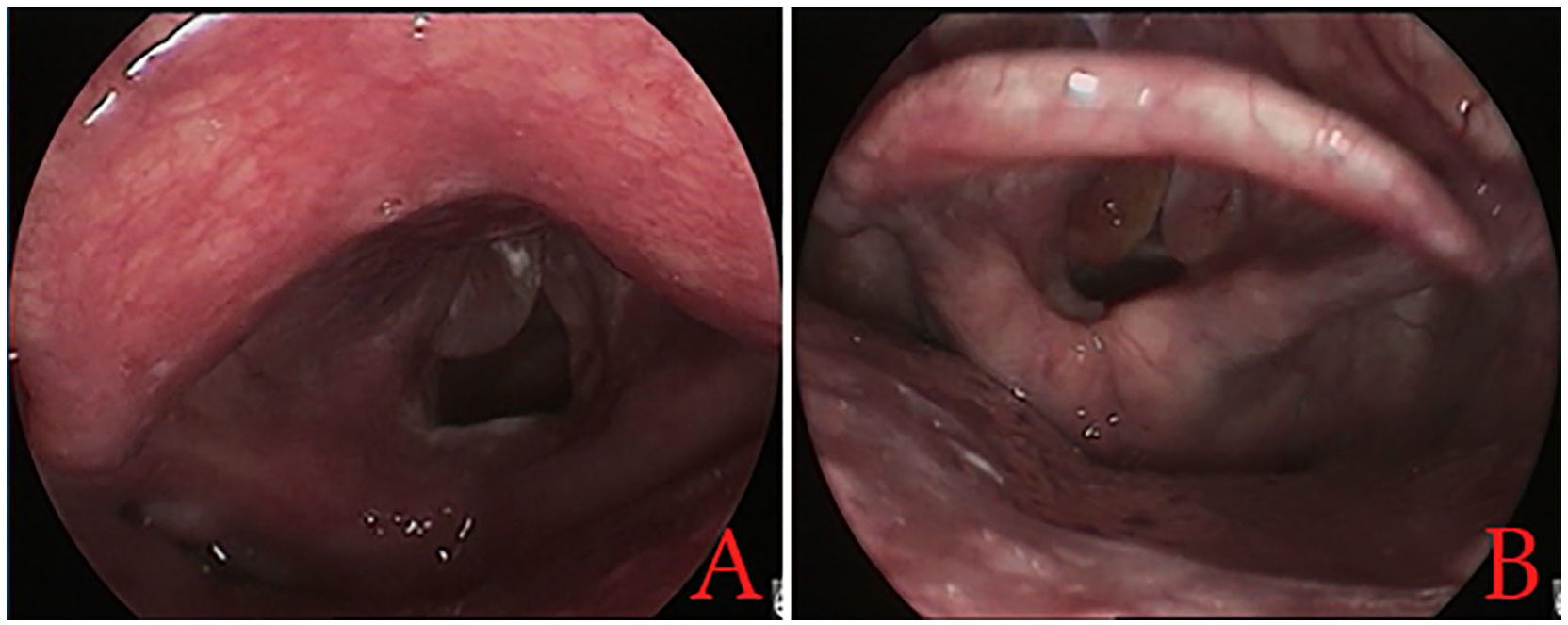
Classification of Reinke’s edema: (A) Grade 3 and (B) grade 4.
Laryngovideostroboscopy (LVS) examination revealed bilateral vocal cord lesions in all patients. Of these, 33 (54.1%) with an average age of 52.8 ± 5.1 years (17 cases were grade 3 and 16 cases were grade 4, including 9 females and 24 males) were treated using traditional CS microlaryngeal instruments (the CS surgery group) from May 2013 to December 2017. These patients had a disease duration ranging from 6 months to 10 years. However, starting from 2018, the senior author shifted to employing coblation for all cases instead of CS. Twenty-eight patients (45.9%), with an average age of 51.7 ± 4.9 years (15 cases were grade 3 and 13 cases were grade 4, including 6 females and 22 males), were treated using the RF coblation technique (the RF coblation group) from January 2018 to September 2021. These patients had a disease duration ranging from 6 months to 12 years. All patients were strictly instructed to cease smoking at least 4 weeks before the operation and to continue abstaining after the surgery.
