
Abstract
Thyroglossal duct cysts are typically benign and usually asymptomatic. Malignant transformation is uncommon. Intralaryngeal extension is rare and results in dysphonia or dyspnea. There is no literature nowadays reporting the thyroglossal duct cyst carcinoma combining the clinical features of intralaryngeal extension. The authors present a case of progressive hoarseness and midline neck mass for 2 years. The laryngoscope and computed tomography revealed a 6-cm thyroglossal duct cyst containing ectopic thyroid tissue with intralaryngeal extension and causing airway obstruction. Complete excision with Sistrunk operation revealed papillary thyroid carcinoma. The patient resumed normal phonation after the surgery. There was no evidence of tumor recurrence and no hoarseness or dyspnea at 6 months follow up. This is the first reported case of a huge thyroglossal duct cyst carcinoma with intralaryngeal extension causing airway compromise. Complete excision of tumor is essential and vital to the symptom relief. A thyroglossal duct cyst carcinoma with endolaryngeal involvement should be considered in the differential diagnosis when the case has a massive midline neck mass with ectopic thyroid tissue and develops dyspnea or hoarseness concurrently.
Keywords
Introduction
Thyroglossal duct cysts are common congenital lesions of the neck, occurring in 7% of the adult population and accounts for 70% of all congenital neck mass. 1 They commonly present as a midline upper neck mass between the hyoid bone and thyroid gland. Intralaryngeal extension is extremely rare and associated with dysphonia and dysphagia. 1
Clinically, most thyroglossal duct cysts are benign. Malignant neoplasms arising from thyroglossal duct cysts are uncommon, with an incidence of 1%. 2 Its clinical manifestations are usually indistinguishable from those of benign tumors.
To the best of our knowledge, there is no literature reporting that thyroglossal duct cyst carcinoma combining the clinical features of intralaryngeal extension. Here, we present such a rare case of thyroglossal duct cyst papillary carcinoma with intralaryngeal extension causing airway compromise.
