
Abstract
Inflammatory myofibroblastic tumor (IMT) is a very rare mesenchymal tumor that can behave as a locally benign or aggressive lesion. Here, we present an extremely rare case of IMT involving the subglottic of a middle-aged male. Steroid therapy treatment alleviated dyspnea, but the recurrence of dyspnea was reported two months later. Both sides of the subglottic tumor were excised following treatment, and the surgical specimens were subjected to histopathological evaluation and diagnosis for IMT. At 4 years after excision, follow-up laryngoscopy revealed symmetric vocal cords without evidence of any subglottic mass. Subglottic mass is often asymptomatic until it presents with hoarseness or dyspnea, and subglottic IMT is rare. Based on the successful treatment of our case, complete surgical excision is highly recommended for this rare tumor. However, further research is needed to discover a more effective and cost-effective treatment approach.
Introduction
Inflammatory myofibroblastic tumor (IMT) is a very rare mesenchymal tumor, consisting of a myofibroblastic spindle cell stroma with accumulation of leukocytes and plasma cells, and/or eosinophils. It behaves as a locally benign or aggressive lesion, clinically and radiologically mimicking a neoplastic process. However, only a few cases of subglottic IMT have been reported. Here, we describe a case of primary IMT of the subglottis.
Case Report
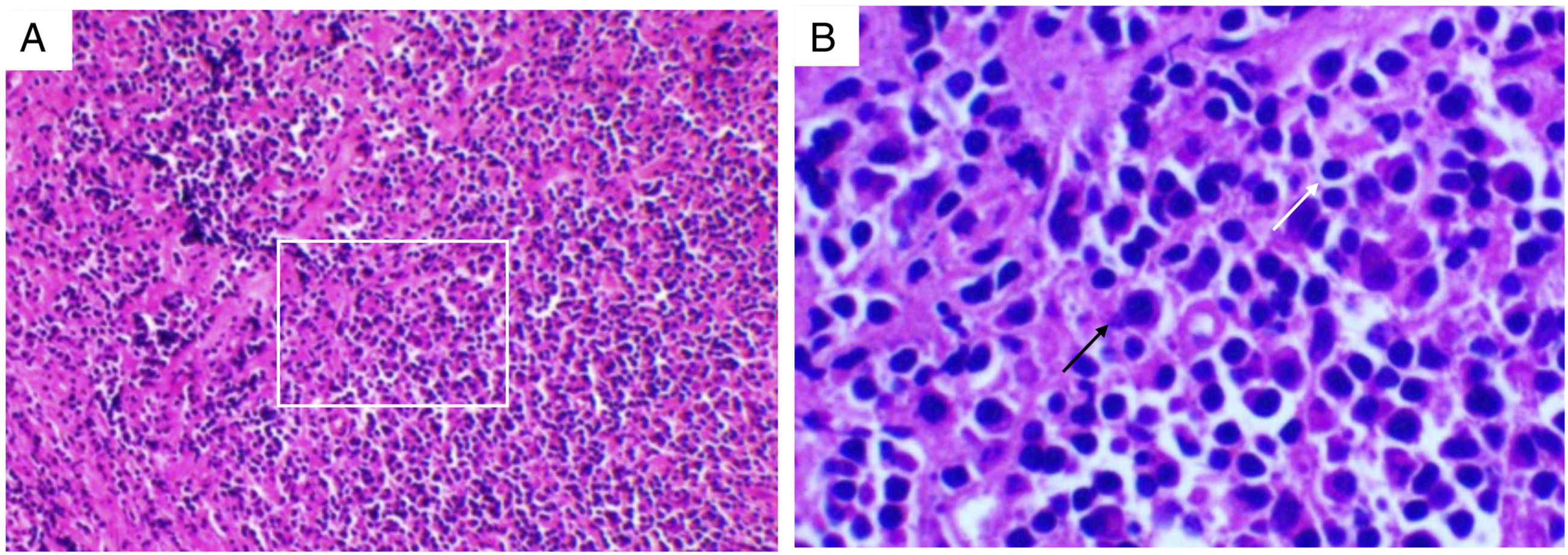
A 39-year-old man was suffered from dyspnea accompanied with hoarseness in the morning for 2 months. Fiberoptic bronchoscopy showed that subglottic stenosis occurred due to symmetrical lumps. The patient was then admitted to the Department of Otolaryngology Head and Neck Surgery. Magnetic resonance imaging (MRI) revealed an inflammation mass in the subglottic area. After 2 weeks of glucocorticoid treatment, the dyspnea was relieved, and the patient was discharged without medication. However, the patient had recurrence of dyspnea two months later. Electronic laryngoscope examination also showed the narrowing of the subglottis. Then, we resected the subglottic tumor by laryngofissure. Hematoxylin-eosin staining and immunohistochemistry were carried out, and the results confirmed that the subglottic tumor was IMT. After 4 years of follow-up, the patient was asymptomatic (Figure 1A and B). Magnetic resonance imaging of the neck revealed low signal intensity on T1-weighted images and medium signal intensity on T2-weighted images. These results demonstrated medium enhancement after contrast infusion. There was a bulging of the subglottic space in the vocal fold, but there was no true extension (Figure 1C and