Dyspnea and Voice Assessment
The primary endpoints, evaluated before and at 1 and 3 months after surgery, were bilateral operation time and dyspnea severity. Operation time was defined as the interval from the start of the surgery, following anesthesia induction, to the withdrawal of the suspension laryngoscope. Dyspnea severity was measured using the Dyspnea Severity Index (DSI) as described by Gartner-Schmidt et al. A DSI score exceeding 10 was deemed abnormal. 17
Secondary endpoints, assessed before and 1 and 3 months after surgery, included vocal subjective and objective assessments, LVS images, and the Voice Handicap Index-10 (VHI-10) score. The subjective evaluation of voice quality was completed using the Grade, Roughness, Breathiness, Asthenia, and Strain (GRBAS) scale. 18 The objective assessment was conducted using the Multi-Dimensional Voice Program software (Kay Elemetrics Corporation, Lincoln Park, NJ, USA), which recorded the fundamental frequency (F0), jitter, shimmer, noise-to-harmonic ratio (NHR), and phonation time. 5 All patients were instructed to pronounce the vowel “a” for at least 3 s in a quiet room. The maximum phonation time (MPT) was assessed during sustained vowel “a” production following deep inspiration, at conversational pitch and loudness level, using a stopwatch.
LVS images were independently reviewed by two otolaryngologists who evaluated disease regression following surgery. They assessed parameters such as vibratory, symmetry, mucosal wave, and glottic closure. The inter-rater variability was calculated to assess the reliability of the reported findings. The VHI-10 score was based on the description provided by Rosen et al. 19
Surgical Procedures
All surgical interventions were performed via video-assisted laryngoscopy under general anesthesia. RE was treated with either CS surgery or RF coblation following surgical exposure. All operations were carried out by the same surgeon, with bilateral vocal fold lesions addressed during the same procedure.
CS Surgery Group
During the operation, a lateral microflap technique was employed to longitudinally incise the mucosa using laryngeal microsurgical scissors along the junction of RE and the normal mucosa of the vocal cord’s upper surface. The flap was elevated below the RE using a microflap elevator. The lower surface of the vocal cords was preserved with special attention paid to retaining 2-3 mm of the anterior commissure mucosa. After the jelly-like substance within the Reinke’s space beneath the mucosa was removed, the medial mucosa was replaced, and the excessive mucosa was carefully trimmed and excised.
RF Coblation Group
The RF coblation system (China Micro Medical Limited Shanghai Micro Medical Devices Co., Ltd. Shanghai city, China) was utilized, with a preference for the Evac 70 Plasma wand. Throughout the procedure, the Evac 70 wand was set at an ablation power of 7 and a coagulation power of 3.
RF coblation began with a mucosal incision that was ablated using the plasma blade into the superior surface of the vocal fold. The mucosa was ablated along the entire length of the vocal fold edges, from the vocal process of the arytenoid cartilage through the anterior commissure, preserving 2 mm of the mucosa near the anterior commissure.
A portion of the RE was removed using laryngeal microsurgical instruments and sent for pathological examination. Then the accumulated fluid within the Reinke’s space was suctioned using the plasma blade, and the redundant vocal fold mucosa was ablated using the plasma blade (with a coagulation setting of 3). Mucosal excision continued until the desired contour was achieved at the vocal fold’s medial border. No microsurgical retraction instruments were used. During the suction and excision procedures, utmost care was taken to avoid damaging the vocal ligament (Figure 2). The remaining mucosa was gently redraped over the vocal ligament using a microsurgical instrument.

(A) Preoperation. (B and C) radiofrequency coblation. (D and E) postoperative 3 months.
Follow-up
Patients were discharged the day after surgery and instructed to maintain strict voice rest for 7 days. They were also strongly advised to quit smoking. All patients were prescribed postoperative antireflux therapy with PPIs for 3 months. Follow-up appointments were scheduled at 1 and 3 months after surgery. The vocal folds’ condition, mucosal wave propagation, and potential recurrence of RE were evaluated via LVS. Perceptual and acoustic voice analyses were conducted at each visit. Preoperative voice analysis results were compared to postoperative findings using the Wilcoxon test. A P-value smaller than .05 was considered statistically significant.
