
Abstract
The term lymphoma includes a wide variety of different clinical entities including diffuse large B-cell lymphomas (DLBCL). Skeletal muscle or intramuscular lymphomas represent less than 2% of B-cell Lymphoma, they are quite rare, even more in the orofacial area. We present the case of a painless growing mass of the right cheek mimicking a chronic oral cellulitis in a 34-year-old man. Magnetic resonance imaging (MRI) of the mandible revealed a well-defined 7x3cm mass around the core of the mandible that invades the buccal floor and the subcutaneous planes. A whole-body 18F-FDG PET/CT for the initial diagnosis revealed an intensely isolated hypermetabolic band corresponding to a voluminous tumoral permeation. The diagnosis of a skeletal muscle diffuse large B-cell lymphoma was established after an intraoral biopsy. It was treated with 4 chemotherapy cures and showed complete remission at one year of follow-up. This atypical form of lymphoma should be integrated into the differential diagnosis of soft tissue tumors in the oral cavity.
Introduction
The term lymphoma includes a wide variety of different clinical entities. Diffuse large B-cell lymphomas (DLBCL) are part of non-Hodgkin lymphomas. They are known as abnormal proliferation of B lymphocytes within the lymph nodes or lymphatic tissues of different organs, in which case they are called extranodal lymphomas. Skeletal muscle or intramuscular lymphomas represent less than 2% of B-cell lymphomas.1-4 They are rare and even more exceptional in the orofacial area.
