
Abstract
We report a case with rare complication of cerebral venous thrombosis, as well as an incomplete response, after sigmoid sinus resurfacing surgery for pulsatile tinnitus (PT). A 24-year-old female patient with PT originating from the sigmoid sinus underwent sigmoid sinus resurfacing surgery. The tinnitus was immediately resolved, but it recurred with headache 5 days after surgery. A cerebral venous thrombosis was identified and treated, but PT persisted, although its frequency and loudness decreased. Sigmoid sinus resurfacing surgery is a safe and effective method to treat PT, but in some patients, it can cause serious complications and/or persistent tinnitus. In our patient, factors such as changes in blood viscosity due to warfarin intake or increased blood flow due to weight loss may have influenced the persistence of the tinnitus. It is important to identify the various associated factors and the weight of each of these factors to provide more tailored treatment of PT for individual patients in the future and to reduce complications and increase the effectiveness of sigmoid sinus resurfacing surgery.
Introduction
Pulsatile tinnitus (PT) is a phenomenon in which one perceives the sound of one’s vascular flow. 1 Pulsatile tinnitus is mainly caused by vascular wall abnormalities, including bony wall thinning/dehiscence, diverticulum, and aberrancy in the major vessels of the temporal bone. 2 The surest way to treat PT is elimination of the causative vessels by ligating or embolizing them. Although there have been reports of successful attempts, many have been associated with considerable morbidity, and these procedures are thus discouraged. 3 Meanwhile, resurfacing of the affected vascular wall has emerged as a new surgical treatment method, 4 -6 which restores the vascular wall abnormalities by applying autologous or artificial material, that is, creating a “sound baffle,” which eliminates turbulent flow caused by existing vascular wall abnormalities and reduces the transmission of vibration via the temporal bone. 7 Promising outcomes have been reported with >80% of resurfacing cases showing complete or partial resolution of PT. 7 In contrast, nonresponders or worsening cases have also been reported and although they are very rare, some complications requiring immediate treatment have occurred
We experienced a case of PT, in which cerebral venous thrombosis (CVT) developed after sigmoid sinus (SS) resurfacing surgery, and PT remained even after the CVT was treated. Here, we introduce this case with a literature review of this rare complication, including a discussion of cases unresponsive to resurfacing surgery.
Case Report
A 24-year-old woman presented with a 1-month history of PT in her right ear. The sound was coincident with her heartbeat, and the intensity was increased when lying down and decreased with compression of the ipsilateral neck. Subjective severity of the tinnitus was assessed using a Korean version of the Tinnitus Handicap Inventory (THI) score, and results were consistent with a severe degree of PT with a score of 66. She had been taking Prozac since 2016 due to major depression disorder. Her body mass index was 36.3, and she was not taking birth control or hormonal replacement medication. On physical examination, the right tympanic membrane was normal. Pure tone audiometry revealed a mild, low-frequency air-bone gap on the right side. Temporal bone computed tomography demonstrated the dominant SS with thin overlying bone on the right side (Figure 1A). Since the symptoms had lasted for only 1 month, the patient was advised to wait for several months to ascertain if the symptoms would subside naturally; however, the patient demanded surgical treatment because of her incapacitating symptoms. The patient decided to undergo SS resurfacing surgery. A simple mastoidectomy was performed and the prominent SS was exposed, showing a remarkably thin cortical bone (Figure 1B). A piece of conchal cartilage and deep temporalis muscle fascia was harvested and inserted under the cortical bony bridge (Figure 1C), and bone cement was applied (Figure 1D).