Results
Demographic Data
This study included 33 patients in the CS surgery group and 28 in the RF coblation group. Histologic examination found no malignancies. All patients were smokers and had successfully quit smoking at least 4 weeks before the operation and continued to do so after the surgery. As shown in Table 1, the demographic data, including sex, age, RF grading, smoking rate, smoking duration, comorbid LPRD, preoperative VHI-10 scores, and abnormal DSI rates, were comparable between the two groups. Bilateral vocal fold lesions were operated on during the same surgery for all patients in both groups. The mean bilateral operation time was 38.4 ± 5.2 min in the CS surgery group and 24.2 ± 3.9 min in the RF coblation group (P = .041).
Demographic Data of Two Groups.
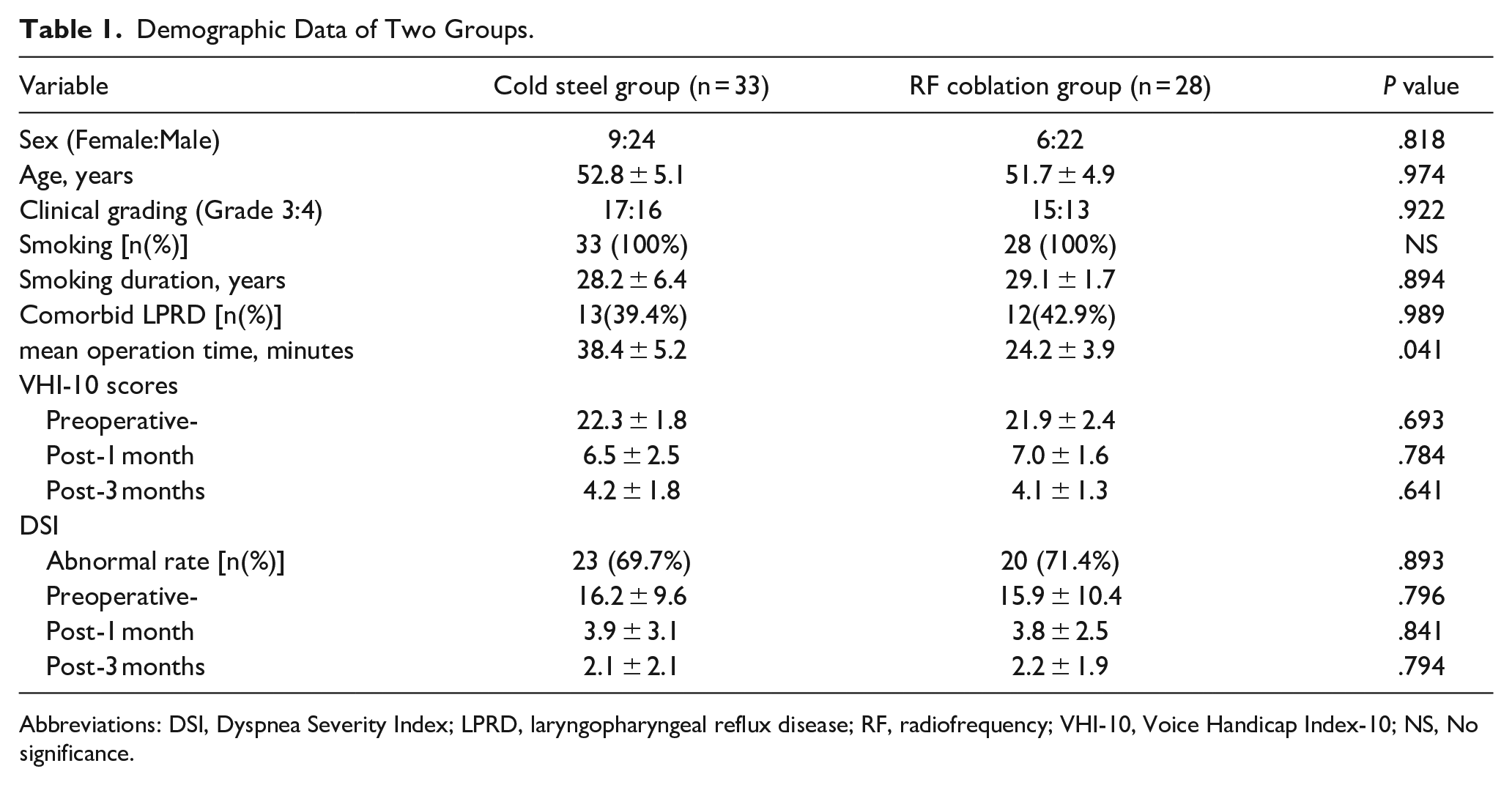
Abbreviations: DSI, Dyspnea Severity Index; LPRD, laryngopharyngeal reflux disease; RF, radiofrequency; VHI-10, Voice Handicap Index-10; NS, No significance.
