
Abstract
Significance Statement
Chronic Eustachian tube dilatory dysfunction (ETD) refers to failure of the ventilatory functions of the Eustachian tube (ET), which can lead to otitis media with effusion (OME), retraction pockets, and cholesteatoma.1,2 The pathogenesis may be related to dysfunction of the dilation mechanism of ET, due to primary mucosal disease, and anatomical obstruction. 3 Here, we report a case of chronic ETD as a manifestation of meningioma and highlight the importance of first-line imaging in the diagnosis.
Case Presentation
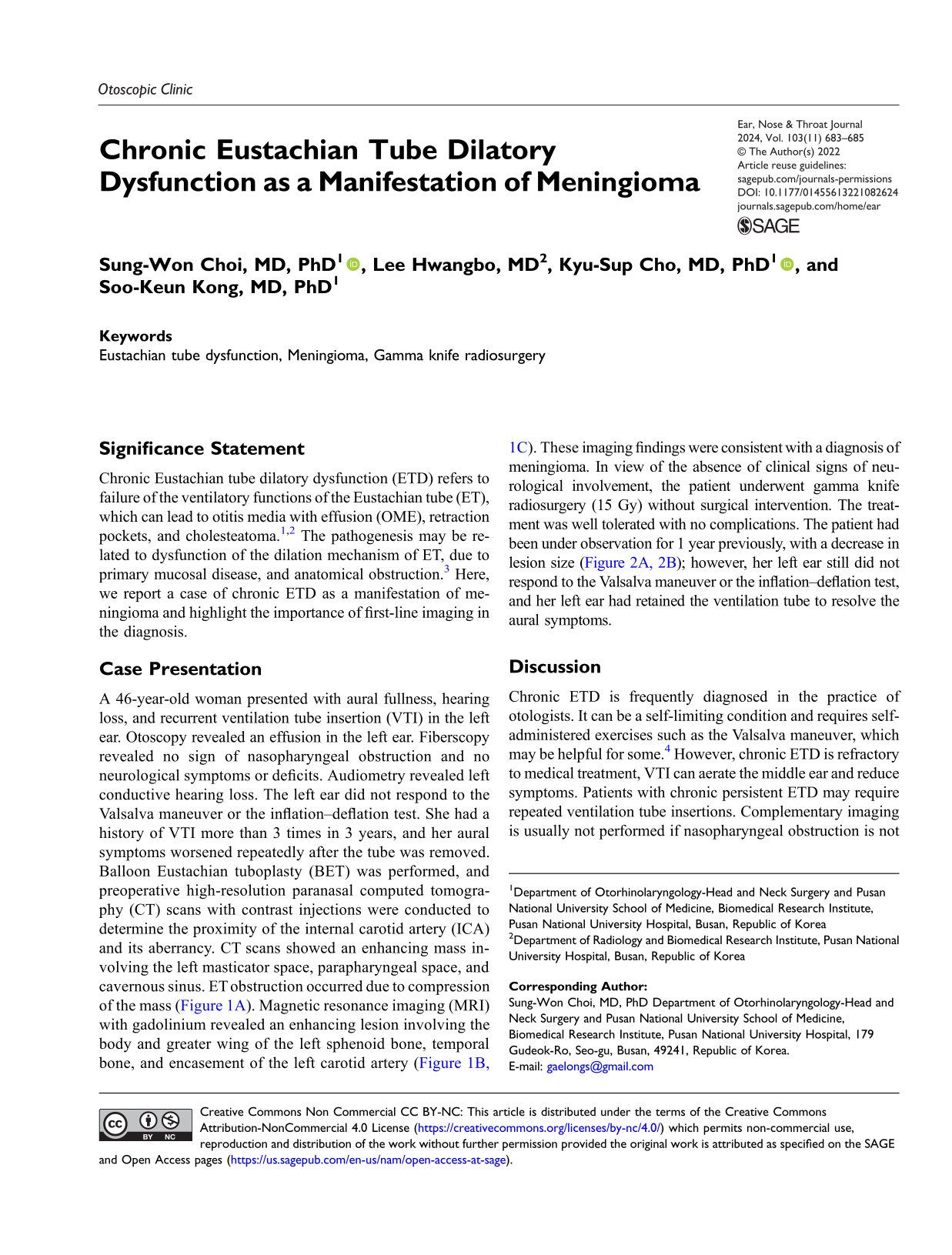
A 46-year-old woman presented with aural fullness, hearing loss, and recurrent ventilation tube insertion (VTI) in the left ear. Otoscopy revealed an effusion in the left ear. Fiberscopy revealed no sign of nasopharyngeal obstruction and no neurological symptoms or deficits. Audiometry revealed left conductive hearing loss. The left ear did not respond to the Valsalva maneuver or the inflation–deflation test. She had a history of VTI more than 3 times in 3 years, and her aural symptoms worsened repeatedly after the tube was removed. Balloon Eustachian tuboplasty (BET) was performed, and preoperative high-resolution paranasal computed tomography (CT) scans with contrast injections were conducted to determine the proximity of the internal carotid artery (ICA) and its aberrancy. CT scans showed an enhancing mass involving the left masticator space, parapharyngeal space, and cavernous sinus. ET obstruction occurred due to compression of the mass (Figure 1A). Magnetic resonance imaging (MRI) with gadolinium revealed an enhancing lesion involving the body and