
Abstract
A thyroglossal duct cyst is the most common congenital disease in the neck. There are two age groups usually associated with thyroglossal duct cysts: 1–11 years in children and 30–60 years in adults. These midline neck masses are typically located anteriorly in the neck, inferior to the hyoid bone. We report an extremely rare case of an intralaryngeal thyroglossal duct cyst without a neck mass, presenting with hoarseness as the sole symptom. A 64-year-old man presented with a 3-month history of hoarseness. On physical examination, no neck mass or swelling was observed during cervical palpation. Laryngostroboscopy revealed a large submucosal mass in the right glottis and supraglottis, and mobility of the right vocal cord was restricted. Surgery was performed via an external approach to completely resect the cyst, together with the middle part of the hyoid bone. Histopathologic examination of the cyst led to a diagnosis of thyroglossal duct cyst. The patient recovered well and his voice returned to normal. Attention should be paid to the occurrence of rare types of thyroglossal duct cyst in unusual clinical sites. Adequate radiological examinations should be performed, and reading the computed tomography or magnetic resonance imaging scans carefully before surgery is important to avoid misdiagnosis.
Introduction
A thyroglossal duct cyst is the most common congenital disease in the neck. Its occurrence is related to abnormal embryonic development of the thyroglossal duct, and it can occur in any part of the midline of the neck between the foramen cecum of the tongue and the suprasternal notch. Most patients are adolescents. Thyroglossal duct cysts are typically located anteriorly in the neck, inferior to the hyoid bone, and are closely related to the thyrohyoid membrane. 1 However, intralaryngeal extension of a thyroglossal duct cyst is rare, particularly without a neck mass; only five cases have been reported in the English medical literature.2-6
We report an extremely rare case of an intralaryngeal thyroglossal duct cyst without a neck mass, presenting with hoarseness as the sole symptom, together with a review of the relevant English medical literature. To the best of our knowledge, this is the first reported case of thyroglossal duct cyst with endolaryngeal extension, no mass in the neck, and limited vocal cord mobility.
Case presentation
A 64-year-old male presented to the Department of Otolaryngology, The First Affiliated Hospital, College of Medicine, Zhejiang University (Hangzhou, China), with a 3-month history of hoarseness that was initially intermittent and improved slightly after vocal silence. After 2 months, the patient’s hoarseness became persistent, and no improvement was observed after resting his voice. The patient exhibited no pharyngeal pain, pharyngeal sensation of a foreign body, dyspnea, or dysphagia. His personal history included 10 years of smoking cigarettes and 40 years of drinking alcohol. The patient had a 3-year history of hypertension, which was well-controlled by medication. His medical history was otherwise unremarkable.
On physical examination, no neck mass or swelling was observed during cervical palpation. Laryngostroboscopy revealed a large submucosal mass in the right glottis and supraglottis (Figure 1). The surface mucosa of the mass was smooth, and mobility of the right vocal cord was restricted. Of note, the laryngeal inlet was significantly smaller than normal, but the patient had no dyspnea. Based on the hoarseness and laryngoscopy results, a preliminary diagnosis of laryngeal tumor was made and the patient was scheduled for further examination.
Magnetic resonance imaging (MRI) with contrast enhancement of the neck was performed to assess the nature and extent of the lesion, and revealed a 4.0 cm × 4.0 cm× 3.5 cm cystic mass containing T1 hypointense and T2 hyperintense homogeneous fluid, with no enhancement in the right pre-epiglottic or paraglottic spaces (Figure 2). The appearance of the thyroid gland was normal. According to the MRI findings, we made a preliminary diagnosis of laryngeal cyst.
Due to the large mass, complete resection through an endolaryngeal approach would have been very difficult, so we planned an external approach. The operation was performed under general anesthesia. A transverse skin incision was made at the level of the hyoid bone. After separating the strap muscles, a cystic mass was observed above the thyroid notch adherent to the hyoid bone, which was pressing the right false vocal cord, laryngeal ventricle, and vocal cord downward along the right paraglottic space, and the epiglottis and the right aryepiglottic fold backward. A thyroglossal duct cyst was considered. The mass was separated and the hyoid bone was exposed upward; finally, the cyst was resected together with the middle part of the hyoid bone, as in the technique described by Sistrunk (Figure 3). Histopathologic examination of the cyst confirmed the diagnosis of thyroglossal duct cyst.
The patient recovered uneventfully and was discharged 3 days after surgery. His voice returned to normal and there was no recurrence during the 4-year of follow-up.