Here, we report the case of a DLBCL diagnosed within our department. The diagnostic process for this pathology is described below.
Case report
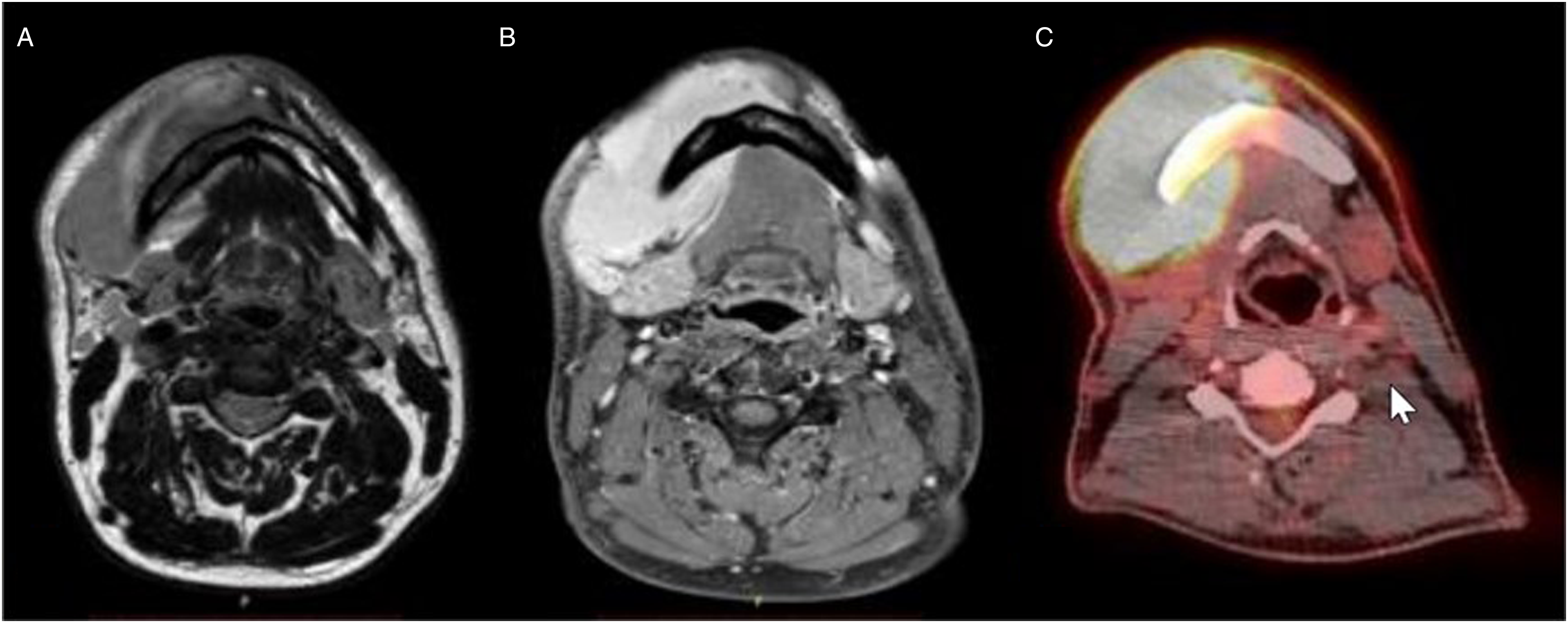
A 34-year-old man patient with no notable medical history except smoking, presenting a 2-month history of a painless growing mass of the lower right cheek that mimics a submandibular cellulitis. Intraoral examination showed no purulent discharge or teeth mobility. The patient was initially unsuccessfully treated with antibiotics for a dental cellulite while experiencing a few labial hypesthesia episodes. At presentation, the panoramic radiography and CT scan revealed no mandibular infection while injected CT scan (Figure 1) and musculoskeletal MRI (Figure 2) showed a well-defined 7x3cm mass around the core of the right mandible. The mass exhibited an isointense signal on T1-weighted images (Figure 2A) and an intermediate signal between muscle and fat on T2-weighted images (Figure 2B). Non-injected CT (A) and injected CT (B) showing the left jugal tumor around the core of the mandible invading the buccal floor. MRI T1-weighted image with an isointense signal (A). MRI T2-weighted image with an intermediate signal between fat and muscle (B). F-18 FDG PET-scan of the tumor (C).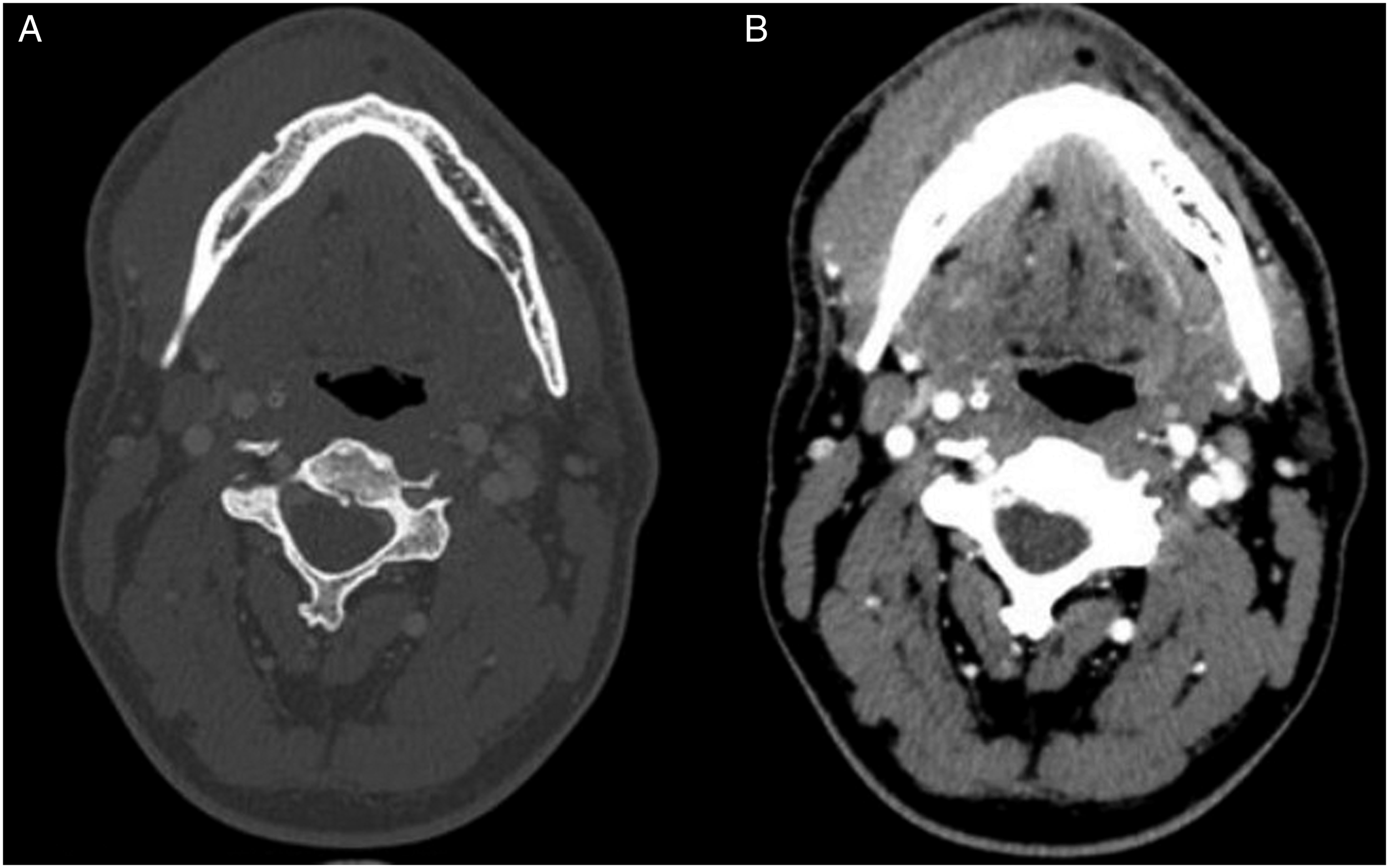
The hypothesis of a dental cellulitis was therefore discarded. The possibility of a benign or malignant tumor was considered, with fibrosarcoma and myosarcoma as main differential diagnoses. Their benign forms, such as fibroma were also considered. An intraoral biopsy was performed and revealed a diffuse large B-cell lymphoma (DLBCL), not otherwise