
Abstract
Objectives
Eosinophilic chronic rhinosinusitis (ECRS) is an allergic inflammatory disease characterized by chronic inflammation of the sinus mucosa, and sometimes, osteitis. This study aimed to investigate the pattern of osteitis in ECRS and the relationship between bony thickening of the middle turbinate and recurrence of ECRS.
Methods
A total of 246 patients with paranasal diseases were included in the study. The patients’ data on bone thickening level, mucosal thickening, polyp score, clinical severity, and laboratory data were retrospectively evaluated.
Results
In total, 38, 186, and 22 patients had ECRS, non-ECRS (NECRS), and odontogenic sinusitis, respectively. The Lund–Mackey (LM) score and Global Osteitis Scoring Scale (GOSS) scores in patients with ECRS were higher than those in patients with other paranasal diseases. There was a significant positive correlation between the GOSS score and ECRS clinical disease severity. Postoperative recurrence was significantly increased in patients with ECRS associated with bony thickening of the middle turbinate.
Conclusion
Both mucosal inflammation and osteitis were more severe in patients with ECRS than in patients with other diseases, and clinical disease severity was correlated with osteitis. Furthermore, the postoperative recurrence rate tended to increase in patients with ECRS who had bony thickening of the middle turbinate.
Introduction
Chronic sinusitis is a disease that causes chronic inflammation of the sinus mucosa, and multiple subclasses have been reported. It is clinically classified as chronic rhinosinusitis with nasal polyps (CRSwNP) and chronic rhinosinusitis without nasal polyps (CRSsNP). Chronic rhinosinusitis with nasal polyp is a heterogeneous phenotype in East Asia. Accordingly, CRSwNP is further classified into eosinophilic chronic rhinosinusitis (ECRS) and non-eosinophilic chronic rhinosinusitis (NECRS), according to the type of cells infiltrating the sinus tissue. 1
Eosinophilic chronic rhinosinusitis is a type 2 inflammation–based disease characterized by refractory nasal polyps with eosinophilic infiltration, and various cells and molecules are involved in the pathogenesis.2,3 Endoscopic sinus surgery is the basic treatment; however, early postoperative recurrence is often observed. Various factors related to recurrence have been reported, and it has been recently reported that the middle turbinate plays an important role. 4 There are various reports on the resection of the middle nasal turbinate during ECRS surgery.5-7 The advantages of resection have been reported in terms of improved drug delivery and improved postoperative endoscopic scores. In contrast, the disadvantages of the resection of the middle turbinate include an increased risk of reoperation due to loss of landmarks and olfactory disturbance. 8 With the advancement of assistive devices and subsequent research, no definitive conclusion has been reached regarding the resection of the middle turbinate.
Eosinophilic chronic rhinosinusitis can extend beyond the sinus mucosa and cause marked bony thickening. The Global Osteitis Scoring Scale (GOSS) score is a method of assessing bone thickening in the sinus cavity using sinus CT and was developed by otolaryngologists and radiologists. It is a method for evaluating the anterior ethmoid, posterior ethmoid, maxillary, frontal, and sphenoid sinuses on a 5-point scale left and right each side, and shows low inter-rater assessment variability. 9 The severity of bone thickening of each paranasal sinus as assessed by the GOSS score is known to correlate well with mucosal inflammation of the sinuses. Therefore, osteitis of paranasal sinus is thought to be involved in the recurrence of ECRS, meanwhile bone thickening in areas other than the paranasal sinuses has not been sufficiently investigated. This study aimed to investigate the pattern of osteitis in ECRS and the relationship between bony thickening of the middle turbinate and recurrence of ECRS.
Patients and Methods
Patient’s Profile
Patients who underwent nasal and paranasal computed tomography (CT) in our hospital between April 2014 and June 2021 were included in the study. Patients with mycetoma, paranasal tumors, or a paranasal cyst, or patients receiving continuous systematic glucocorticoid treatment, were excluded from this study. Patients with ECRS were diagnosed according to the Japanese Epidemiological Survey of Refractory Eosinophilic Chronic Rhinosinusitis (JESREC) criteria. 1 Patients with malignant tumors were excluded from this study. This study was approved by the ethics committee of our institution (No. 21061). Informed consent was obtained from the patients through an opt-out system via the hospital website. Patients who opted out were excluded from the study.
Computed Tomography Protocol
The computed tomography dose index (CTDI) used in this study was 17 mGy, with minor adjustments for body size and other factors, a .6-mm slice thickness. The bone window was used to calculate the GOSS score and bony thickening of middle turbinate.
Evaluation of Clinical Findings in Paranasal Sinus Diseases
The nasal polyp score in each patient was evaluated using nasal endoscopy. Nasal polyp scores were graded into 5 stages as described by Meltzer et al. 10 The Lund–Mackey (LM) score was used to assess mucosal inflammation in each sinus. The level of bone thickening in the sinus cavity was assessed using the GOSS score. 9
Measuring Bone Thickening of the Middle Turbinate
The boundaries of the middle turbinate and conchal bone were traced on the CT scan by modifying the method adopted by Demir et al.
