
Abstract
Objectives
Chronic rhinosinusitis (CRS) is a common disease with mucosal inflammation, and may sometimes be accompanied by bone thickening. The disease is usually bilateral; when it is unilateral, there may be a specific disease. This study aimed to investigate the association between unilateral sinus opacification and osteitis.
Methods
In total, 104 patients with computed tomography revealing unilateral sinus opacification were included in this study. Patients were retrospectively evaluated using the Global Osteitis Scoring Scale (GOSS) score, Lund–Mackey (LM) score, polyp score, and blood tests.
Results
In total, 47, 11, 9, 17, and 20 patients had CRS, paranasal sinus cyst, inverted papilloma, mycetoma, and odontogenic sinusitis, respectively. The GOSS score in patients with mycetoma was higher than that in patients with CRS. However, no significant differences in the GOSS scores between patients with mycetoma, inverted papilloma, and odontogenic sinusitis existed. 10 of the 104 patients had osteitis with extensive bone thickening and a GOSS score of 4 or higher. Patients with CRS and mycetoma tended to have a higher GOSS score for the maxillary sinus than for the other sinuses. There was a significant positive correlation between the GOSS score and LM score in patients with diseases other than paranasal sinus cyst.
Conclusions
Mycetoma is more likely to cause osteitis than CRS, and a unique mechanism of osteitis exacerbation is predicted. As there is a positive correlation between bone thickening and sinus inflammation, a close association between osteitis and mucosal inflammation is inferred in diseases involving unilateral sinus opacification.
Introduction
Chronic rhinosinusitis (CRS) causes chronic inflammation of the sinus mucosa, resulting in mucosal thickening, sometimes accompanied by bony thickening.1,2 These bony changes have been described by histological analysis as a process of neo-osteogenesis, and is referred to as osteitis. The presence of osteitis of the paranasal sinuses is also common, especially in severe paranasal sinus diseases.
Osteitis of sinuses was first noted in an animal model of sinusitis, and the focus is now on human CRS.3,4 Computed tomography (CT) is useful in the evaluation of chronic rhinosinusitis with osteitis, and various methods of evaluation have been reported to date.5-7
The Global Osteitis Scoring Scale (GOSS) is a CT-based method for assessing bone thickening, that was developed by otolaryngologists and radiologists. It is a method for evaluating the anterior ethmoid, posterior ethmoid, maxillary, frontal, and sphenoid sinuses on a 5-point scale from grades 1 to 5 based on right and left sides, and shows low inter-rater assessment variability. 8 The severity of bone thickening as assessed by the GOSS score is known to correlate well with mucosal inflammation of the sinuses.
In patients with chronic rhinosinusitis, bilateral shadows in the paranasal sinuses are usually detected by CT. In contrast, unilateral opacification of the paranasal sinuses can be observed in a variety of other diseases in addition to chronic rhinosinusitis, such as mycetoma, odontogenic sinusitis, and inverted papilloma.9 -12 These pathologies are different from chronic rhinosinusitis, and the developmental pattern of osteitis has not been fully investigated. This study aimed to investigate the pattern of osteitis in diseases associated with unilateral sinus opacification.
Patients and Methods
Patient Profiles
Patients who visited our department for nasal symptoms and demonstrated unilateral sinus opacification on nasal and paranasal CT at our hospital between April 2014 and June 2021 were included in the study; patients with malignancies were excluded from the study. This study was approved by the ethics committee of the National Hospital Organization Osaka National Hospital (No. 21061). Informed consent was obtained from the patients through an opt-out system via the hospital website. Patients who opted out were excluded from the study.
Computed Tomography (CT) Scan Protocols
The CT scan protocols were standardized to ensure that the radiation dose was based on the 17 mGy computed tomography dose index (CTDI); slight adjustments were made according to body size and other factors, .6 mm slice thickness, and the bone window.