greater wing of the left sphenoid bone, temporal bone, and encasement of the left carotid artery (Figure 1B, 1C). These imaging findings were consistent with a diagnosis of meningioma. In view of the absence of clinical signs of neurological involvement, the patient underwent gamma knife radiosurgery (15 Gy) without surgical intervention. The treatment was well tolerated with no complications. The patient had been under observation for 1 year previously, with a decrease in lesion size (Figure 2A, 2B); however, her left ear still did not respond to the Valsalva maneuver or the inflation–deflation test, and her left ear had retained the ventilation tube to resolve the aural symptoms. (A) The initial contrast-enhanced paranasal CT revealed an avidly enhancing mass of the left masticator space (white line), foramen ovale, middle cranial fossa, and ipsilateral cavernous sinus. Peritumoral hyperostosis was noted at the pterygoid plate (arrow heads), and the mass exhibited extrinsic compression of the Eustachian tube (arrow). The tumor texture on the coronal T2-weighted (B) and contrast enhanced fat-suppressed T1-weighted images (C) was highly suggestive of meningioma based on the sunburst appearance of the dark signal (arrowheads) and lack of cystic portions. Note that the lesion spreads through the foramen ovale (arrow), and encases the cavernous segment of the left ICA (asterisk). The mass at the masticator space (asterisk) of pre- (A) and post-Gamma Knife radiosurgery (GKRS) (B) on fat-suppressed T1-weighted images. This initial follow-up MRI, 12 months after GKRS, revealed a decreased volume of the lesion, implying responsiveness to treatment.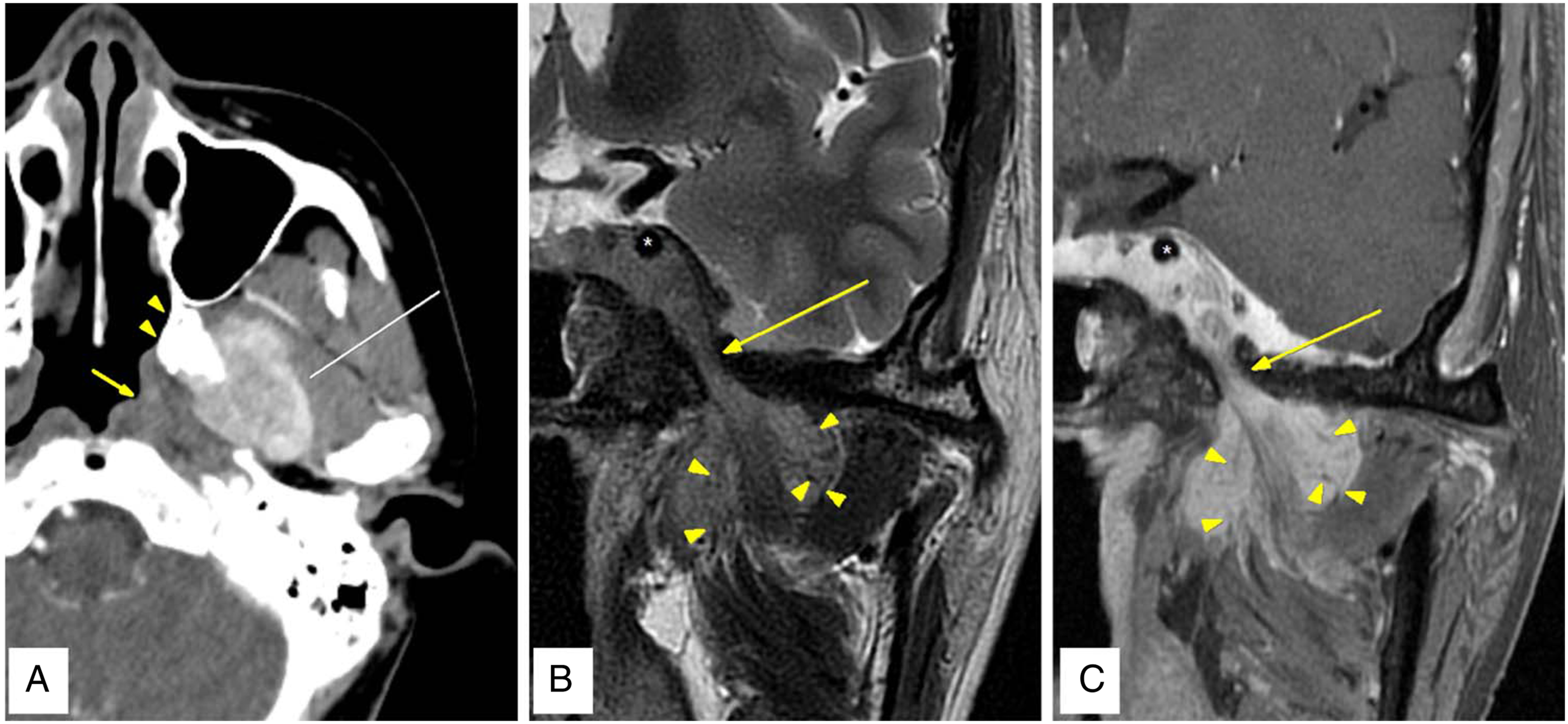