DSI Before and After Therapy
Before surgical intervention, an abnormal DSI, that is, above 10, was observed in 23 out of 33 patients in the CS group and 20 out of 28 (71.4%) in the RF coblation group. A decrease in the DSI score was noted after surgery in all patients across both groups. No patients exhibited an abnormal DSI after surgery in either group.
In the CS group, the average DSI score significantly decreased from 16.2 ± 9.6 before surgery to 3.9 ± 3.1 1 month postoperation (P < .001) and further to 2.1 ± 2.1 3 months postoperation (P < .001). In the RF coblation group, the average score dropped from 15.9 ± 10.4 before surgery to 3.8 ± 2.5 1 month after surgery (P < .001) and to 2.2 ± 1.9 3 months after surgery (P < .001). However, no significant differences were noted between the two groups preoperation, and at 1 month and 3 months postoperation.
Voice Assessment
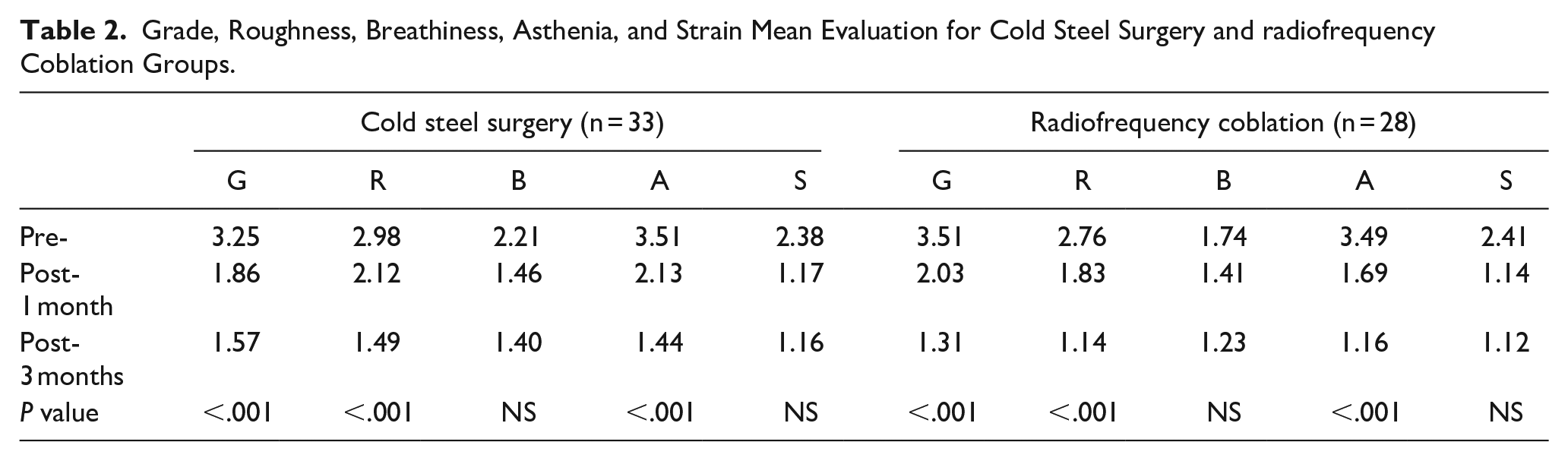
All patients reported improvement in their voice, noting it was no longer as rough or heavy. The perceptual pre- and postoperative voice evaluation in the GRBAS scoring system is presented in Table 2. All patients in both groups saw improvement in their GRBAS scores after surgery. However, the improvement was more pronounced in the RF coblation group compared to the CS group regarding hoarseness, roughness, and asthenia (P < .001). There were no statistically significant differences in breathiness and strain between the two groups.