Diagnosis of Paranasal Disease
The level of bone thickening was assessed using the GOSS, and sinus inflammation was assessed using the Lund–Mackey score (LM score). 8 A paranasal cyst was diagnosed in cases with characteristic expansive shadows on CT, and cystic effusions without infection observed during surgery. Inverted papilloma was confirmed by preoperative biopsy or intraoperative rapid diagnosis. Mycetoma was defined by preoperative or intraoperative evidence of a fungal mass. The diagnosis of odontogenic sinusitis was confirmed based on a CT scan showing either periapical lucency or oroantral fistula, and consultation with our oral surgeon. Cases that did not satisfy these criteria and showed polyp formation or pus accumulation in the sinuses were diagnosed as CRS.
Statistical Analyses
All statistical analyses were performed using the Prism version 7 (GraphPad Software, San Diego, CA, USA); data are expressed as means ± standard deviation. Comparisons between two groups were performed using the nonparametric Mann–Whitney U test; Kruskal–Wallis tests were performed to compare multiple groups. Correlations are expressed as the Spearman’s rank correlation coefficient. Analysis of variance was performed to evaluate differences between the two groups. P-values of <.05 were considered statistically significant.
Results
Disease-Specific GOSS Score
Clinical and Demographic Data of Study Participants.
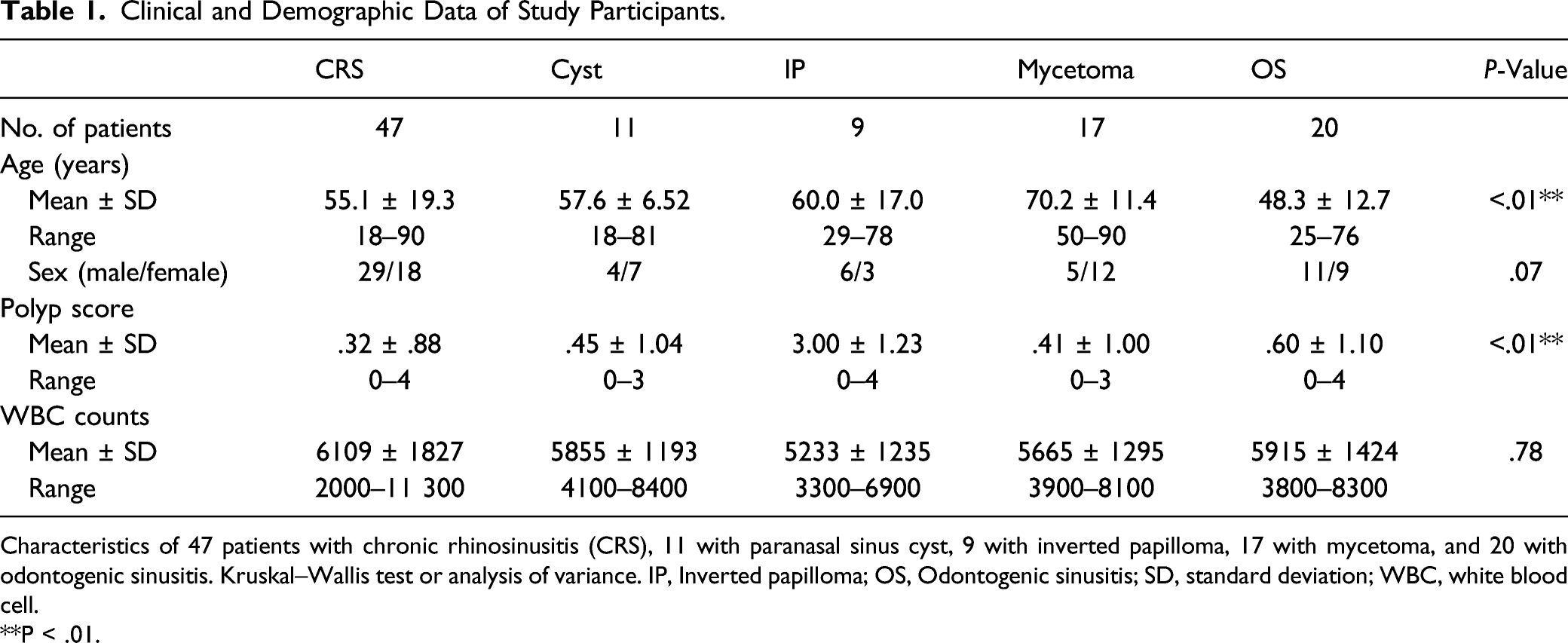
Characteristics of 47 patients with chronic rhinosinusitis (CRS), 11 with paranasal sinus cyst, 9 with inverted papilloma, 17 with mycetoma, and 20 with odontogenic sinusitis. Kruskal–Wallis test or analysis of variance. IP, Inverted papilloma; OS, Odontogenic sinusitis; SD, standard deviation; WBC, white blood cell.