11
The area of the bony thickening of the middle turbinate enclosed by the tracing line was measured directly using Synapse Vincent software (Fujifilm, Tokyo, Japan). Images of typical bony thickening of the middle turbinate for ECRS are shown in Figure 1. Images of typical bony thickening of the middle turbinate for ECRS.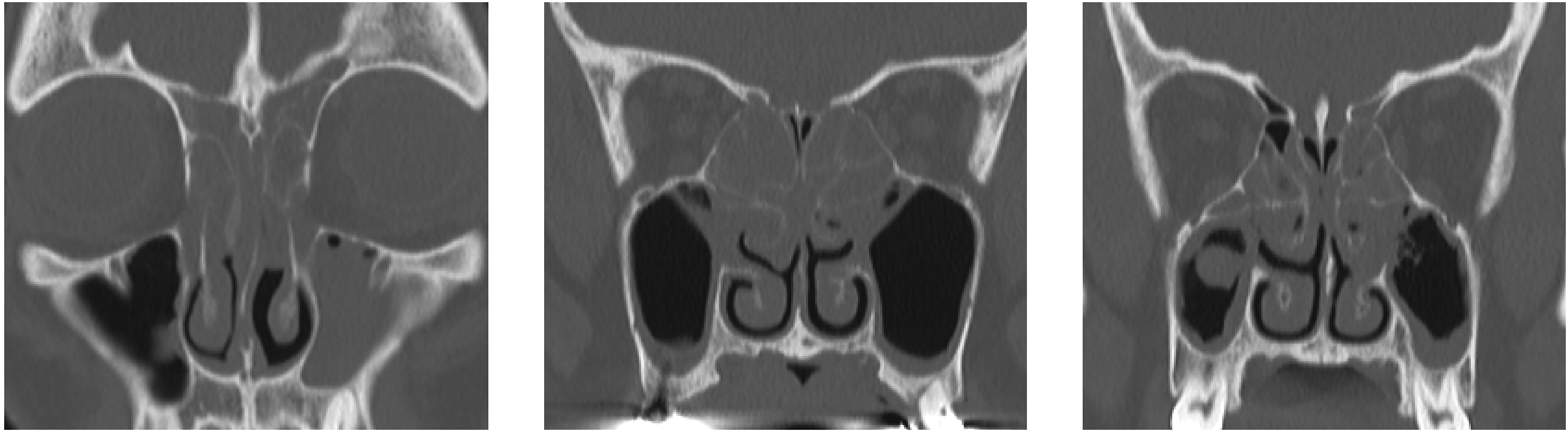
Statistical Analyses
All statistical analyses were performed using the Prism version 7. Data are expressed as mean ± standard deviation. Comparisons between 2 groups were performed using the nonparametric Mann–Whitney U test. The Kruskal–Wallis test was used to compare multiple groups. Correlations were expressed as Spearman’s rank correlation coefficients. Analysis of variance was used to evaluate differences between the 2 groups. Statistical significance was set at P < .05.
Results
Disease-specific GOSS
Clinical Data and Demographic Data of Patients.
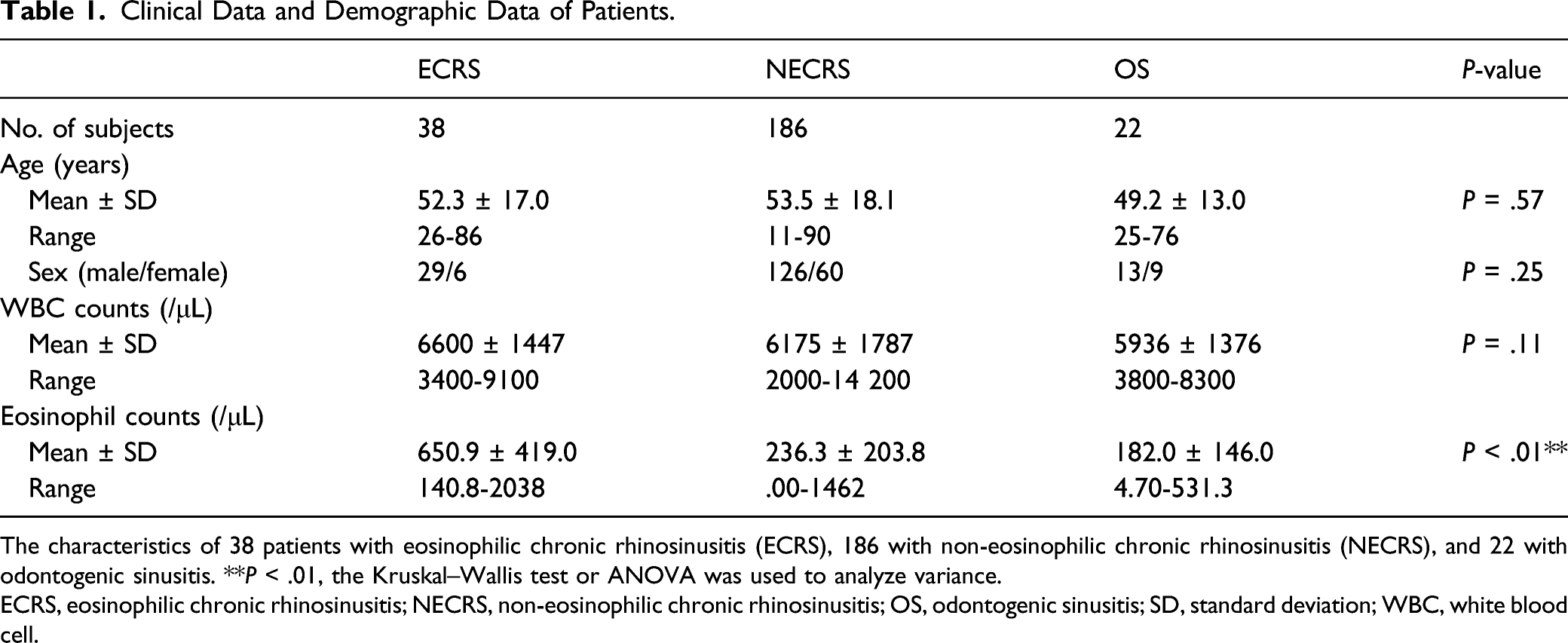
The characteristics of 38 patients with eosinophilic chronic rhinosinusitis (ECRS), 186 with non-eosinophilic chronic rhinosinusitis (NECRS), and 22 with odontogenic sinusitis. **P < .01, the Kruskal–Wallis test or ANOVA was used to analyze variance.