specified, of the germinal center B-cell-like subtype, according to the Hans classification. The lesion is described as a massive infiltration of the muscular tissue by large cells and lymphocytes (Figure 3A). The cells presented an irregular and sometimes multilobe nucleus with light chromatin. Immunohistochemistry showed strong expression of CD20 (Figure 3B) and BCL6. It also showed expression of MYC in 20% of tumor cells with no reshuffle, but no expression of BCL2. The proliferative index was high, estimated at 70% by Ki67. EBER was not detected by fluorescent in situ hybridization. Hemalun-eosin-saffron staining (A) (magnification x400). CD20 immunochemistry is highly positive on biopsy (B) (magnification x200).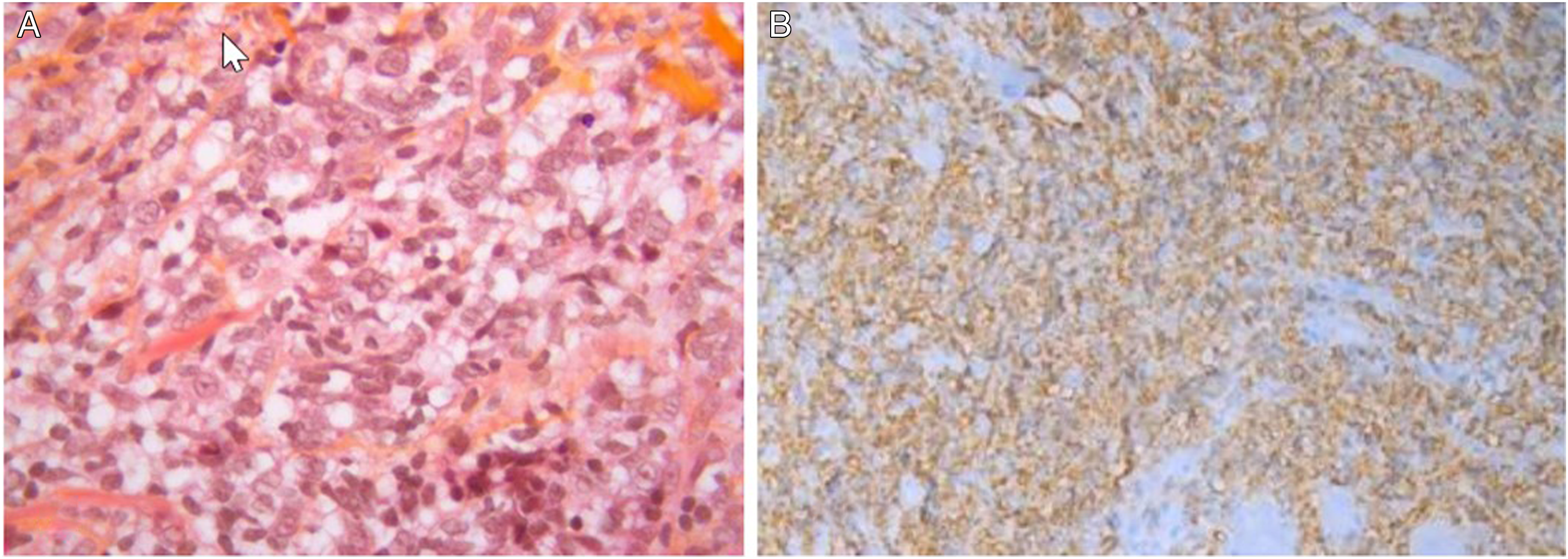
A whole-body 18F-FDG PET/CT for initial staging was performed and revealed an intensely hypermetabolic band (SUV max.16,0), corresponding to a voluminous tumoral permeation of the right jugal and chin cutaneous and subcutaneous planes (80 x 55 x 80 mm). Towards the mandible’s internal part, the tumor extended into the buccal floor. No loss of continuity of the mandibular bone was observed (Figure 2C). Furthermore, a hypermetabolic site located higher within the right ramus (SUV max 8,4) and a moderately hypermetabolic site on lymph nodes level I (SUV max. 2,5; 8mm in left IB group) and level II (SUV max. 3,8; 6mm in right IIA group) were detected. The left cervical lymph nodes were infra-centimetric and significantly nonfixating. There was no other suspicious hypermetabolic focus on the remainder PET.