Grade, Roughness, Breathiness, Asthenia, and Strain Mean Evaluation for Cold Steel Surgery and radiofrequency Coblation Groups.
Every patient experienced a decrease in their VHI-10 score (Table 1). The average score in the CS group decreased from 22.3 ± 1.8 before surgery to 6.5 ± 2.5 1 month postoperation (P < .001), and further to 4.2 ± 1.8 3 months postoperation (P < .001). In the RF coblation group, the average score significantly dropped from 21.9 ± 2.4 before surgery to 7.0 ± 1.6 1 month postoperation (P < .001), and to 4.1 ± 1.3 3 months postoperation (P < .001). Yet, there were no significant differences between the two groups preoperation, and at 1 month and 3 months postoperation.
Pre- and postoperative acoustic voice analyses are presented in Table 3. All patients demonstrated an improvement in acoustic voice parameters (F0, jitter, shimmer, NHR, and MPT) after surgery in both groups. This trend of improvement was evident from 1 month to 3 months postoperation in both groups, yet no significant differences were found between the two groups.
Voice Parameters in Cold steel surgery and radiofrequency Coblation groups.
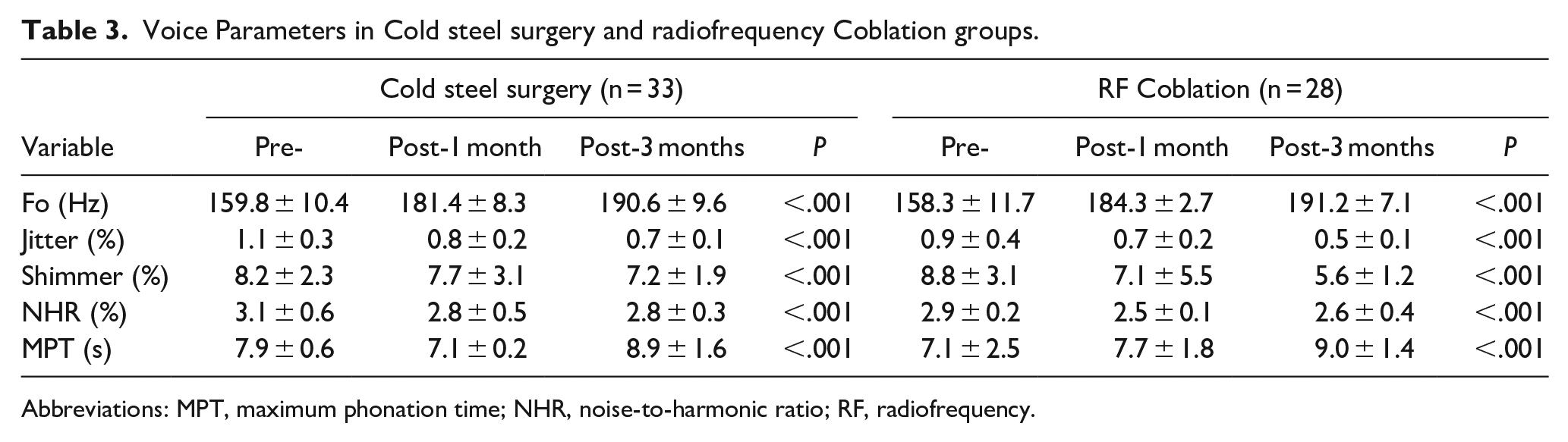
Abbreviations: MPT, maximum phonation time; NHR, noise-to-harmonic ratio; RF, radiofrequency.
The results of the pre- and postoperative morphological analysis conducted with LVS in both groups are given in Table 4. The inter-rater reliability analysis showed an intraclass correlation coefficient of .712, indicating excellent consistency between the two otolaryngologists who evaluated the endoscopic laryngeal findings. No recurrence of lamina propria edema was observed post-surgery in either group (Figures 2 and 3). There was no degradation of the mucosal waves in any of the cases in both groups, and no vocal fold scarring or stiffening were noted. No postoperative complications, including postoperative granulation tissue hyperplasia or anterior commissure adhesion, were found in either group. All patients across both groups showed significant improvement in all ratings (vocal fold symmetry, wave, and glottis closure) and this trend persisted from 1 month to 3 months postoperation. However, no significant differences were noted between the two groups.