ECRS, eosinophilic chronic rhinosinusitis; NECRS, non-eosinophilic chronic rhinosinusitis; OS, odontogenic sinusitis; SD, standard deviation; WBC, white blood cell.
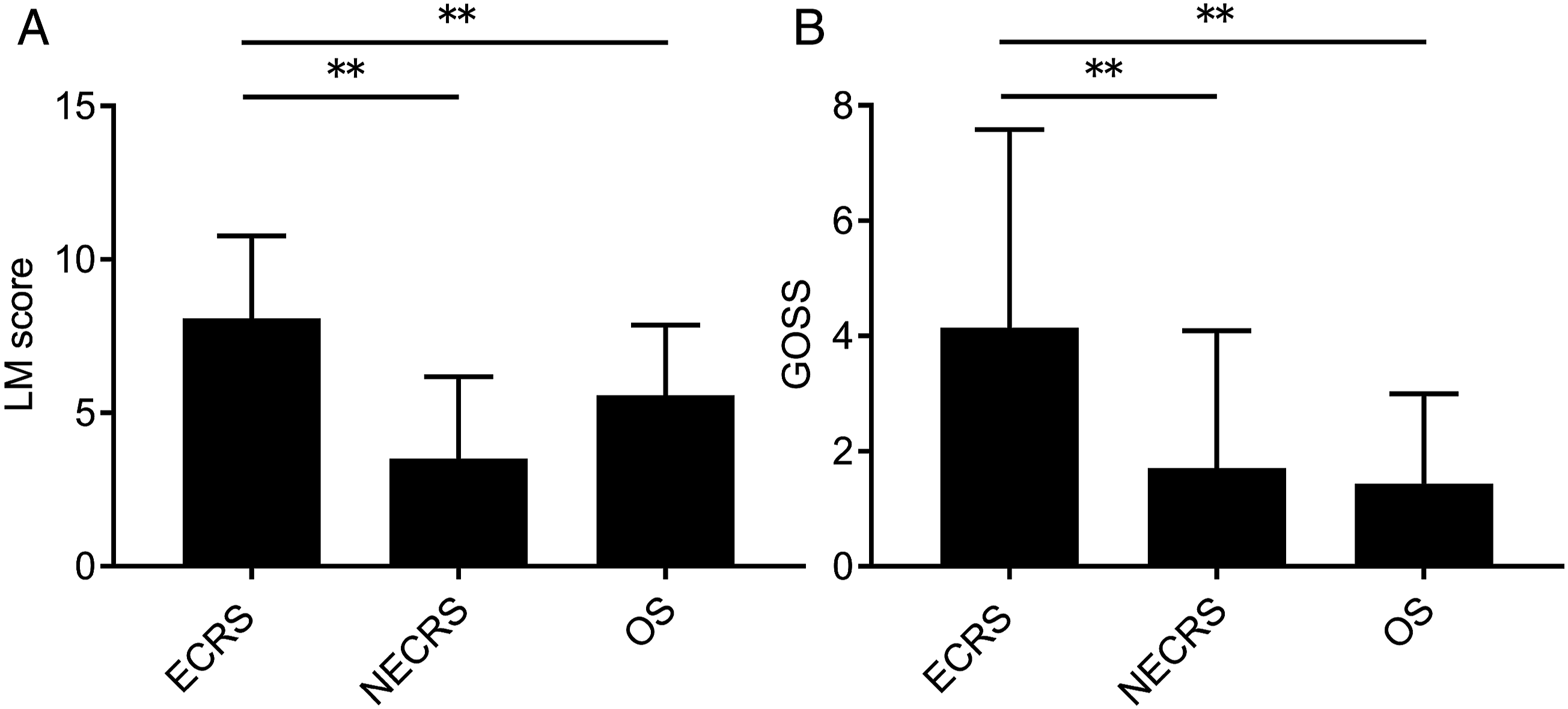
The Lund–Mackey score and Global Osteitis Scoring Scale score of patients with paranasal disease. (A) The Lund–Mackey score of 38 patients with eosinophilic chronic rhinosinusitis (ECRS), 186 with non-eosinophilic chronic rhinosinusitis (NECRS) and 22 with odontogenic sinusitis. (B) The Global Osteitis Scoring Scale score of 38 patients with eosinophilic chronic rhinosinusitis (ECRS), 186 with non-eosinophilic chronic rhinosinusitis (NECRS) and 22 with odontogenic sinusitis. Unilateral sinus disease was assessed only on the side with paranasal computed tomography (CT) shadowing, while bilateral sinus disease was assessed on both sides as 2 sides. *P < .05, **P < .01, NS: Not significant, as determined by the Kruskal–Wallis test, followed by the Mann–Whitney U test. Values are presented as mean ± standard deviation. LM score, Lund–Mackey score; GOSS, global osteitis scoring scale; ECRS, eosinophilic chronic rhinosinusitis; NECRS, non-eosinophilic chronic rhinosinusitis; OS, odontogenic sinusitis.
In addition, we assessed the osteitis levels in each disease using the GOSS score. The results showed that bone thickening levels were significantly higher in patients with ECRS than in patients with other diseases, similar to the trend seen in inflammation of the sinus mucosa (Figure 2B). Therefore, we further evaluated the characteristics of bone thickening of ECRS.