The lymphoma was thus considered stage I in the Ann Arbor classification, with a low-risk Age-Adjusted International Prognostic Index of 1. The treatment consisted in an intensified CHOP-like chemotherapy (ACVP, doxorubicin, cyclophosphamide, vindesin, and prednisone) plus rituximab, followed by a sequential consolidation with high-dose methotrexate, rituximab, ifosfamide, etoposide, and cytarabine. 5 The lymphoma showed a great sensibility to chemotherapy. After one-year of follow-up, PET-scan confirmed a complete metabolic response. The facial swelling completely disappeared while a few infra-centimetric jugular-carotid lymph nodes remained.
Discussion
Lymphomas are the third most common type of cancer in the oral cavity,6,7 representing 5% of all cancers 6 after squamous cell carcinomas and basal cell carcinomas. 7 DLBCLs are the most common lymphomas in the orofacial region 7 . Non-Hodgkin lymphoma may appear in an extranodal site in 40% of the cases,6,8 2 to 3% of these cases may arise in the oral region. 8 In DLBCL cases, the muscular invasion can come from the spreading of lymphatic cells from another tumoral site or by lymphomatous deposits coming from the adjacent bone or lymph nodes. 9 In rare cases, such as ours, the invasion can be caused by a primary lesion.1,8,10 Salivary glands, hard palate and soft palate tonsils are the most frequent sites.2,6 They represent only 0.1% to 1.4% of all extranodal lymphomas,1-4,11 and 1.2 to 2% of muscle tumors with a majority of DLBCL. 11 To our knowledge, this is the first case of an intramuscular lymphoma in the orofacial area reported in the literature.