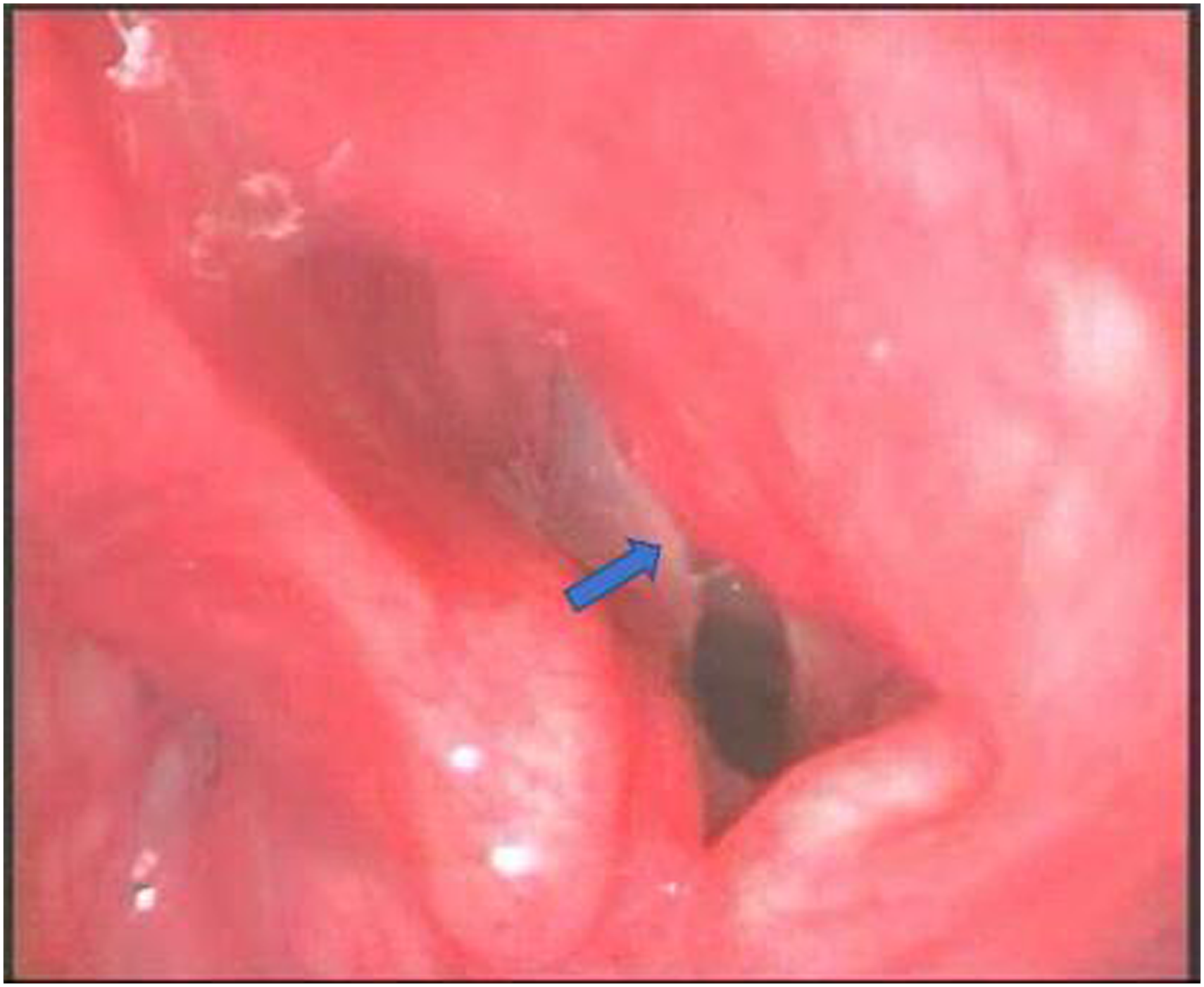
Laryngostroboscopy showed a large submucosal mass in the right glottis and supraglottis. The laryngeal inlet was markedly narrowed.