**P < .01.
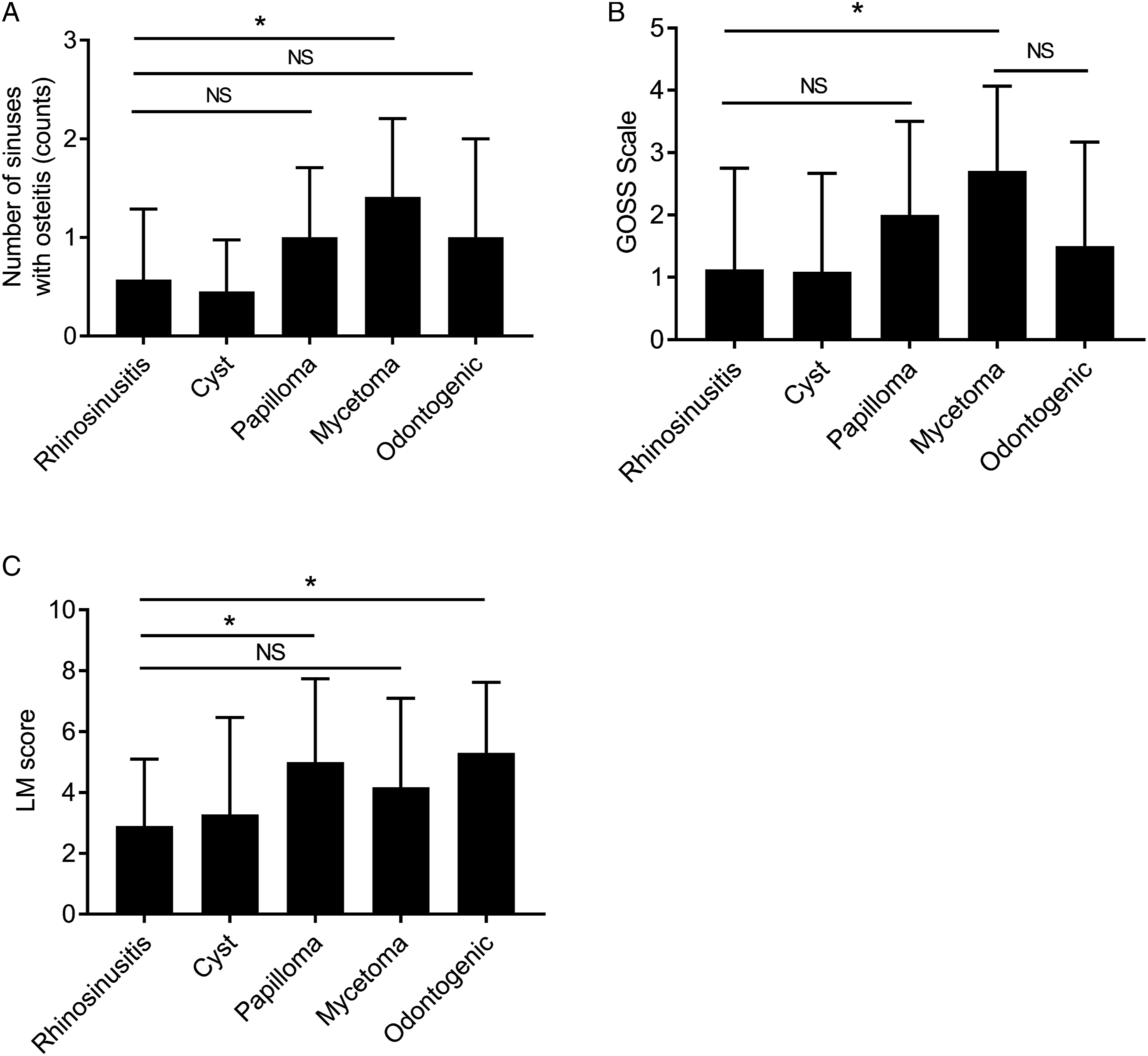
Disease-specific Global Osteitis Scoring Scale score and Lund–Mackey score. (A) Number of sinuses with osteitis in 47 patients with chronic rhinosinusitis (CRS), 11 with paranasal sinus cyst, 9 with inverted papilloma, 17 with mycetoma, and 20 with odontogenic sinusitis. (B) Global Osteitis Scoring Scale (GOSS) score of 47 patients with chronic rhinosinusitis (CRS), 11 with paranasal sinus cyst, 9 with inverted papilloma, 17 with mycetoma, and 20 with odontogenic sinusitis. (C) Lund–Mackey score (LM score) of 47 patients with CRS, 11 with paranasal sinus cyst, 9 with inverted papilloma, 17 with mycetoma, and 20 with odontogenic sinusitis. * P < .05, as determined by the Kruskal–Wallis test followed by the Mann–Whitney U test. Values are presented as means ± standard deviation. NS, Not significant.