Mucosal Inflammation and Bone Thickening Levels in the Sinus Cavity of Patients With ECRS
Figure 3 shows the level of mucosal inflammation and bone thickening in each sinus cavity of the patients with ECRS. As the Japanese criteria for ECRS include the ethmoid-dominant shadow on paranasal CT, the ethmoid sinus is the main location of inflammation in ECRS. Predictably, mucosal inflammation in the ethmoid sinus tended to be stronger than that in other sinus cavities of patients with ECRS. Further, bone thickening levels showed a significantly higher trend for posterior ethmoid sinuses than for anterior ethmoid sinuses; however, no significant difference was observed for other sinuses. The Lund–Mackey score and Global Osteitis Scoring Scale (GOSS) score of each paranasal sinus in patients with eosinophilic chronic rhinosinusitis (ECRS). (A) The Lund–Mackey score and GOSS score of each paranasal sinus in 38 patients with ECRS. (B) The GOSS score of each paranasal sinus in 38 patients with ECRS. **P < .01, as determined by the Kruskal–Wallis test, followed by the Mann–Whitney U test. Values are presented as mean ± standard deviation. LM score, Lund–Mackey score; GOSS, global osteitis scoring scale; FS, frontal sinus; MS, maxillary sinus; AES, anterior ethmoidal sinus; PES, posterior ethmoidal sinus; SS, sphenoid sinus; ECRS, eosinophilic chronic rhinosinusitis; GOSS, global Osteitis Scoring Scale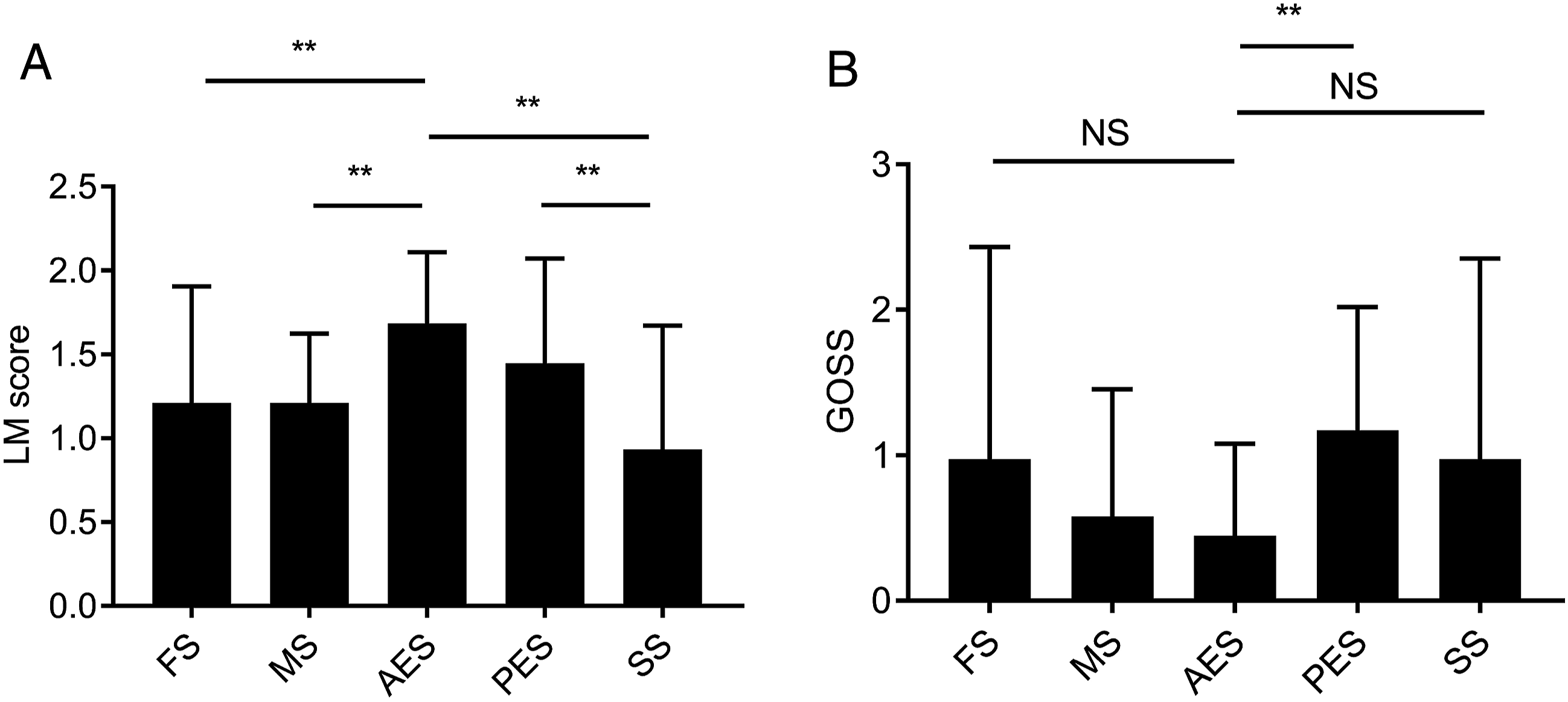
Correlation Between GOSS and Laboratory Data in Patients With ECRS
Further assessment of the correlation between laboratory findings and GOSS scores was performed.