Pre- and Post-Operative Ratings for Vocal Fold Symmetry, Wave, and Glottis closure.
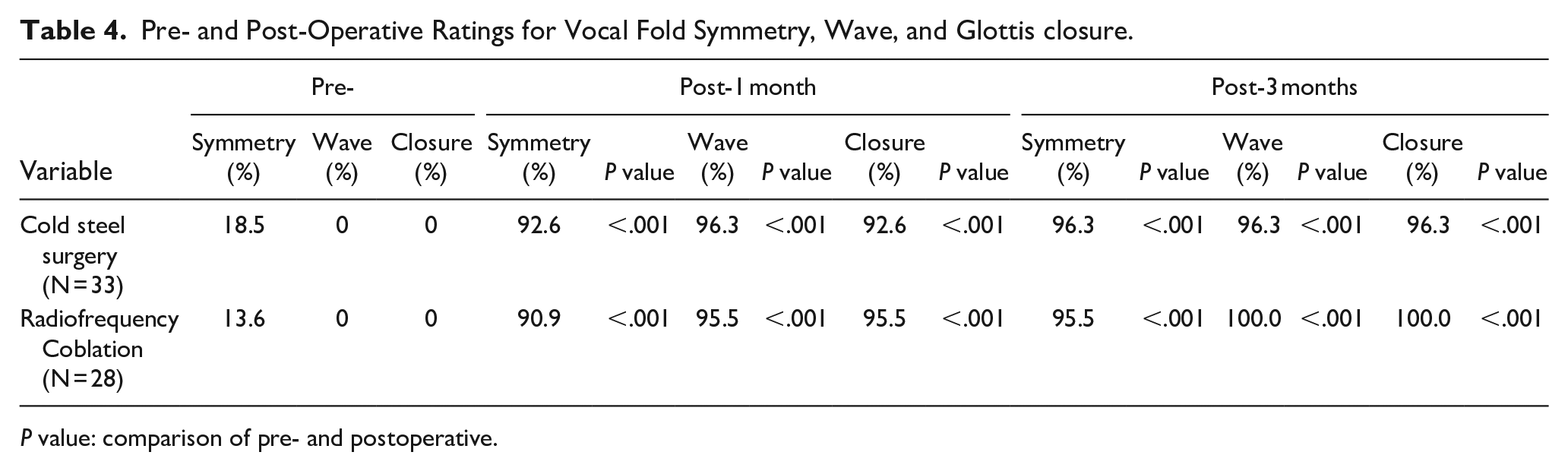
P value: comparison of pre- and postoperative.
(A) preoperative. (B and C) postoperative 12 months.
Discussion
The primary objective of RE surgery is to remove the mucous that accumulates in Reinke’s space and excise the redundant mucosa while preserving the structure of the vocal folds to the maximum extent possible, thereby improving voice quality.1,2,4 Traditional CS microlaryngeal phonosurgery used to evacuate the edematous mucoid gelatinous fluid from Reinke’s space by creating a mucosal incision, resulting in a bloody operative field. This obscured the clear visualization of the surgical plane, which makes it challenging to preserve the delicate structure of the vocal cords. It can also lead to prolonged aphonia and increased risk for anterior glottic web formation.5,11,20 Furthermore, the microflap surgery technique prevents clear visualization of the surgical plane and can lead to the hydrodissection of the normal basement membrane from the superficial lamina propria. Despite the use of Hirano’s microflap technique in recent years, normal mucosal waves are rarely restored. 6
The microdebrider has gained popularity due to its oscillatory knife that can gently remove a pathology with adjustable suction pressure, offering a less invasive approach and preserving the underlying lamina propria and vocal ligament. However, Grigaliute et al 9 compared the microdebrider technique with the CS technique and found significant improvements in vocal parameters and VHI-10 for both patient groups.
