
Abstract
Metastatic carcinoma of the external auditory canal (EAC) is extremely rare. Herein, we report the first case of a patient with metastasis of parotid adenocarcinoma to the EAC. Clinicians should include it in the differential diagnosis of tumors of the EAC. In patients with parotid carcinoma, a physical examination of the entire head and neck, including the EAC, should be performed before surgery.
Introduction
Metastatic carcinoma of the external auditory canal (EAC) is extremely rare.1-4 To the best of our knowledge, there are no previous reports of metastasis of parotid carcinoma to the EAC. Herein, we report the first case of a patient with metastasis of parotid adenocarcinoma to the EAC.
Case report
A 56-year-old male patient was first diagnosed with left parotid adenocarcinoma 10 years ago and had undergone several surgeries, radiation therapy, and chemotherapy until 2 years ago. The patient had no recurrence or metastasis on imaging and physical examinations after the end of the last session of chemotherapy 2 years ago. However, 1 year ago, a borderline lymph node was found at the left neck level II and the size of the lymph node had increased over several months, and recurrent lesions were also found at the parotid gland surgery site. In the preoperative examination, recurrent left parotid adenocarcinoma (T4aN2bM0) was diagnosed, and radical parotidectomy with wide skin excision and neck dissection were planned (Figure 1). Multiple recurrent lesions are observed around the site of previous surgery for parotid carcinoma, and no lesions were found in the external ear.
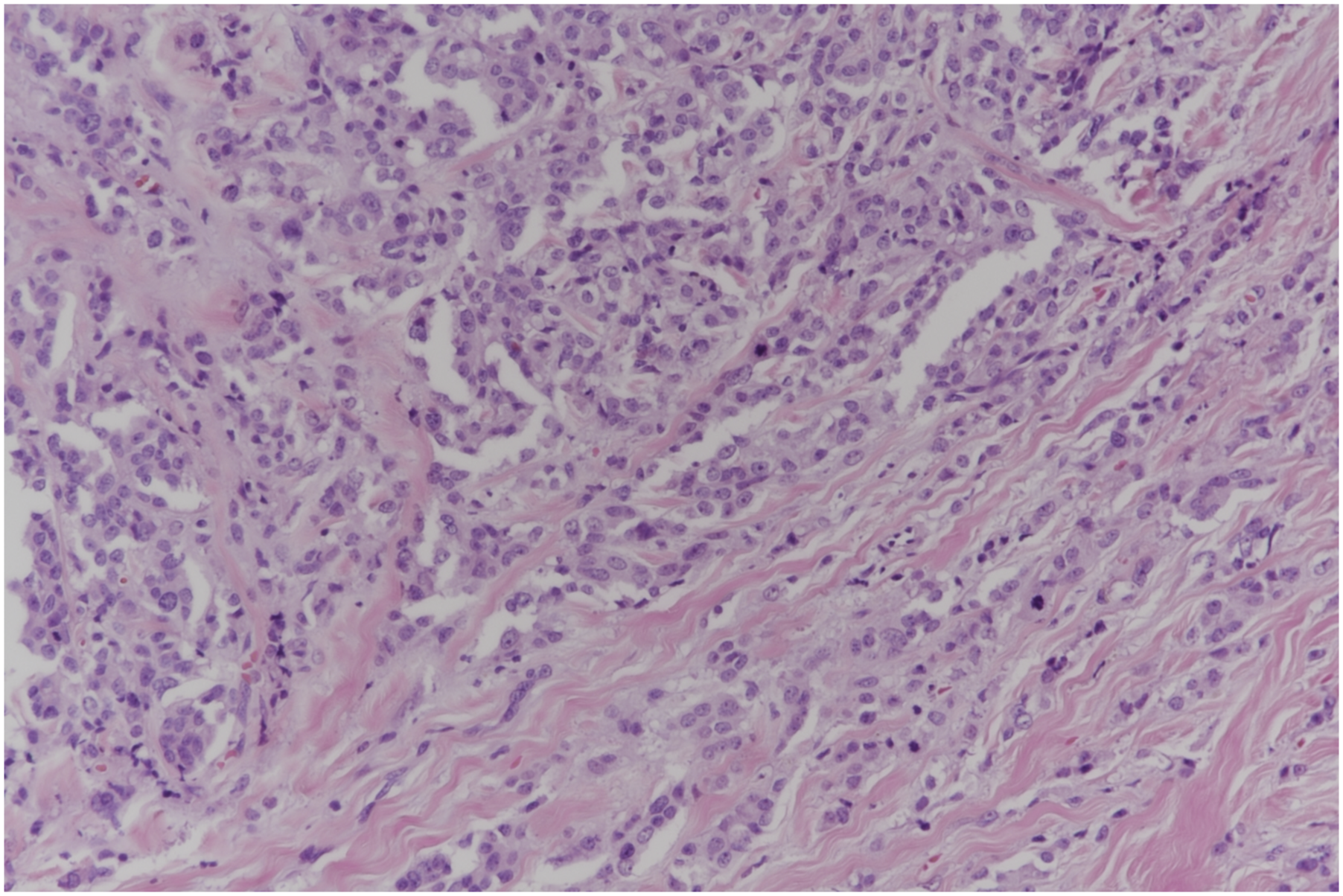
During the preoperative head and neck examination, a mass in the left EAC was discovered incidentally just in front of the tympanic membrane (Figure 2). This mass had not been observed before, and the patient did not have any otologic symptoms, such as otorrhea, hearing loss, or otalgia. The mass was about 0.5 cm in size, well circumscribed, and attached to the posterior wall of the left EAC. During the operation for parotid carcinoma, the mass in the EAC was also completely removed endoscopically. Histological examination of the EAC mass confirmed that it was an adenocarcinoma that had metastasized from the parotid gland (Figure 3). All other EAC tissues, temporal or mastoid regions were normal; thus, it was judged as isolated metastasis of left parotid adenocarcinoma. The patient will be treated with postoperative chemoradiotherapy without any further surgery. In the endoscopic photograph, a 0.5-cm sized mass in the left external auditory canal is discovered incidentally just in front of the tympanic membrane. Tumor shows infiltrative, solid, cord-like and ductal growth patterns. Tumor cells show pleomorphic nuclei, prominent nucleoli, and frequent mitotic figures (H & E stain, x200).