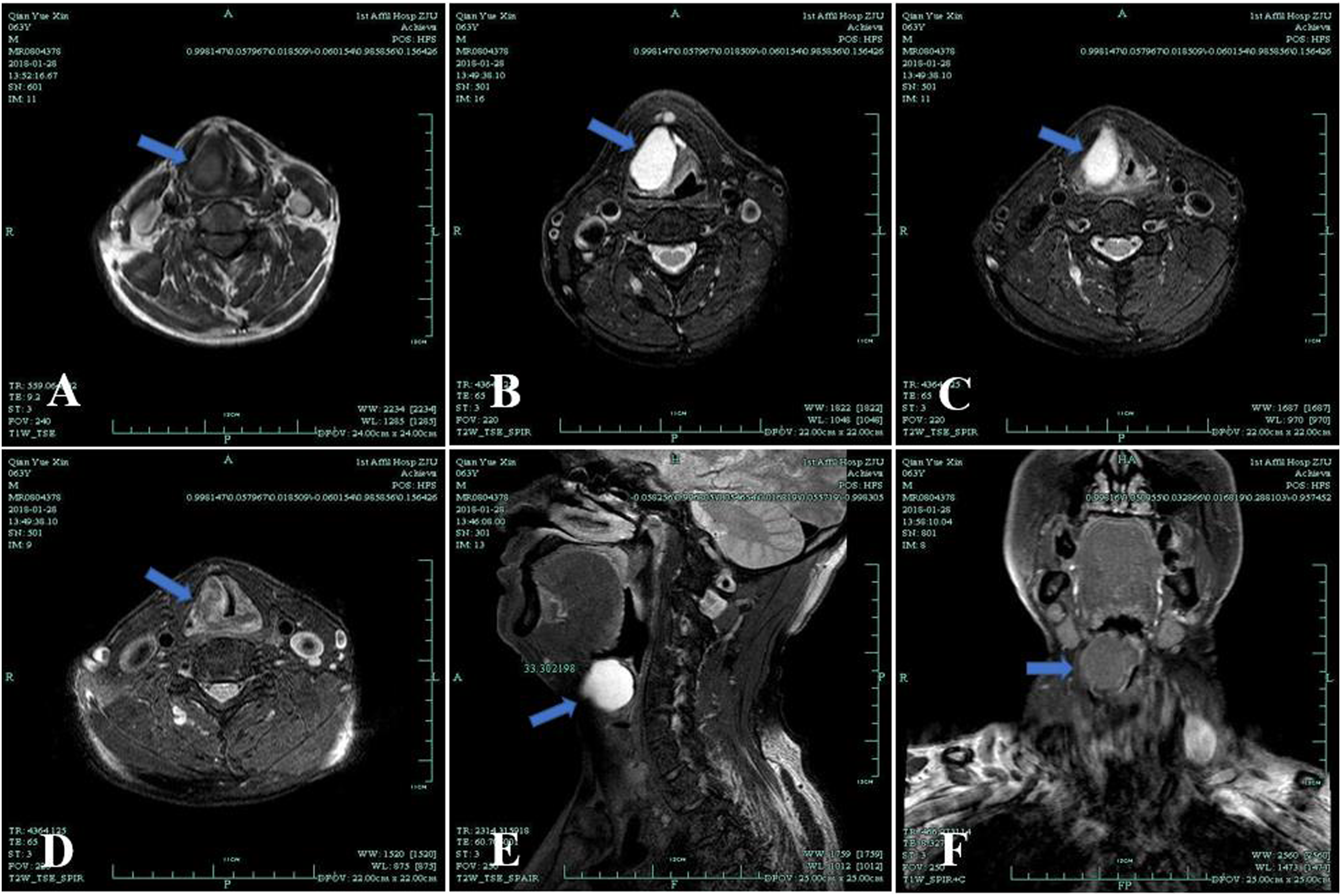
MRI with contrast enhancement of the neck revealed a cystic mass containing T1 hypointense (A), T2 hyperintense homogeneous fluid (B, C, D, E), and no enhancement (F) located in the right pre-epiglottic and paraglottic spaces.