Case Report
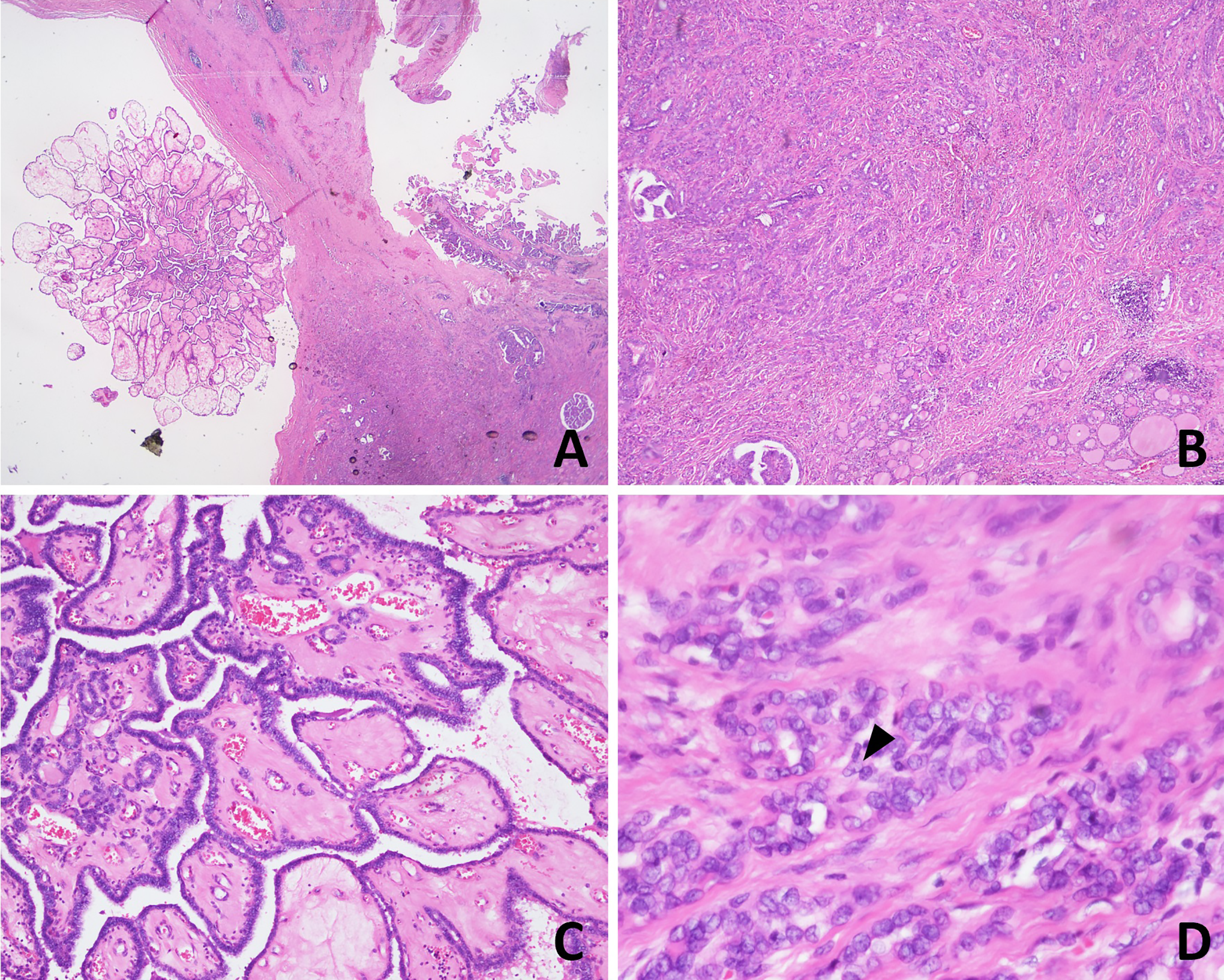
A 39-year-old man presented to our clinic with a midline neck mass and progressive hoarseness. The neck mass was not obvious until 2 years ago, when the patient lost more than 10 kg weight after an intracranial hemorrhage. Hoarseness, which was considered to be the neurologic deficit after stroke, was neglected at first. The patient’s medical history included hypertension. Physical examination revealed a 3-cm neck mass anterior to the thyroid cartilage. Flexible nasopharyngoscopy revealed a huge bulge at right false vocal cord with airway compromise (Figure 1A). Fine needle aspiration with drainage of 20 cc serous fluid was performed, and hoarseness improved immediately (Figure 1B). However, the symptoms recurred 3 weeks after the aspiration (Figure 1C). Computed tomography showed a 6-cm midline infrahyoid lobulated cystic mass containing calcification within the lesion and downward extension to right paraglottic space. The thyroid gland had a homogeneous appearance and was not attached to the lesion (Figure 2). After discussing with the patient, a Sistrunk operation was arranged. At surgery, a multilobulated thyroglossal duct cyst was noted above the thyroid cartilage notch and extended into the thyrohyoid membrane. The cyst was dissected and completely excised. Patient could resume normal phonation after surgery (Figure 1D). The pathohistology demonstrated a 7-cm thyroglossal duct cyst containing a 1.5-cm papillary thyroid carcinoma, classic type (Figure 3). Immunohistochemistry revealed positive results for thyroglobulin, cytokeratins, and cyclin D1. A low Ki-67 index (<5%) was noted. Blood samples of thyroglobulin, T3, T4, and thyroid-stimulating hormone were all within the normal range. Neck ultrasonography including thyroid gland and bilateral neck lymph node and aspiration cytology at neck level VI lymph node were also performed to rule out the possibility of metastasis from the primary thyroid gland or direct extension from ectopic thyroid tissue. Histopathology showed negative results for metastatic carcinoma. At 6-month follow-up, there was no evidence of tumor recurrence.