Laser surgery has recently been introduced as a treatment for RE.6-8 Some researchers have observed improvements in subjective and objective voice assessments following laser surgery for RE.6,7 Nevertheless, the use of CO2 lasers in treating RE has been questioned due to the potential for heat dispersion to normal surrounding tissue after complete suction of the edema fluid, leading to vocal fold scarring.11,20 Murry et al 6 compared Hirano’s microflap technique, CO2 laser, and CS phonosurgery and found that the duration of postoperative dysphonia was longest with laser removal. Burduk et al 8 observed significant improvements in all voice parameters in both the CO2 laser and microdebrider groups, but the improvements were greater after microdebrider surgery.
Although the potassium titanyl phosphate laser (KTP) and pulsed dye laser (PDL) have superior voice outcomes in non-contact mode compared to CO2 laser resection of RE, the outcomes depend on the energy delivered and the exposure time of KTP or PDL. These techniques require multiple procedures in at least 20% of patients and can result in postoperative airway compromise and worsening voice.4,21-23 Furthermore, KTP or PDL lasers are particularly effective for patients with mild to moderate RE but less so for severe cases. 1 As such, some researchers maintain that no single method to date has been definitively proven to be superior for improving voice in the treatment of RE.1,7
This study was the first to apply the RF coblation technique to treat RE. Our findings suggest that although all patients experienced an improvement in their GRBAS scores after surgery in both groups, the improvements were more significant in the RF coblation group than in the CS group for grades of hoarseness, roughness, and asthenia. However, although all patients had a significant decrease in their VHI-10 scores from before surgery to 1 month and 3 months post-surgery in both groups, no significant differences were found in the decrease in mean score between the two groups. Similarly, all patients had a significant improvement in all objective acoustic voice parameters after surgery in both groups, with both groups showing improvement from 1 month postop to 3 months postop, but no significant differences were found between the two groups. Postoperative morphologic analysis confirmed good results in both groups, with slightly better function among patients operated on with RF coblation.
In recent years, the RF coblation technique has been increasingly used to treat granuloma,13,14 laryngeal carcinomas, 15 and oropharyngeal tumors 12 in otolaryngological clinics. The RF coblator operates between 40°C and 70°C, causing minimal surrounding tissue damage and preserving the integrity of surrounding tissue, thereby overcoming the collateral thermal injury caused by lasers. 12 In addition, RF has simultaneous coblation, cautery, hemostasis, and suction functions in one instrument, which ensures a bloodless operative field and eliminates the need for different instruments, thereby shortening operation time and promoting wound healing. In addition, the plasma knife of RF coblation can bend over a larger range, benefiting the adjustment of the angle for unfavorable laryngoscopic exposure during operation. In this study, RF coblation significantly shortened the mean operation time compared to the CS surgery group for bilateral surgery.
All patients underwent a 3-month antireflux therapy with PPIs as a standard protocol in both groups. Based on previous clinical studies, it is understood that controlling laryngopharyngeal reflux (LPR) helps prevent postsurgical scarring and reduces the recurrence of RE. 7 In this study, all subjects exhibited no recurrence of lamina propria edema after surgery in both groups. There was no worsening of the mucosal waves in any of the cases and no vocal fold scarring or stiffening were noted. Furthermore, no postoperative complications, including granulation tissue hyperplasia or anterior commissure adhesion, were found in either group. Thus, the RF coblation procedure offers a reliable and safe method for treating RE and establishes itself as an effective treatment option for RE. However, this study had some limitations, including its retrospective nature, limited number of subjects, and relatively short follow-up period. In addition, there was no objective measure of dyspnea. Future studies should conduct randomized controlled trials and investigate long-term outcomes.
Conclusion
The RF coblation procedure provides a reliable and safe method for RE surgery and is an effective treatment option for RE.
Footnotes
Authors’ Note
Author Contributions
Xudan-Lou: Interpretation of data for the work, analysis of data for the work, drafting the work and technical the diagram, agreement to be accountable for all aspects of the work, and final approval of the version to be published. Zhengcai Lou: Interpretation of data for the work, design of the work, analysis of data for the work, drafting the work, agreement to be accountable for all aspects of the work; final approval of the version to be published.
Data Availability Statement
All data generated or analyzed during this study are included in the published article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Technology Agency of Yiwu city, China (Grants#2021-3-55).
Ethical Statement
The study protocol was reviewed and approved by the Institutional Ethical Review Board of Yiwu Central Hospital.