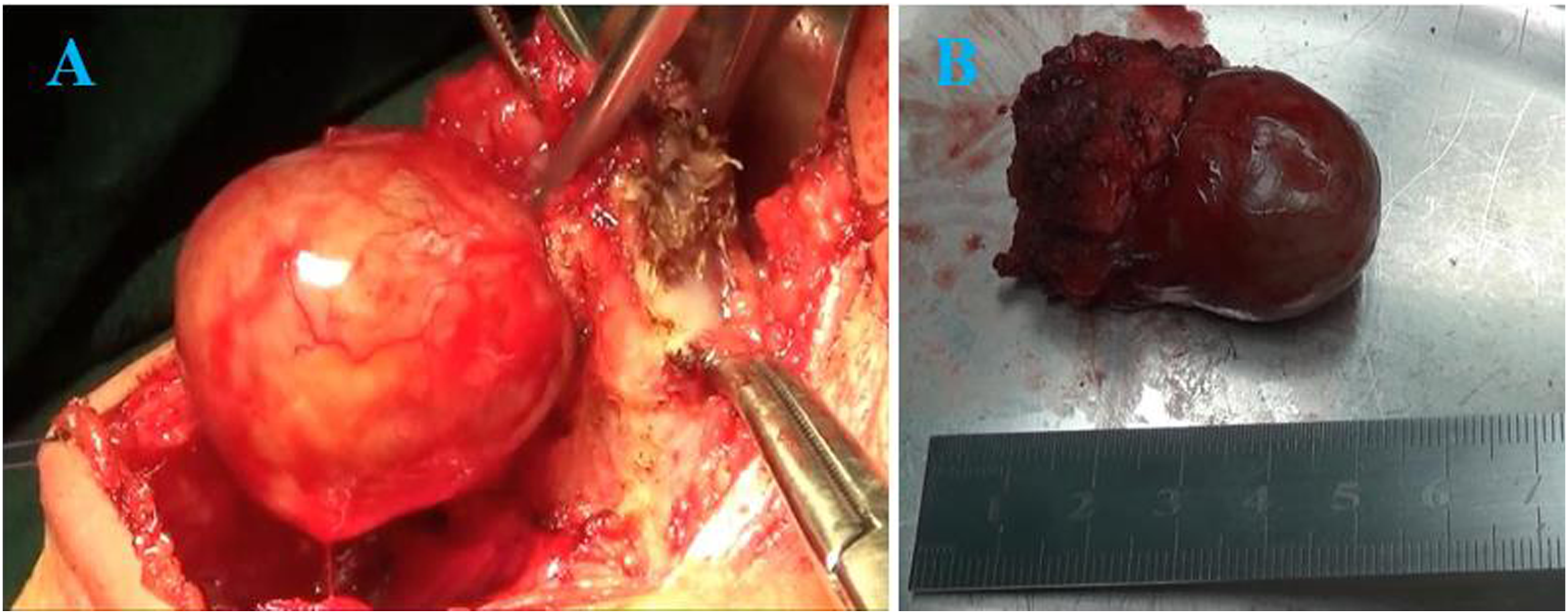
Intraoperative image of the cyst showed the mass was closely adhered to the hyoid bone and pressed the right pre-epiglottic and paraglottic spaces (A). The mass was measured to be about 4cm (B).
Discussion
We reviewed the English medical literature in the MEDLINE database, using the search terms “intralaryngeal” OR “endolaryngeal” OR “laryngeal extension” OR “endolaryngeal extension” AND “thyroglossal duct cyst”.
Intralaryngeal extension of thyroglossal duct cyst without neck mass reported in English-language literature.
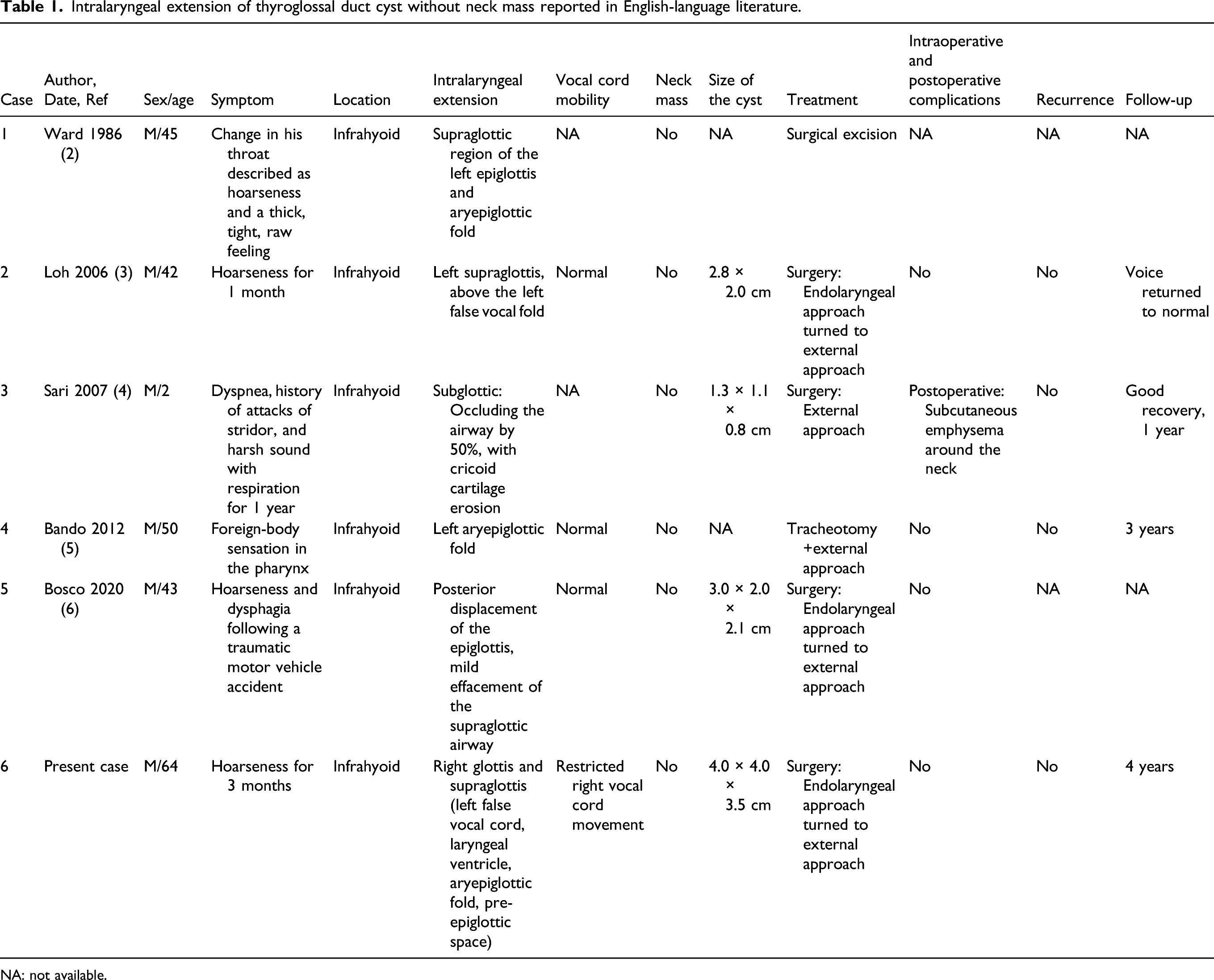
NA: not available.
There have been previous reports of intralaryngeal thyroglossal duct cyst with hoarseness as the initial symptom. 3 However, extensive compression of the paraglottic space with limited vocal cord movement and no neck mass has not been reported, so this case was more likely to be misdiagnosed as a laryngeal mass. Surgery via suspension laryngoscopy will result in incomplete removal of the cyst, with relapse likely after surgery; laryngofissure will thus be necessary, which can destroy the normal structure of the larynx and cause internal injury, resulting in long-term or even permanent hoarseness.7,8
This case showed that computed tomography (CT) or MRI scans should be read carefully before surgery, and observations and positioning should be performed in the axial, coronal, and sagittal planes. Particularly in the sagittal view, if the cystic mass is located in the pre-epiglottic space and the pedicle protrusion is closely related to the hyoid bone, thyroglossal duct cyst