We also assessed the GOSS score by individual disease. Similar to the results for the number of sinuses with osteitis, the GOSS score was significantly higher in patients with mycetoma than in those with chronic rhinosinusitis (Figure 1B). Images of typical osteitis for each disease are shown in Supplemental Figure 1.
A further assessment of sinus inflammation for each disease using the LM score showed a significantly higher trend for inverted papilloma and odontogenic sinusitis than for chronic rhinosinusitis. However, no significant difference was observed for mycetoma (Figure 1C).
Pattern of Osteitis
Number of Patients With Severe Bone Thickening by Disease Category.
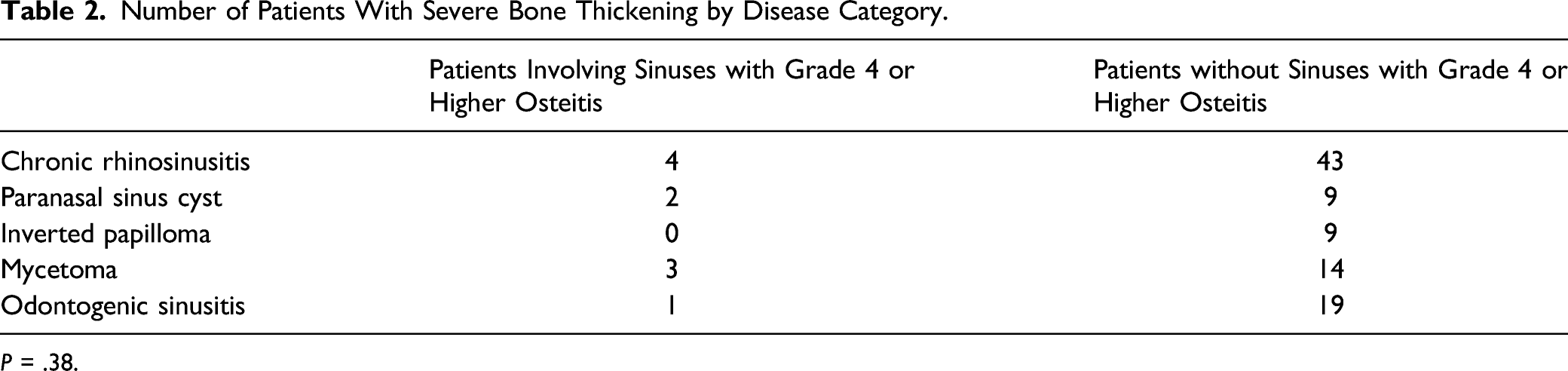
P = .38.