3
The results showed that the GOSS score was not correlated with the white blood cell or neutrophil counts; however, there was a positive correlation between the eosinophil counts and percentages and the GOSS score (Figure 4). Correlations between laboratory data and the Global Osteitis Scoring Scale (GOSS) score in patients with eosinophilic chronic rhinosinusitis (ECRS). Correlation between the GOSS score and white blood cell count, eosinophil count and percentage, and neutrophil count in patients with ECRS (n = 38). WBC, white blood cell; ECRS, eosinophilic chronic rhinosinusitis; GOSS, global Osteitis Scoring Scale.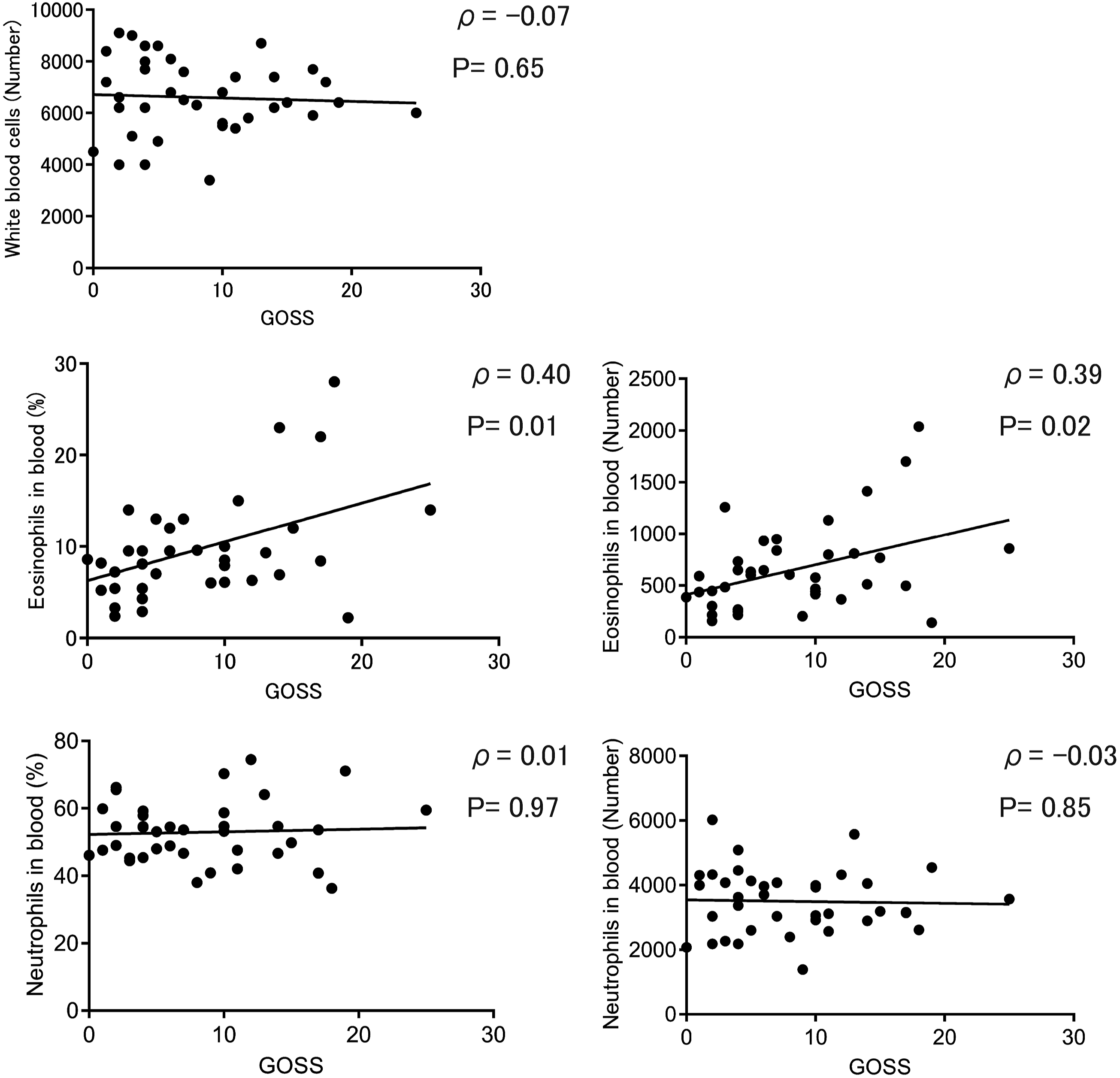
Association Between ECRS Disease Severity and GOSS
We evaluated the correlation between the markers of clinical disease severity of ECRS and the level of bone thickening. The findings showed that there was a strong positive correlation between the polyp score, LM score, JESREC score, clinical stage, and GOSS score (Figure 5), indicating that the more severe the bone thickening, the worse the severity of ECRS. Correlations between clinical disease severity of eosinophilic chronic rhinosinusitis and the Global Osteitis Scoring Scale (GOSS) score. Correlations between the GOSS score and Lund–Mackey score, polyp score, Japanese Epidemiological Survey of Refractory Eosinophilic Chronic Rhinosinusitis (JESREC) score, and stages in patients with eosinophilic chronic rhinosinusitis (n = 38). JESREC, Japanese Epidemiological Survey of Refractory Eosinophilic Chronic Rhinosinusitis; GOSS, global Osteitis Scoring Scale.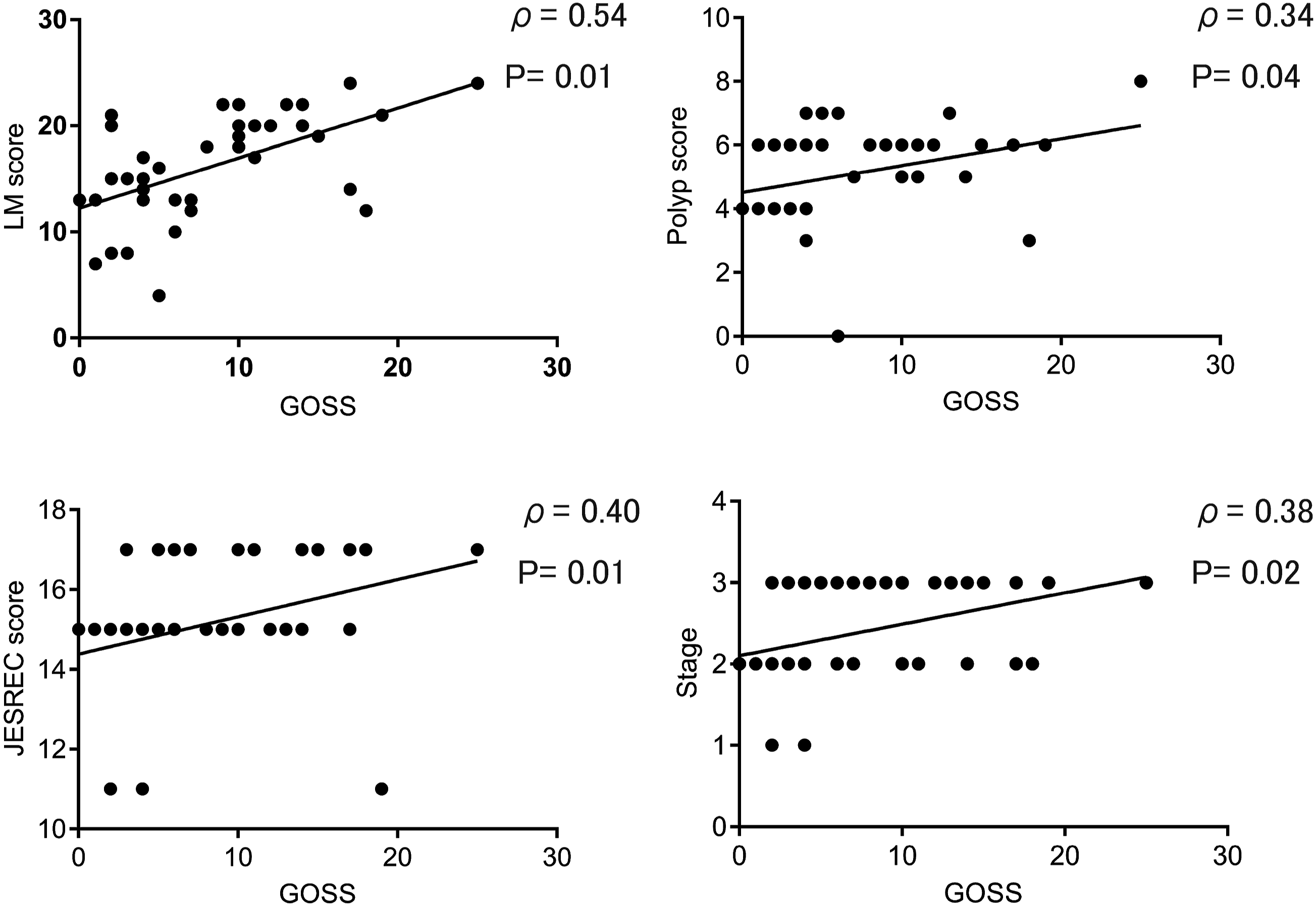
Relationship Between the Level of Bone Thickening, Number of Surgeries, and Recurrence Rate
Previous reports have suggested a causal relationship between the number of surgeries, recurrence rate, and bone thickening. We found a positive correlation between surgical history and the GOSS score, indicating that frequent surgery tended to result in increased bone thickening.