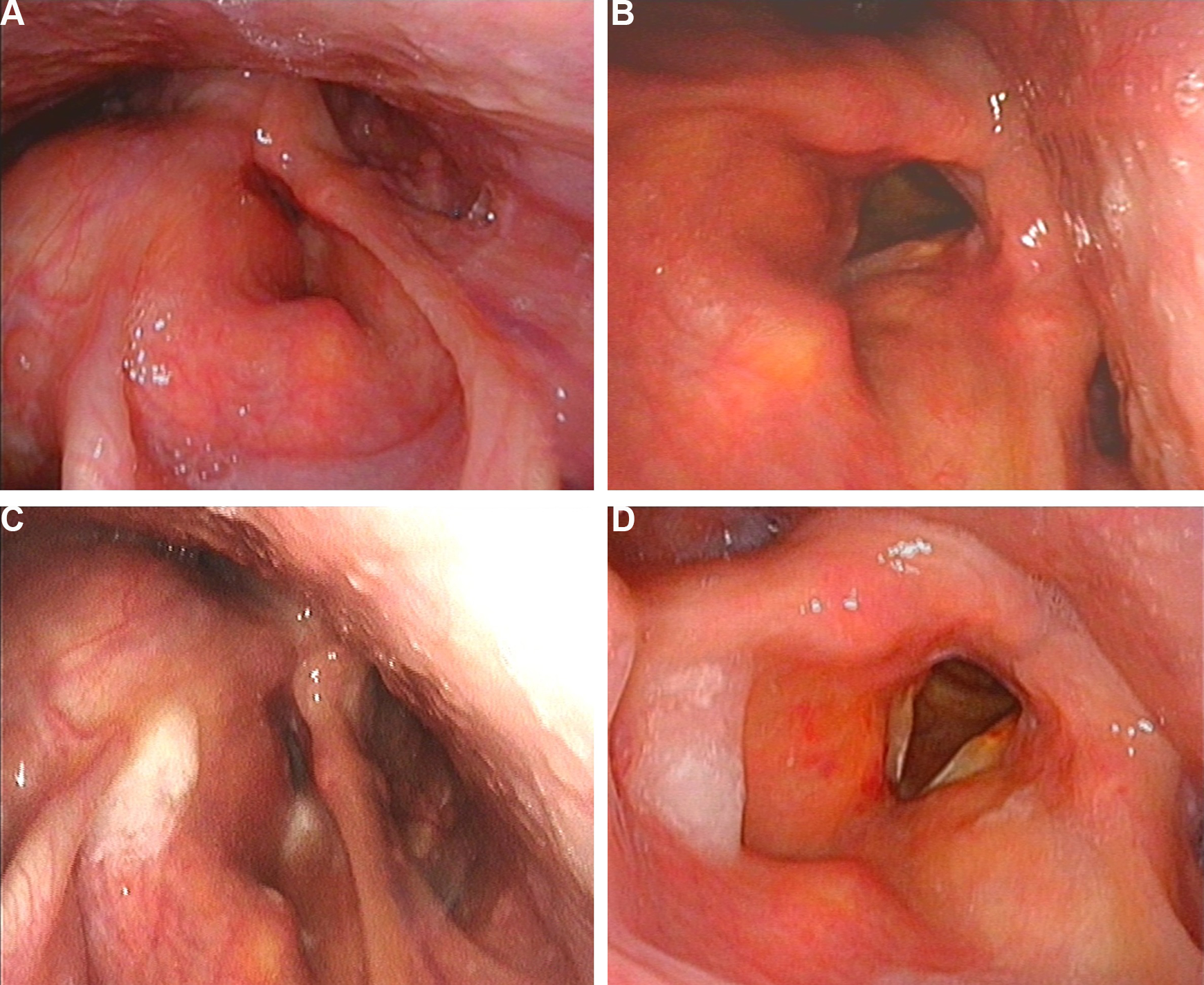
Flexible nasopharyngoscopy revealed (A) right bulging false vocal cord with airway compromise. (B) Larynx and airway was visible after fine needle aspiration. (C) A huge bulge recurred at right false vocal cord (D) intact larynx structure after Sistrunk procedure.