GOSS score of 4 or higher for osteitis by disease category. Analysis of variance was performed to evaluate the variance between the two groups.
GOSS Score by Each Sinus
The details of the tendency of sinuses to develop bone thickening are shown in Figure 2. In all cases, the GOSS score was significantly higher in the maxillary sinus than in the other sinuses. We also assessed each disease and found that patients with chronic rhinosinusitis and mycetoma had a significantly higher GOSS score in the maxillary sinus than in the other sinuses. Conversely, there was no difference in osteitis between the sinuses in patients with paranasal sinus cyst, inverted papilloma, or odontogenic sinusitis (Figure 2). We speculated that this result was due to the maxillary sinus being the most common site of inflammation; as expected, the maxillary sinus was the most common sinus with mucosal thickening in all of the diseases, except inverted papilloma (Supplemental Figure 2). Global Osteitis Scoring Scale score of each paranasal sinus. Global Osteitis Scoring Scale score of each paranasal sinus in 47 patients with chronic rhinosinusitis, 11 with paranasal sinus cyst, 9 with inverted papilloma, 17 with mycetoma, and 20 with odontogenic sinusitis. **
P < .01, as determined by the Kruskal–Wallis test followed by the Mann–Whitney U test FS, Frontal sinus; MS, Maxillary sinus; AES, Anterior ethmoidal sinus; PES, Posterior ethmoidal sinus; SS, Sphenoid sinus; GOSS, Global Osteitis Scoring Scale; CRS, Chronic rhinosinusitis; IP, Inverted papilloma; OS, Odontogenic sinusitis; NS, Not significant.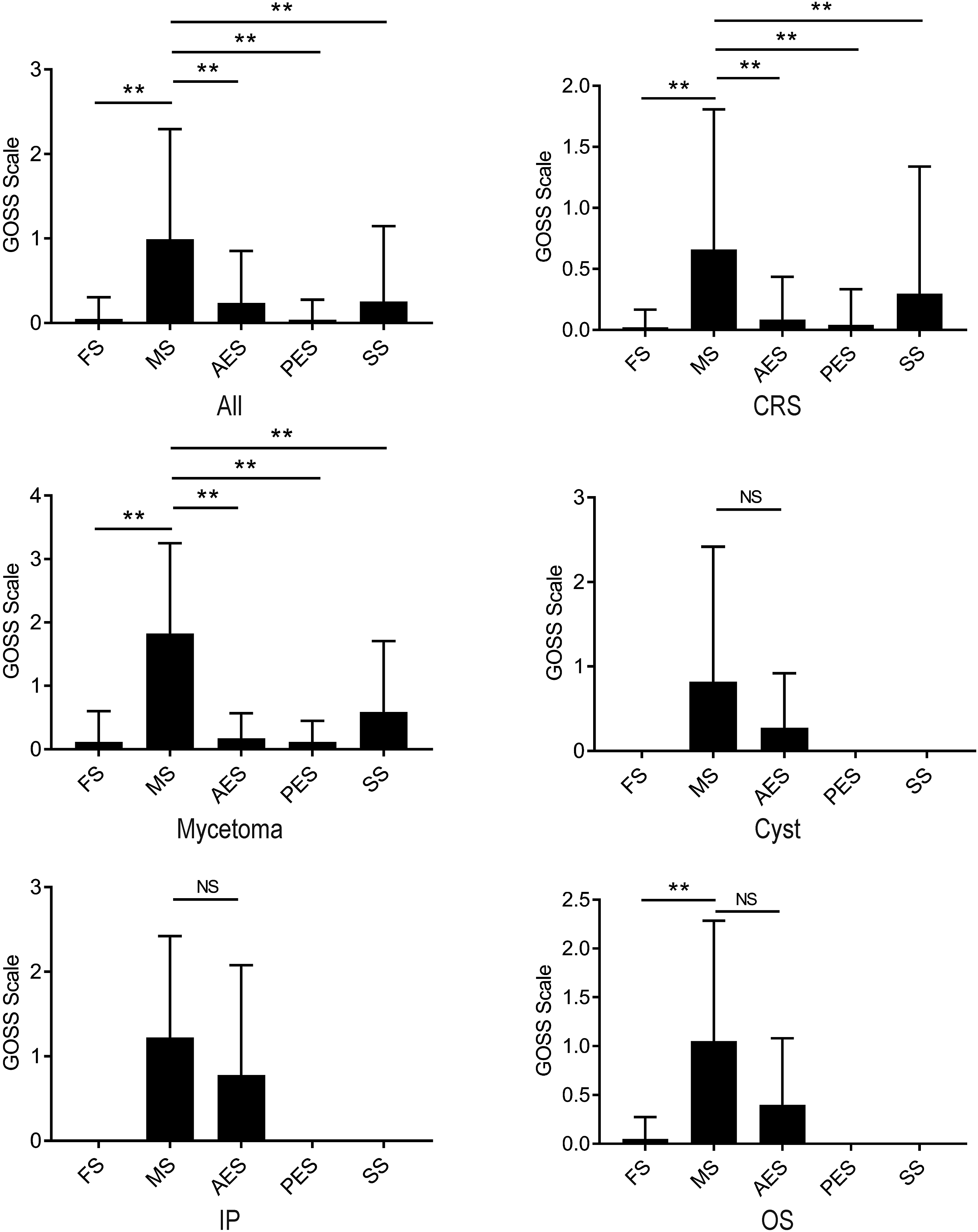