We also evaluated the association between postoperative recurrence and the GOSS score in 34 patients, excluding 4 patients who had not undergone surgery. The results showed that the GOSS score was significantly higher in patients with recurrence than in those without recurrence (Figure 6). Postoperative recurrence and the Global Osteitis Scoring Scale (GOSS) score in patients with eosinophilic chronic rhinosinusitis. (A) Correlations between the GOSS score and number of surgeries in 38 patients with ECRS. (B) The GOSS score in 21 recurrent cases and 13 non-recurrent cases with ECRS (excluding 4 patients who did not undergo surgery). The specific P-value was .03. *P < .05, as determined by the Mann–Whitney U test. ECRS, eosinophilic chronic rhinosinusitis; GOSS, global Osteitis Scoring Scale.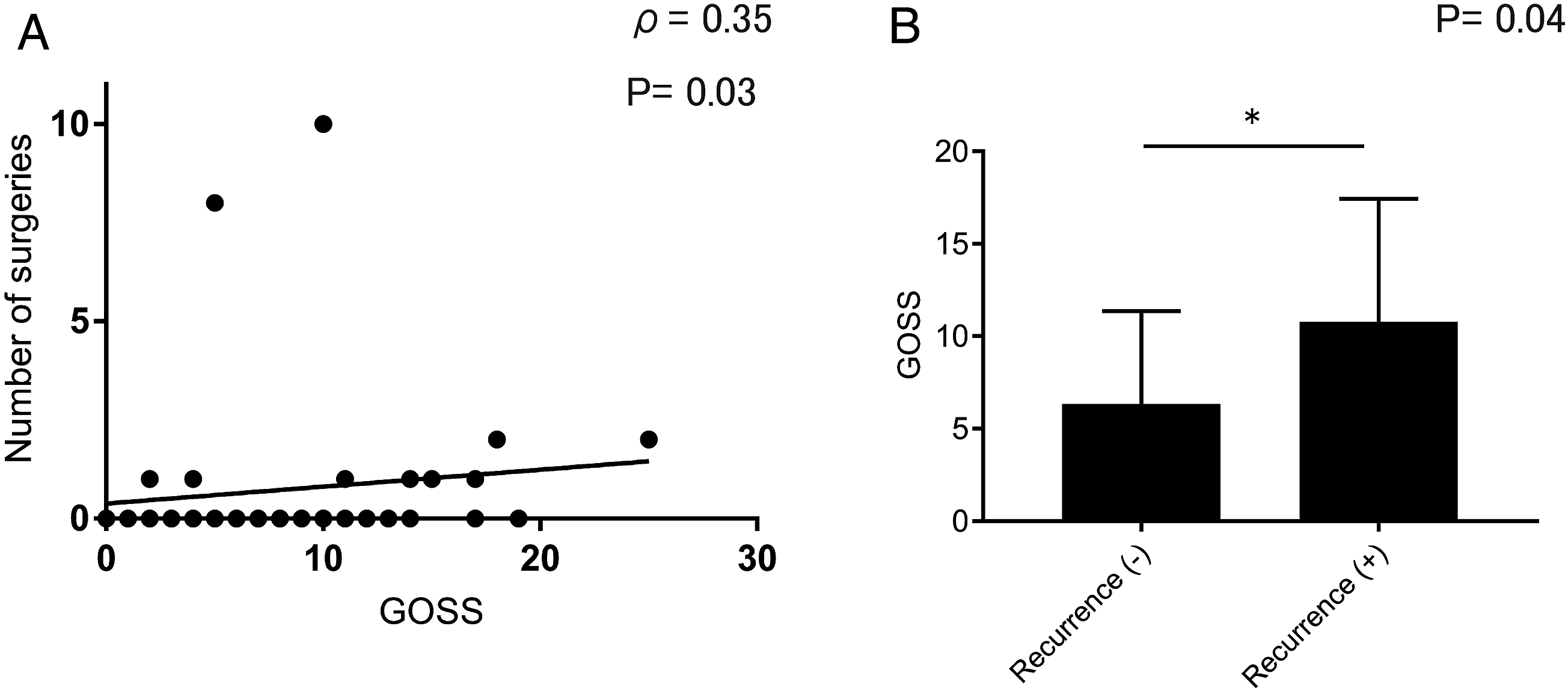
Bone Thickening in the Middle Turbinate and Recurrence
Finally, we focused on the important role of the middle turbinate in intractable cases of ECRS and investigated the relationship between bone thickening of the middle turbinate and recurrence. We evaluated the area of the middle turbinate bone in 25 patients with ECRS with no surgical history; as a result, we found that recurrence after the initial surgery was significantly more common in patients with a strong bony thickening of the middle turbinate (Figure 7). Bone thickening of the middle turbinate and postoperative recurrence of eosinophilic chronic rhinosinusitis (ECRS). Area of the middle turbinate bone in 25 patients with ECRS at initial surgery. No recurrence was observed in 19 patients, whereas 6 patients experienced recurrence. The specific P-value was .003. **P < .01, as determined by the Mann–Whitney U test. ECRS, Eosinophilic chronic rhinosinusitis.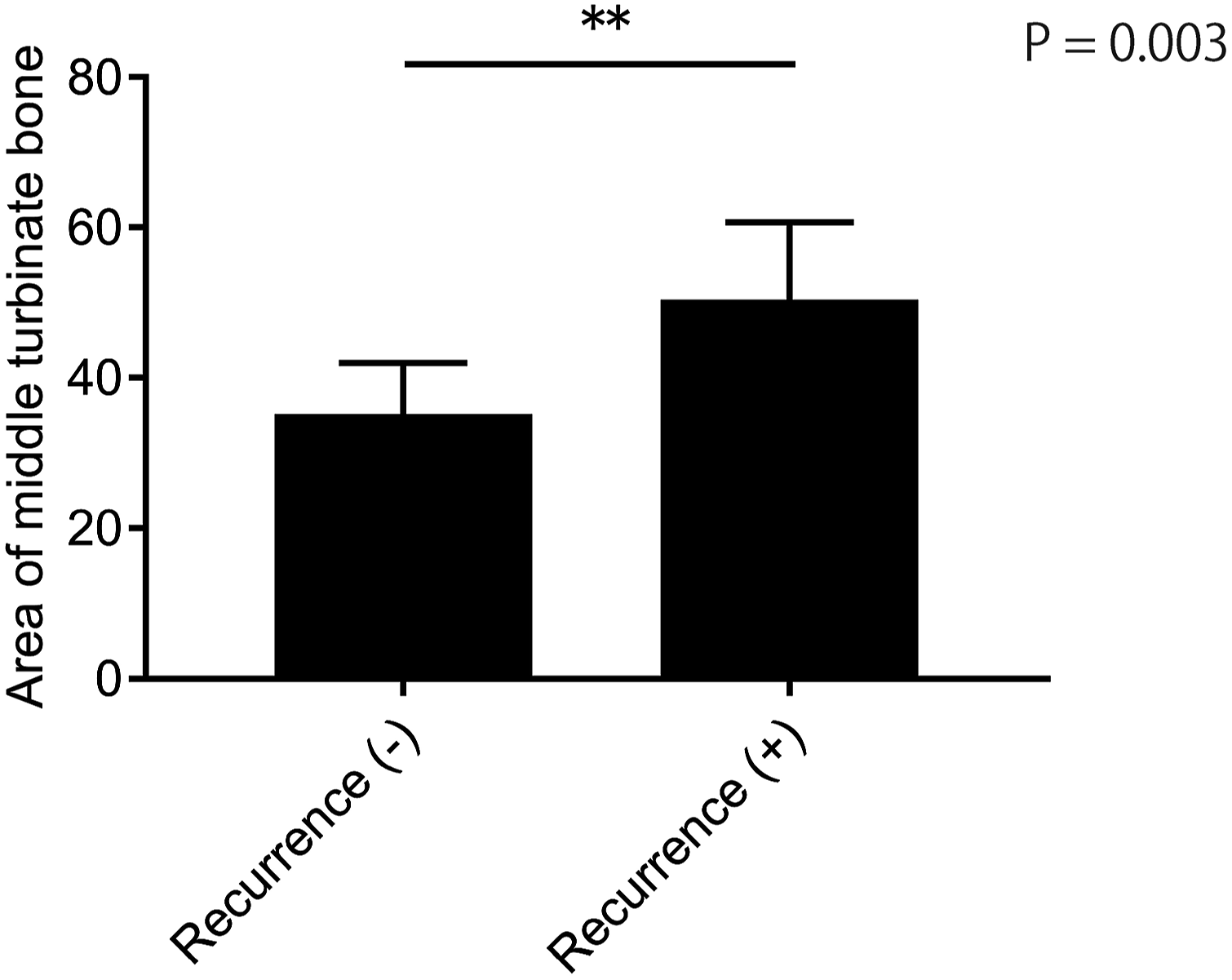
Discussion
Eosinophilic chronic rhinosinusitis is a subtype of chronic rhinosinusitis (CRS) with type 2 inflammation of the sinus mucosa. Inflammation is not confined to the mucosa, and it sometimes spreads to the surrounding bone tissue, resulting in osteitis.12,13 In this study, we demonstrated the pattern of osteitis in patients with ECRS.
First, we assessed the severity of mucosal inflammation and osteitis for each disease. The results showed that ECRS was the strongest of all sinus diseases in terms of both mucosal and bone inflammation, which is consistent with previous reports. The induction of TG-β1 production and osteoblast activation by eosinophils may contribute to the increase in osteitis severity in patients with ECRS. 14 These data are supported by the fact that the higher the eosinophil count in patients with a nasal polyp, the more severe the severity of osteitis. In our study, we found a similar correlation between the number of eosinophils in the blood and level of osteitis.