Several authors studied the MRI aspect and features of primary muscle lymphoma, reporting a higher prevalence in the tight and the arm.12,13 In 75% of the cases the initial manifestation was a muscular mass. The MRI aspect of muscle lymphoma seems to be specific. As first reported in the literature, the muscle involvement showed a hypointense or isointense signal on T2-weighted images. 14 In more recent studies, with improved of the imaging methods, some authors showed that in T1-weighted MRI images, muscle lymphoma appears as an isointense signal and in T2-weighted images as an intermediate signal.12,15 The CT aspect seems to be an ill-defined mass in the soft tissues, difficult to discern and sometimes infiltrating the fat and skin planes.13,16,17
The diagnosis of lymphomas is based on the biopsy and the histopathological study which allows to determine the exact type of lymphoma. Choudhury et al. 9 recommend fixing histological sections with a mix of acetic acid and ethanol which allows more specific results with cytological studies, electronic microscopy, or by the use of immunohistochemical markers. Recently, the use of immunohistochemistry allowed a breakthrough in the molecular diagnosis of DLBCL for which a specific molecular signature can be revealed according to their GC (germinal center) or ABC (advanced B-cell) type. These two types of lymphomas do not have the same prognosis, the ABC ones being less favorable. 18
The prognosis of intramuscular DLBCL lymphomas is good and has progressed through the years with better treatment. 5-year survival rates vary from 50 to 80% through the different studies.3,6,8,19 In 1993, Ship et al. 20 identified the poor prognostic factors of lymphomas: an age greater than 60 years, a stage III or IV lymphoma according to the Ann Arbor classification, a number of extranodal sites superior than 1 and increased lactase dehydrogenase (LDH) levels. With these criteria, they created the IPI Index, which gives the lymphoma’s prognostic value according to the different clinical and patient characteristics. But the prognosis also depends strongly on an early diagnosis and the appropriate staging technique and extension assessment which determine the treatment. Our patient presented no aggravating factors and a good prognosis. Combined chemotherapy is the gold standard treatment for lymphoma,1,6 indeed after the initiation of chemotherapy the tumor size decrease rapidly. 6 A combination of chemotherapy with radiotherapy can be used in cases of extensive lymphomas with good results. 19 Surgery should only be limited to the excisional biopsy.3,6 In our case, the chemo sensibility of the lymphoma was high, and it responded well to 4 chemotherapy cures, controlled on PET-scan. Chemotherapy cures are usually followed by a consolidation phase with methotrexate.
Response assessment is usually controlled with an 18F-FDG PET-scan and sometimes in association with CT scan. Indeed, FDG Pet-scan as a high sensitivity and specificity to assess the lymphoma’s response to chemotherapy. 21 The association with CT scan could conduct to even higher results as showed by Allen-Auerbach et al. in 2004. 22 In this previous study, the CT is performed as part of a PET-CT, without using intravenous contrast product, so the association between PET-scan and CT scan could avoid the use of an intravenous contrast. 21
The differential diagnosis that should be considered are undifferentiated metastatic carcinomas, round cell sarcomas, 3 and benign tumors 19 by using histopathological examination along with immunohistochemistry (IHC). 4 The hypothesis of lymphoma must be taken into account when faced with an unexplained tumor of the soft tissues surrounding the jawbone. Oral manifestations of lymphomas are most often painless swellings or mass6,8,10,19 with or without ulceration and sometimes paresthesia (6%). 23 They can quite often mimic other clinical entities such as infections and the less common benign or malignant conjunctives and soft tissue tumors. 23 Diagnostic errors will unfortunately lead to delayed treatment. In some cases, it will lead to overtreatment (tooth extraction for example) or worse, to a loss of chance. When faced with facial swelling where no dental cause can be found, a benign or malignant tumor should be considered and ruled out with the help of an MRI and a biopsy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by APHP, INSERM U1138, and Gustave Roussy Cancer Campus.