Correlation Between GOSS Score and Disease Severity
Finally, we assessed the correlation between the level of bone thickening and severity of disease for each disease. The results showed a significant correlation between the GOSS score and LM score in patients with chronic rhinosinusitis, inverted papilloma, mycetoma, and odontogenic sinusitis. In contrast, there was no significant correlation with paranasal cyst (Figure 3). There were no significant correlations with other clinical findings, such as polyp score, white blood cell count, neutrophil count, and eosinophil count. However, there was a high correlation coefficient between the GOSS score and polyp score in patients with mycetoma (Supplemental Figures 3–7). Correlations between Global Osteitis Scoring Scale score and Lund–Mackey score. Correlations between Global Osteitis Scoring Scale (GOSS) and Lund–Mackey score (LM score) of 47 patients with chronic rhinosinusitis, 11 with paranasal sinus cyst, 9 with inverted papilloma, 17 with mycetoma, and 20 with OS. Correlations are expressed as the Spearman’s rank correlation coefficient. GOSS, Global Osteitis Scoring Scale; CRS, Chronic rhinosinusitis; IP, Inverted papilloma; OS, Odontogenic sinusitis.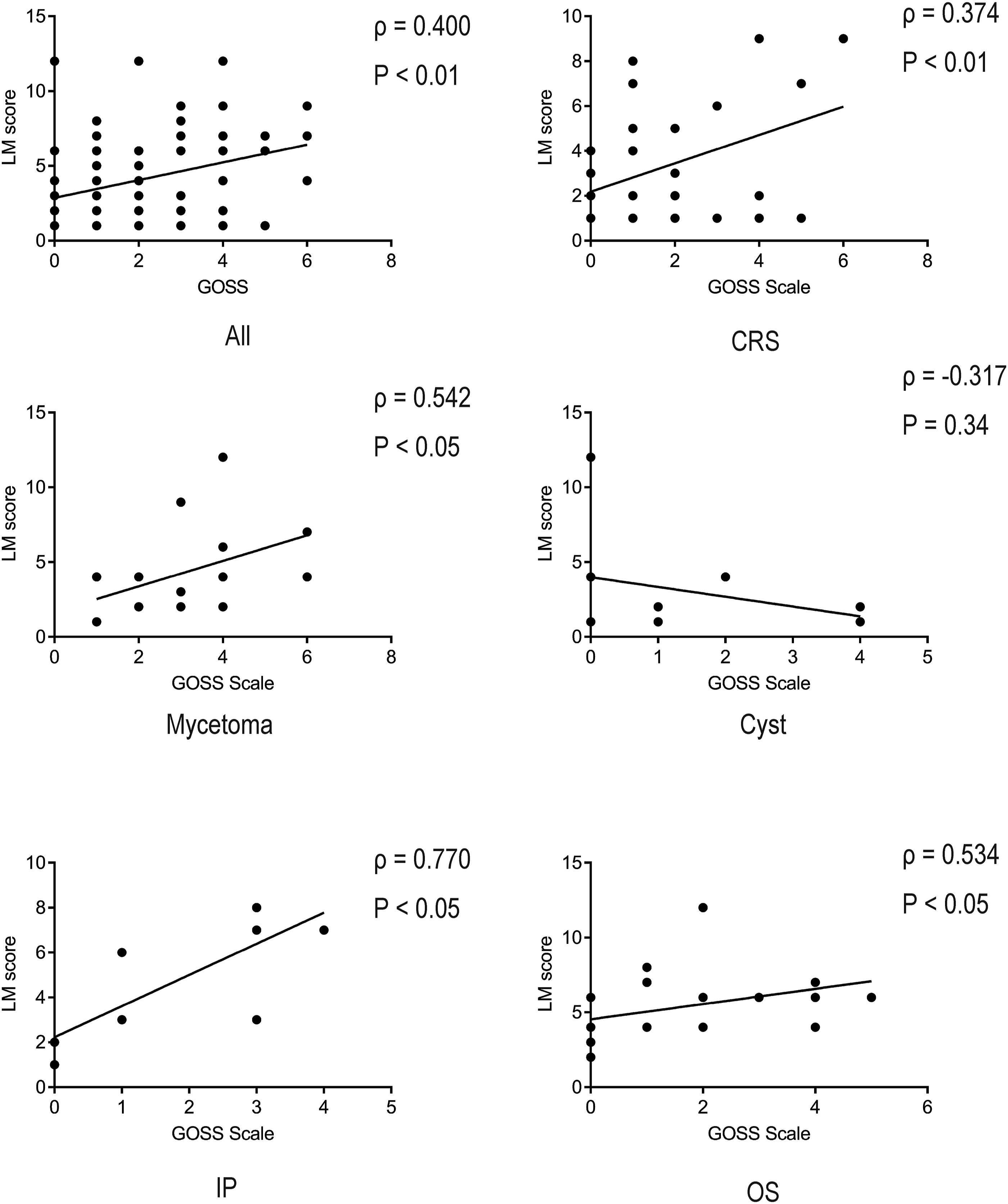
Discussion
Chronic rhinosinusitis causes inflammation of the sinus mucosa, and may also cause inflammation of the bone. Chronic sinusitis is often associated with bilateral sinus shadows on CT; however, diseases with unilateral sinus opacification often include odontogenic sinusitis, mycetoma, and paranasal tumors. There are considerably few reports on bone thickening in relation to these diseases.
Initially, we investigated the diseases that predispose bones to thickening, and found that mycetoma was more likely to cause bone thickening than chronic rhinosinusitis. In contrast, there was no significant difference between odontogenic sinus and inverted papilloma in this regard. Previous reports have shown that mycetoma tends to be associated with greater bone thickening than odontogenic sinusitis.13,14 Although there was no significant difference, the overall GOSS score tended to be higher in mycetoma. The points at which statistical significance could not be confirmed were due to variability between the cases. There have been several reports on fungal infections and bone metabolism, including Austalide K from the fungus Penicillium rudallense, which promotes bone thickening by inhibiting osteoclast differentiation, and Aspergillus flocculosus, which inhibits osteoclast differentiation by inhibiting the receptor activator of nuclear factor kappa B ligand production.15,16 These fungal-specific mechanisms of osteogenesis may be one of the factors that predispose patients to osteitis in mycetoma.