Next, we evaluated the correlation between disease severity and osteitis in patients with ECRS. Previous reports have shown that the LM score is correlated with the severity of osteitis in CRS.15,16 Similar results were obtained in this study. In addition, a positive correlation was observed with the JESREC score and stage, which are Japanese criteria for ECRS diagnosis, suggesting that osteitis is a good marker for evaluating disease activity in ECRS.
Finally, we examined the effect of surgery on bone thickening in patients with ECRS. As shown previously, bone thickening tended to become more severe as the number of surgeries increased.17-19 In addition, there was a tendency for increased recurrence after surgery in patients with severe bone thickening. Although the etiology of osteitis induced by surgery is not well established, it has been suggested that bacterial invasion and toxins produced by these bacteria may be the cause of osteitis in cases of bone exposure associated with surgical operation. 18 However, osteitis is also observed in patients without previous surgery, suggesting that there is more than 1 mechanism that causes bone thickening.
In the paranasal sinus region, there is a small bone partition separating each paranasal sinus that can be resected during endoscopic sinus surgery; however, the skull base and orbital walls are usually not resectable. There is a possibility of osteitis in these unresectable bony plates. Whether bone thickening in ECRS can be improved by conservative treatment has not been fully investigated, and within the scope of our search, we found only 1 report of improvement in bone thickening with steroid use in a mouse model of rhinosinusitis. 