Computer tomography showed a 4.6 × 6.1 × 4.6 cm infrahyoid multilobulated cystic and dumbbell-shaped mass with downward extension to right vallecula and right paralaryngeal space (asterisk). The inferior portion of the lesion embedded in the strap muscle. Ectopic thyroid tissue with calcification is within the cyst (arrow).
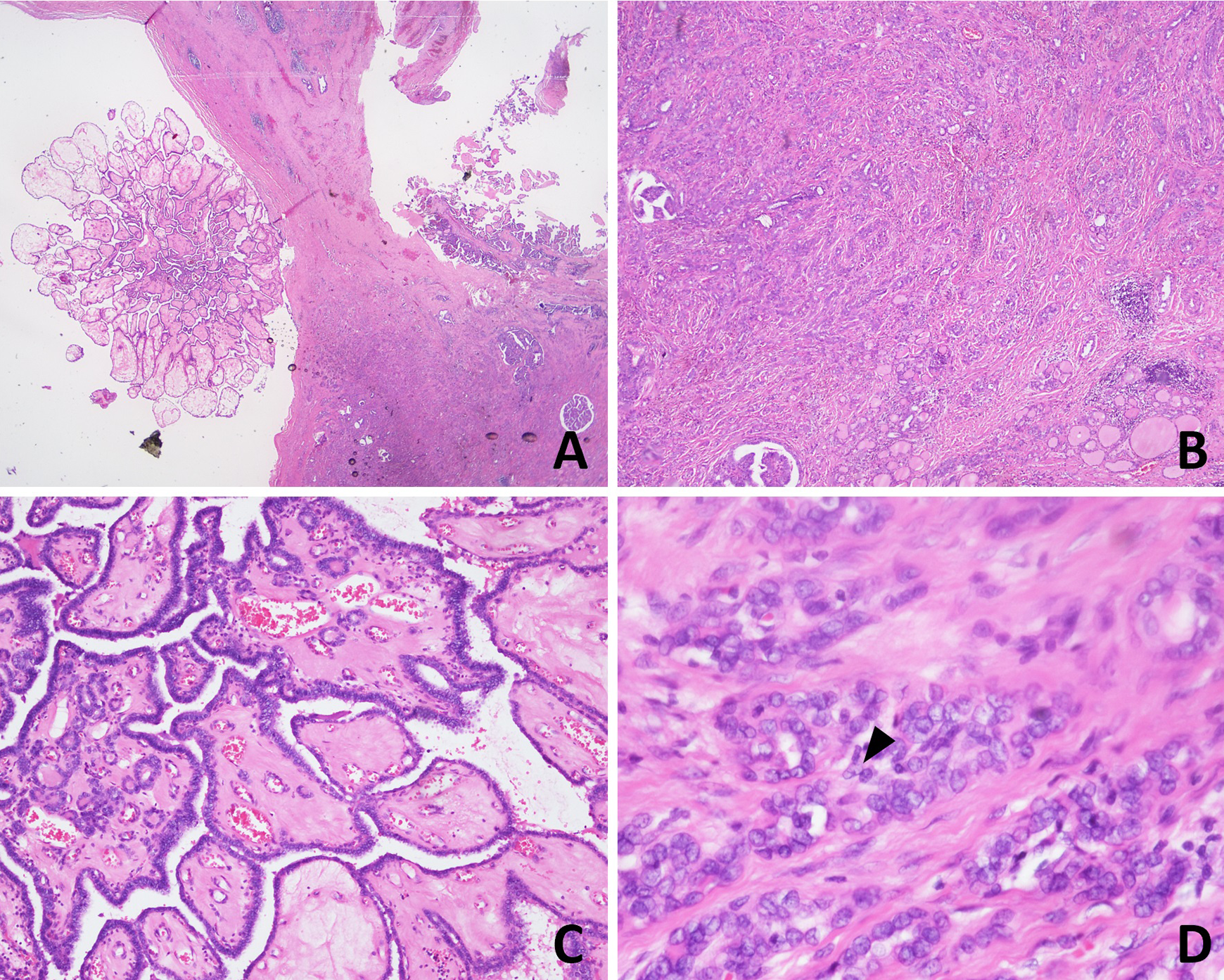
(A) Papillary thyroid carcinoma arising in the thyroglossal duct cyst. (B) Follicular pattern with normal thyroid tissue (hematoxylin and eosin [H&E] × 40). (C) Papillary architecture (H&E × 100). (D) Intranuclear pseudo-inclusion in the tumor cells (arrowhead) (H&E × 400).