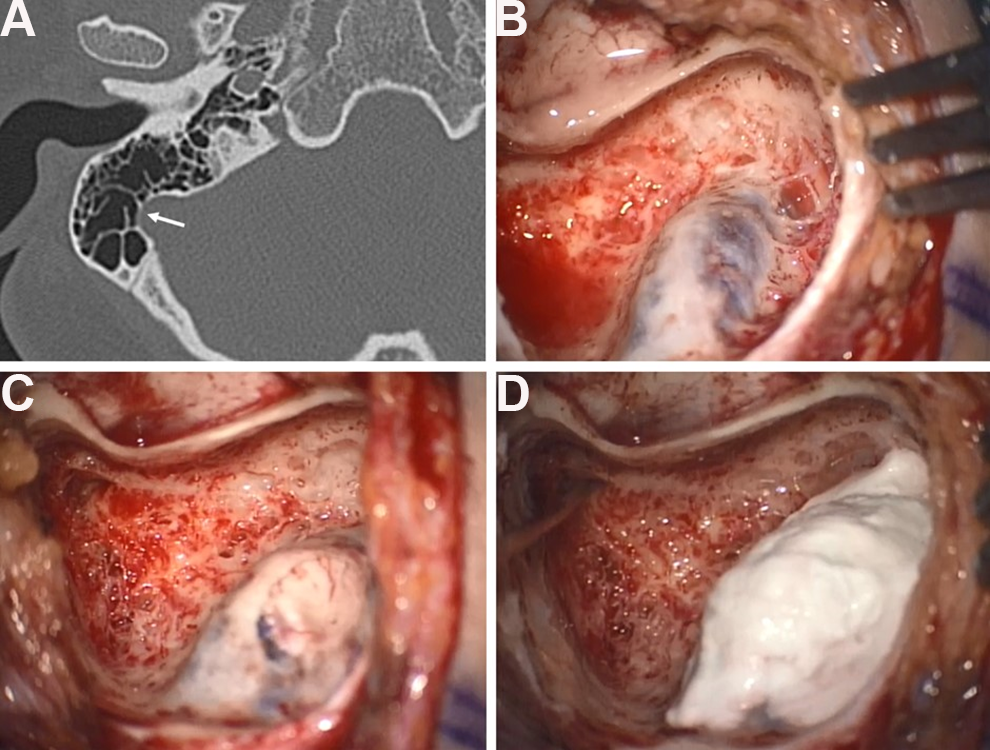
Temporal bone computed tomography demonstrates the dominant sigmoid sinus (SS) with thin overlying bone on the right side (A, arrow). Prominent SS and thin overlying bone are exposed after simple mastoidectomy (B). Conchal cartilage is inserted under the cortical bony bridge (C). Bone cement is applied (D).
The tinnitus disappeared immediately after surgery; however, 5 days later, the patient complained of a severe headache and the return of PT, and she had a spiking fever. At first, increased intracranial pressure (IICP) due to mechanical SS compression with central nervous system infection was suspected. Bilateral papilledema was noted, and lumbar puncture was performed to measure intracranial pressure (ICP) and to obtain cerebrospinal fluid (CSF). Intracranial pressure was mildly increased to 24 mmH2O, and no microorganism was detected from the CSF. However, the symptoms were resolved right after CSF drainage. Temporal bone computed tomography revealed a hyperattenuated lesion in the right SS on noncontrast imaging (Figure 2A) and a distended right transverse sinus on contrast-enhanced imaging (Figure 2B). Contrast-enhanced T1-weighted MR imaging and magnetic resonance venography (MRV) revealed a focal filling defect in the right SS, and CVT was suspected (Figure 2C and D). The laboratory study revealed increased
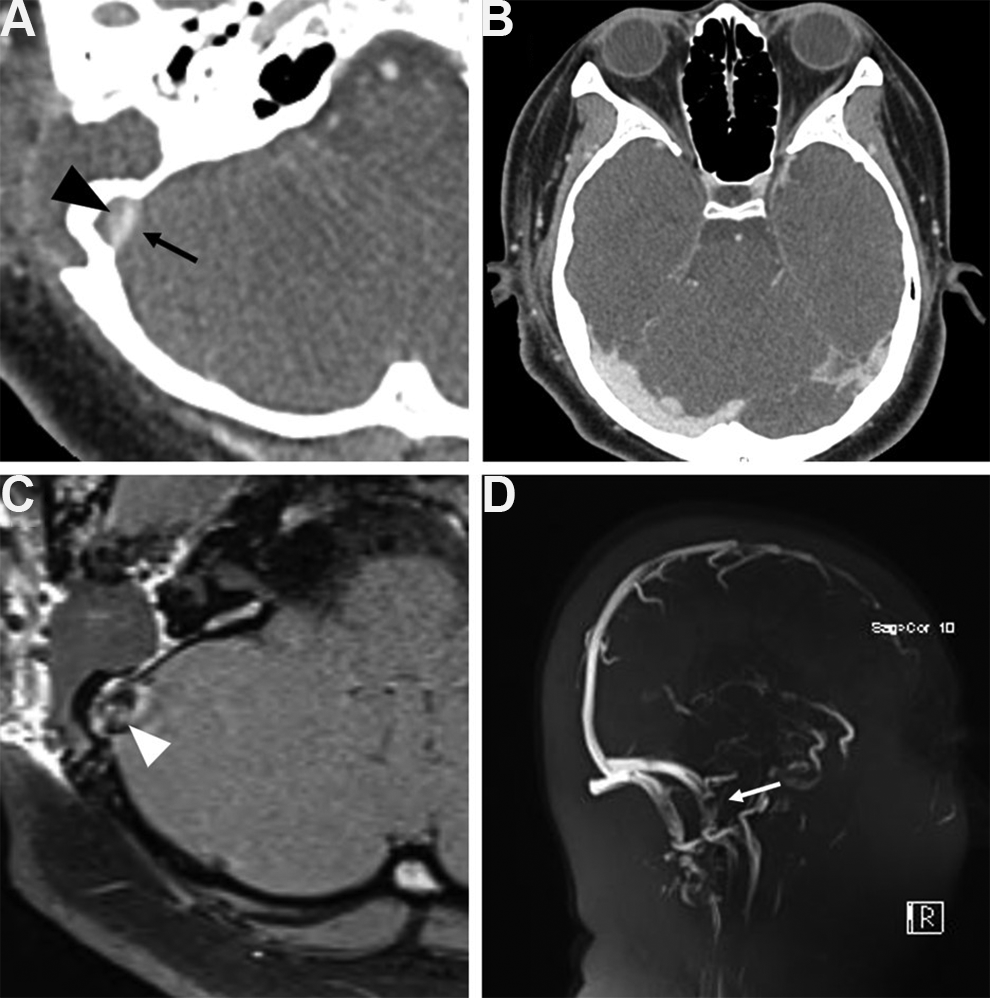
Noncontrast temporal bone computed tomography (TBCT) reveals a hyperattenuated lesion in the right sigmoid sinus (SS), a cerebral venous thrombosis (CVT, black arrow) is suspected, while the graft material appears as hypoattenuated (black arrowhead) (A). Distended right transverse sinus is noted on contrast-enhanced TBCT (B). Contrast-enhanced T1-weighted magnetic resonance imaging (white arrowhead) (C). Magnetic resonance venography (white arrow) (D) reveals a focal filling defect in the right SS, and CVT is suspected.
An additional laboratory test was performed to investigate the causes of the development of CVT, such as autoimmune disease or high blood viscosity–related disease. The patient showed increased platelet counts up to 500 K; however, the increased platelet counts were probably due to iron deficiency anemia reactive thrombocytosis. A laboratory test to detect vasculitis was performed, and several associated antibodies, such as anticardiolipin antibody and antinuclear antibody, were detected. The rheumatologists suggested the possibility of preoperatively unrecognized antiphospholipid syndrome or systemic lupus erythematosus (SLE). Considering her underlying systemic inflammatory disease, long-term anticoagulation therapy was administered with 6-month warfarin (5 mg daily) therapy. Follow-up MRV imaging was performed 7 months following surgery, and thrombosis was not detected.