can be diagnosed. Therefore, special attention should be paid to the occurrence of rare types of thyroglossal duct cyst in unusual clinical sites. All relevant examinations should be performed before surgery, and a comprehensive analysis should be performed based on the medical history, physical examination, and imaging results, to avoid misdiagnosis and unnecessary damage due to inappropriate treatment measures.
Conclusions
Intralaryngeal extension of a thyroglossal duct cyst without a neck mass is extremely rare. Adequate radiological examinations should be performed, and careful interpretation of the CT or MRI scans before surgery is important to avoid misdiagnosis.
Footnotes
Acknowledgments
We would like to thank for the support by Scientific Research Fund of Zhejiang Provincial Education Department (NO. Y202045601) and Zhejiang Province Public Welfare Technology Application Research Project (No. LGF19H180018).
Author contributions
BYY and GYP designed and wrote the manuscript. ZXJ reviewed the references. DLB and GY made the pictures and the tables. ZSH and LW performed analysis of the data and revision of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Scientific Research Fund of Zhejiang Provincial Education Department (NO. Y202045601) and Zhejiang Province Public Welfare Technology Application Research Project (No. LGF19H180018).
Author’s note
All authors contributed to the article and approved the submitted version.
Informed consent
Written informed consent was obtained from the patient for the publication of any potentially identifiable images or data included in this article.