D). Biopsies of the mass showed a fibroblastic proliferation admixed with lymphocytes and plasma cells. There was no evidence of a definite malignancy. As shown in Figure 2, immunochemistry stains were positive for CD138, CD31, CD34, and CD38, while positive/negative for smooth muscle actin. (A-B) Endoscopic examination of the larynx before and after treatment. (A) shows the subglottic tumor under fiberoptic bronchoscopy. (B) indicates that the tumor is completely excised after surgery under laryngoscopy (white arrow represents the subglottic tumor). (CE) Magnetic resonance imaging (MRI) of the subglottis. (C) is the T1-weighted image, (D) is the contrast infusion image, and (E) is the T2-weighted images (white arrow indicates the subglottic tumor). Hematoxylin-eosin staining of the subglottic tumor. A (×100) and B (×400). Subglottic tumor contains large amounts of lymphocytes and plasma cells (white rectangle shows the part in figure B, white arrow represents the lymphocytes, and black arrow indicates the plasma cells).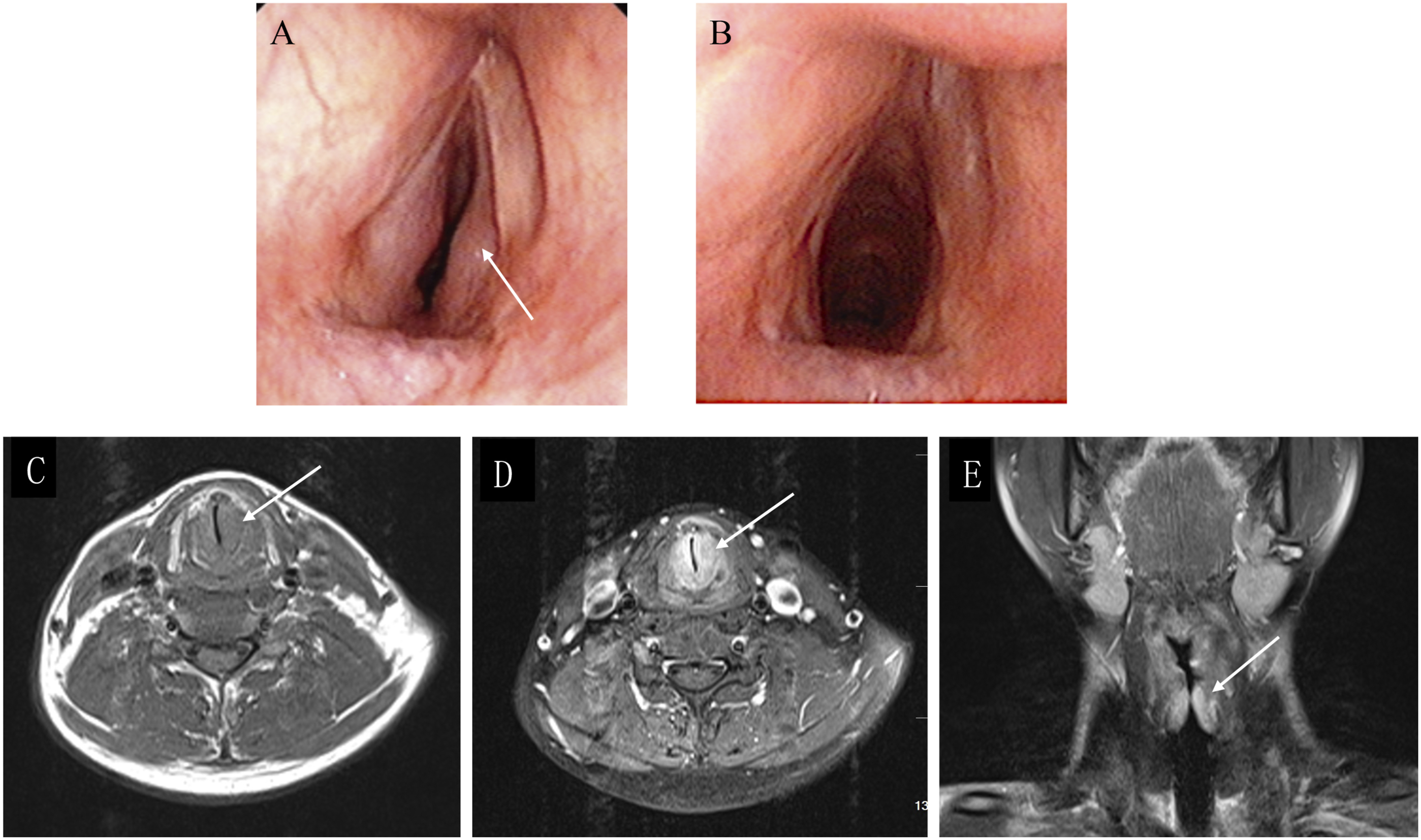
Discussion
Inflammatory myofibroblastic tumor is a rare benign tumor caused by an inflammatory condition. The time-honored term “inflammatory pseudotumor” and the alternative expression “plasma cell granuloma” comprise a wide range of neoplastic and non-neoplastic (reactive) lesions. Inflammatory myofibroblastic tumor has been commonly seen in the lungs, but is rare in the subglottis. 1 Its exact incidence and etiology are still unknown. The lesion’s pathogenesis, biological behavior, and appropriate treatments remain controversial, and little is known about its prognosis. Inflammatory myofibroblastic tumor involves a variety of organs and tissues in the body, and can occur at any age in both sexes.2-4 The etiology of IMT remains unclear, which may involve an immunologic response to stimuli such as tissue damage, smoking, foreign bodies, stem cell transplant, inflammatory reaction to trauma, autoimmune reaction, or infection. Epstein–Barr viruspositive infection has been reported as a possible predisposing factor for IMT.5-8
It is difficult to diagnose IMT by physical examination, MRI, computed tomography (CT), and laryngoscopy. The imaging features of IMT lack specificity, and it cannot be distinguished from inflammation by CT or MRI. The clinical behavior of IMT is relatively similar to that of neoplasm. Therefore, it must be differentiated from a variety of benign and malignant soft tissue tumors such as chronic fungal infection, Wegener’s granulomatosis lymphomas, fibrosarcomas, and metastases.9-11 All these lesions located in the subglottic region can present with dyspnea, hoarseness, and