Discussion
Chronic ETD is frequently diagnosed in the practice of otologists. It can be a self-limiting condition and requires self-administered exercises such as the Valsalva maneuver, which may be helpful for some. 4 However, chronic ETD is refractory to medical treatment, VTI can aerate the middle ear and reduce symptoms. Patients with chronic persistent ETD may require repeated ventilation tube insertions. Complementary imaging is usually not performed if nasopharyngeal obstruction is not confirmed by fiberscopy. Recently, BET is also being administered more frequently. 5 Previously, CT was not usually performed before BET. Alternatively, a CT would be carried out without contrast enhancement, resulting in an inability to detect intracranial components such as meningiomas. 3 Diagnoses of meningiomas extending to the ET have been extremely rare, and to date, few cases of meningiomas extending to the ET without other neurological symptoms have been reported as chronic ETDs.
Meningiomas are the second most common tumors of the cerebellopontine angle, comprising 10%–15%. 5 If a BET is planned for chronic ETD, even if a nasopharyngeal tumor has been ruled out by fiberscopy, we recommend that CT be performed with a contrast injection, not only to identify the proximity of the ICA and its aberrancy but also not to misdiagnose an intracranial lesion. In conclusion, meningiomas involving the ET can mimic chronic ETDs. In cases of unilateral, chronic, and persistent ETDs, complementary imaging should be performed in the interests of accurate diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.