Subsequently, as none of the previous studies referred to the pattern of bone thickening, we examined the tendency to develop extensive bone thickening in each disease. In this study, there were significantly few cases of extensive bone thickening above a GOSS score of 4, and no significant differences were found between the diseases. In particular, there were no cases of osteitis with a GOSS score of 4 or higher in any of the 9 cases with inverted papillomas; however, the small number of cases was considered one of the reasons behind this. It is common to find marked bony thickening at the attachment of inverted papilloma; indeed, in our study, almost all of the patients (7/9 patients) had thickening at the stem.17,18 No reports examining why tumor attachment is more likely to be associated with strong calcification in inverted papilloma were found. Considering the possibility that bone morphogenetic protein 4, 19 which induces osteoblast migration, is expressed in calcification-prone inverted papilloma and tumor attachment sites being penetrated by tumor vessels have a role in calcification tendency, further research is needed to elucidate this.
Since no previous study was identified that assessed osteitis by disease or by sinus, we assessed the areas of the sinuses most likely to cause osteitis. Our study showed that the GOSS score tends to be significantly higher in the maxillary sinus in patients with chronic rhinosinusitis and mycetoma. Similarly, it was assumed that the GOSS score for the maxillary sinus would be higher in odontogenic sinusitis. This was thought to be due to the maxillary sinus being the most frequently inflamed sinus in this group of patients with unilateral sinus opacification.
Finally, we analyzed the correlation between osteitis and disease severity. Previous reports have suggested that patients with chronic rhinosinusitis with bone thickening have a significantly higher LM score than those without bone thickening. 7 It has also been reported that the severity of osteitis is positively correlated with the LM score, and there was a significant positive correlation between the GOSS score and LM score in odontogenic sinusitis, mycetoma, and chronic rhinosinusitis in our study.5-7
This study has the limitation of being conducted at a single institution; as a result, the number of cases was small, and the patient background was not standardized. Although the sample size is small, no other reports have evaluated osteitis in unilateral sinusitis; we therefore believe that the findings of this pilot study are meaningful. Further studies with larger sample sizes are needed to validate our findings. Additionally, there may be a mechanism that predisposes patients to osteitis in diseases involving unilateral sinus opacification; however, these mechanisms have not been investigated in detail.
In this study, we investigated osteitis in patients with unilateral sinus opacification using paranasal CT. Of all the diseases causing unilateral sinus shadowing, mycetoma was more likely to cause osteitis than chronic rhinosinusitis, suggesting the presence of a unique osteitis-promoting mechanism. There was a significant correlation between the GOSS score and LM score, suggesting that osteitis and mucosal inflammation are closely associated with diseases involving unilateral sinus shadowing and bilateral chronic rhinosinusitis.
Supplemental Material
sj-pdf-1-ear-10.1177_01455613221074957 – Supplemental Material for Osteitis in Diseases With Unilateral Opacification of Paranasal Sinuses
Supplemental Material, sj-pdf-1-ear-10.1177_01455613221074957 for Osteitis in Diseases With Unilateral Opacification of Paranasal Sinuses by Takeshi Tsuda, Kazuya Takeda, Risa Terada, Shohei Tanaka, Sadanori Waki, Toshiyuki Akama and Hiroshi Nishimura in Ear, Nose & Throat Journal
Supplemental Material
sj-pdf-2-ear-10.1177_01455613221074957 – Supplemental Material for Osteitis in Diseases With Unilateral Opacification of Paranasal Sinuses
Supplemental Material, sj-pdf-2-ear-10.1177_01455613221074957 for Osteitis in Diseases With Unilateral Opacification of Paranasal Sinuses by Takeshi Tsuda, Kazuya Takeda, Risa Terada, Shohei Tanaka, Sadanori Waki, Toshiyuki Akama and Hiroshi Nishimura in Ear, Nose & Throat Journal
Footnotes
Acknowledgments
None.
Author Contributions
HN supervised the project. TT analyzed the data and wrote the manuscript. KT, RT, ST, SW, and TA provided advice on project planning and data interpretation. All authors participated in the discussion of the results and critically reviewed and approved the final draft of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Data Accessibility
The data obtained in this study are available from the corresponding author, TT, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.