other non-specific symptoms. Despite advances in imaging technologies, distinguishing between IMT and other larynx masses continues to be a major challenge. A spectral CT imaging study reported that patients with IMT had significantly higher normalized iodine concentration in the arterial phase and venous phase (NICVP), slope of spectral Hounsfield unit curve in the arterial phase (λAP) and venous phase (λVP), and normalized iodine concentration difference between arterial and venous phases (ICD) than those with lung cancer. 12 It may be helpful for diagnosis. If the clinical presentation and imaging studies reveal a suspicious appearance, it is often diagnosed as a malignant tumor.13,14 Radiological results can help surgeons plan a surgical approach. In our case, the tumor presented as a single mass with a non-specific radiologic appearance; thus, a definitive diagnosis can be made depending on biopsies.
The management of subglottic IMT remains a topic of controversy. To our knowledge, the medical treatment for subglottic IMT has not yet been standardized. The natural clinical course is spontaneous regression without intervention.15,16 However, if the lesion causes significant discomfort, therapeutic interventions are necessary. Management options include conservative or surgical approach. The mainstay of treatment for laryngeal IMT is complete surgical excision.4,17 In head and neck, the tumor can be completely excised by endoscopic surgery, 4 and sometimes with carbon dioxide laser 17 or potassium-titanyl-phosphate laser. 18 Conservative management includes nonsteroidal anti-inflammatory agents or steroids.2,19,20 For patients with unresectable masses, corticosteroid treatment and radiotherapy may be useful.19,21 However, patients treated with conservative or surgical approach can experience a recurrence of the disease. It has been reported that the malignant transformation of IMT and recurrent distant metastasis may occur a few years following surgical resection. 2
Inflammatory myofibroblastic tumor is not a common lesion in the subglottis and often lacks specific symptoms and radiological performance. The main treatments of this disease include surgical excision, steroids, and others. Based on the successful treatment of our case, complete surgical excision is highly recommended for this rare tumor. Considering that it can mimic malignant tumor, a close follow-up is necessary after treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Ethical Approval
The study was approved by the ethics committee of Zhongnan Hospital of Wuhan University, Wuhan, China.
Informed Consent
Written informed consent was obtained from the patient.