Discussion
We presented a rare case of CVT, which is the most worrisome complication of SS resurfacing surgery, which inevitably yields direct SS compression and subclinical vascular injury. This provides a favorable condition for CVT to occur since compression brings venous flow reduction and stasis, and damaged endothelium triggers the activation of platelets and coagulation. 8 However, CVT caused by SS manipulation alone is extremely rare. Cerebral venous thrombosis is typically multifactorial, and various causes and associated risk factors for CVT have been identified. Pregnancy, puerperium, and birth control medication or excess estrogen use can contribute to prothrombotic condition. Ear infections, systemic inflammatory disease, hematologic conditions, direct mechanical stimulation, and trauma can facilitate the development of CVT. 9 Our patient had multiple risk factors including obesity, 10 thrombocythemia, possible antiphospholipid syndrome or SLE, and SS resurfacing surgery. Identifying all risk factors before surgery is difficult, and even if all risk factors are identified in advance, predicting whether CVT will occur after surgery is still difficult. For this reason, in some groups of patients, prophylactic anticoagulation medication is administered to prevent CVT associated with SS resurfacing surgery. 11 However, its benefits and risks have not yet been studied.
A recent systematic review reported CVT after resurfacing surgery in 2 of 140 cases,
7
and these 2 patients presented with headache and blurred vision. These are relatively nonspecific symptoms for IICP as they also occur in the absence of thrombosis simply due to compression of the sinus by surgical materials. Differentiating CVT from simple compression is crucial because these two conditions pose completely different mortality risks and require different treatments. Prompt anticoagulation administration is mandatory in cases of CVT since the untreated thrombosis can progress to neurologic deficits and/or death, whereas extraluminal compression requires close observation, but is usually self-limiting. Imaging and laboratory studies could help to distinguish between them. On noncontrast CT, an acute thrombus is hyperattenuated, whereas the soft tissue material compressing the vessel appears as hypoattenuated.
11
Here, graft materials and thrombus were easily distinguishable (Figure 2A). A magnetic resonance imaging (MRI) is more sensitive for the detection of CVT than CT in general.
12
On MRI, an acute thrombus is hypointense, unlike graft materials.
11
A systematic review reported 121 cases of SS resurfacing and included 91 (75%) cases with complete resolution, 12 (10%) with partial resolution, 17 (14%) with no resolution, and 1 (1%) with worsened PT. 7 Many hypotheses have been suggested to explain the different results after the same treatment, and Eisenman proposed a multifactorial theory, which hypothesized that various factors are in balance and PT begins to occur when this balance collapses. 13 According to the theory, the existence of transverse SS and its degree and length, size of dehiscence, flow characteristics of blood flow, outflow resistance, and central venous pressure are possible factors, and the weight of each factor in the balance differs from patient to patient. Here, PT was completely lost at first, indicating that SS resurfacing itself was successful in creating the sound baffle. Thereafter, PT occurred again as CVT developed. The presence of CVT narrows the SS, resulting in a change in blood flow velocity and pressure, which is thought to have contributed to the recurrence of PT. However, PT persisted even after CVT was treated. It can be assumed that PT recurred due to the occurrence of another factor that was more influential than the sound baffle, such as changes in blood viscosity due to warfarin intake, or increased blood flow due to some weight loss. In the present case, various factors were associated with different degrees of influence on the development of PT; thus, we believe that identification of the various associated factors and the weight of each of these factors could provide more tailored treatment of PT for individual patients in the future.
Sigmoid sinus resurfacing surgery is an effective and safe method for treating PT. However, procedures that do not take into account individual diversity may be ineffective and dangerous. We hope that this case report provides an improved understanding of the pathophysiology of PT and provides practical advice for more effective and safe treatment of PT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2019R1C1C1006341) to J.M.L.