20 In recent years, monoclonal antibodies therapy have been recommended for refractory cases of ECRS, and it will be important to further investigate whether they can improve inflammation in unresectable bone osteitis. Under these circumstances, management of the middle turbinate is controversial. There have been various reports on the resection of the middle turbinate, including total resection, partial resection, and resection of only the bone of the middle turbinate.5-7 Since the middle turbinate is an important landmark during surgery, its removal may make reoperation more difficult. 8 In addition, some reports suggest that it may cause olfactory disturbances and atrophic rhinitis nasal obstruction; however, it has also been reported that resection of the middle turbinate has the advantage of improving drug delivery, improving the postoperative endoscopy score, and decreasing nasal resistance.8,21-28 Based on our results, it seems to be important to use a therapeutic approach in patients with bony thickening of the middle turbinate.
The limitation of this study is that it was a single-center study with a relatively small number of patients. In addition, the mechanism of accelerated bone metabolism in patients with ECRS has not been fully investigated. In a recent study, BMP-2, a kind of bone morphogenetic protein that is a member of the TGF-β protein family, was shown to induce remodeling of human nasal epithelial cells; therefore, further studies in this regard are required. 29 However, the study has novel features: we investigated the role of osteitis in the middle turbinate in ECRS recurrence.
Conclusion
The patients with ECRS tended to have more severe osteitis and mucosal inflammation than the patients with other sinus diseases. Furthermore, the level of osteitis in ECRS correlated with disease severity, and patients with severe osteitis tended to experience increased recurrence. Because there are many cases of postoperative recurrence, it may be important to treat the middle turbinate during surgery in patients with bony thickening of the middle turbinate.
Footnotes
Acknowledgments
We thank Dr Masaki Hayama for advice on our research.
Author Contributions
HN supervised the project. TT analyzed the data and wrote the manuscript. KT, RT, ST, SW, and TA provided advice on project planning and data interpretation. All authors participated in the discussion of the results and critically reviewed and approved the final draft of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, TT, upon reasonable request.