Discussion
Thyroglossal duct cysts are the most common congenital lesions of the neck. It accounts for 70% of all congenital midline neck masses. 3 A thyroglossal duct cyst arises as a cystic expansion of the epithelial remnant of the thyroglossal tract and ectopic thyroid tissue could be examined histologically in up to 50% of the cyst 4 and located within the wall of the cyst and has the potential to develop malignancy.
Most thyroglossal duct cysts have an average size of 2 to 4 cm. 5 In up to 60% of the cases, the cysts were at or below the hyoid bone. Although the cyst is adjacent to the larynx, intralaryngeal extension of the cyst is relatively rare. Intralaryngeal extension may be due to long-standing enlargement of the cyst or malignant change. 3 Reviewing the literature, there were only 24 reported cases. 1 All the cases reported were benign. Statistically, most patients had neck mass at presentation and the most common symptoms reported were dysphonia, dysphagia, and dyspnea, which result from laryngeal obstruction. Thus, intralaryngeal extension should be considered when there is thyroglossal duct cyst associated with hoarseness, difficulty swallowing, and dyspnea.
Carcinoma occurs in less than 1% of thyroglossal duct cysts. Papillary type is the most common, comprising 94% of all. 2 It tends to present and diagnosed at a mean age of about 40 years. 6 Statistically, approximately 80% of thyroglossal duct cyst carcinomas are 2 to 5 cm in size, which is very similar to benign cysts. 7 Up to 95% of patients with thyroglossal duct cyst carcinoma presented with an asymptomatic neck mass. 6 Only 3.1% of patients had dysphagia. 6 None of the reported cases had such a huge lesion with intralaryngeal extension leading to airway compromise.
There are 2 theories to explain the etiology of thyroglossal duct cyst carcinomas. One is the hypothesis of de novo theory basing on the evidence of ectopic thyroid tissue within the cyst and absence of metastatic disease. 4,8,9 The other is the metastatic theory, which suggests that the lesion is metastatic from an occult primary thyroid gland. 10 In our case, calcification within the tumor is localized within the thyroglossal duct cyst that is revealed on the computed tomography scan and it did not extend beyond the cyst, which contains normal epithelial lining, and no malignancy is found in the main thyroid gland. We believe that the primary carcinoma in our case originated from the ectopic thyroid tissue within the thyroglossal duct cyst.
Due to the rarity of reported cases of thyroglossal duct carcinoma, there is no consensus regarding the surgical management. Sistrunk procedure is the mainstay of the treatment if there is no evidence of lymphadenopathy or thyroid malignancy. If the lesion concurred with thyroid malignancy or involves the cervical lymph nodes, total thyroidectomy, and neck dissection should also be considered. 11 With a 99.4% survival rate and low recurrence rate, the prognosis is very well. 6 Sistrunk operation alone with close follow-up is a proper treatment option for our case.
The clinical and imaging presentation of this reported case was extremely rare. Thus, a thyroglossal duct cyst carcinoma with intralaryngeal extension should be considered in the differential diagnosis when the case has a huge central neck mass with ectopic thyroid tissue and develops airway compromise concurrently. Surveillance of ectopic thyroid tissue and cervical lymph nodes are mandatory for unveiling occult malignancy. Complete excision with adequate adjuvant therapy according to tumor extent generally leads to not only symptom relief but also good prognosis.
Footnotes
Authors’ Note
This article does not contain any studies with human or animal subjects. Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.