Discussion
Carcinomas of the EAC are mainly primary carcinomas, and metastatic carcinoma is very rare.1-4 Common carcinomas that mainly metastasize to the EAC are breast, renal, and lung carcinoma.2-4 Metastasis of parotid carcinoma to the EAC has not yet been reported.
Metastasis to the EAC occurs via vascular and perineural pathways or combined methods. 2 The histopathologic biopsy result of this patient showed both vascular and perineural invasion; thus, it was not known by which of the two methods did metastasis occur. Because parotid carcinoma is close to the EAC, it can be directly extended through the fissures of Santorini. 5 However, in this patient, invasion into the EAC and temporal regions was not observed on imaging examinations or surgical findings.
Metastatic carcinoma of the EAC usually presents with symptoms, such as an externally visible mass, hearing loss, bloody otorrhea, and otitis externa.1-4 However, if the tumor is small and located deep in the EAC, as in our patient, it may be asymptomatic.
Metastatic carcinoma of the EAC can be easily detected by physical examination, but imaging and biopsy are required to differentiate diagnosis for exostosis, malignant otitis externa, cholesteatoma, aural polyp, and other neoplasms of the EAC.1-5
Although the treatment of metastatic carcinoma of the EAC varies depending on the primary site, chemotherapy is prioritized because it is almost always caused by distant metastasis.1-4 In this patient, since metastatic carcinoma of the EAC was small, complete endoscopic resection was performed simultaneously with parotid surgery. However, parotid adenocarcinoma is an aggressive, high-grade cancer with frequent regional metastasis and low survival. 6 Because this patient is in an advanced stage with EAC and neck metastases, additional chemoradiotherapy is being administered after surgery. 5
Conclusion
Although metastatic carcinoma of the EAC is extremely rare, clinicians should include it in the differential diagnosis of tumors of the EAC. In patients with parotid carcinoma, a physical examination of the entire head and neck, including the EAC, should be performed before surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.