
Abstract
Objectives
Multiple affected salivary gland diseases are rare compared to single gland diseases and represent a major diagnostic challenge. These cases are commonly neglected in the scientific literature, despite the considerable suffering of these patients. The aim of this retrospective study was to report disease characteristics, diagnostic pathways, and therapeutic options, including sialendoscopic treatment of multiple affected salivary gland disorders.
Methods
Patients experiencing multiple affected salivary gland diseases treated between 2013 and 2020 were consecutively identified. Data regarding demographics, clinical presentation, disease characteristics, treatment, complications, and follow-up were analyzed retrospectively.
Results
In total, 71 patients were identified with these diseases and included obstructive disease without sialolithiasis (n = 22), inflammation (n = 15), immune disease (n = 19), radioiodine-induced sialadenitis (RAI) (n = 5), sialadenosis (n = 2), and juvenile recurrent parotitis (JRP) (n = 8). Diagnostic and therapeutic sialendoscopy was performed on 113 salivary glands in 42 patients, leading to completely (n = 27, 64.3%) or partially (n = 11, 26.2%) improved symptoms in most cases. In total, 4 patients did not improve after interventional therapy.
Conclusions
Multiple affected salivary gland diseases are rare and diagnostically challenging. Interventional sialendoscopy offers an effective and safe therapeutic option and should be considered in this specific cohort.
Introduction
Salivary gland diseases are common and can manifest as recurrent swelling, pain, changes in taste, and xerostomy. Obstructive salivary gland diseases are the most common non-neoplastic disorders and are characterized by recurrent meal-dependent pain and swelling of the gland. They are generally caused by calculi, ductal stenosis, fibromucinous plugs, foreign bodies, or anatomic variants of the ductal system.1,2 In most cases, only one single gland is affected and the diagnosis can be easily assessed by clinical and ultrasonographic examination.
During the past decade, sialendoscopic intervention has been described as an efficient treatment option in approximately 76-91% of this cohort.3-13 However, a “non-stone” affection of the salivary glands represents a diagnostically and therapeutically challenging entity. In particular, when multiple glands are affected, patients present with considerable suffering and deterioration in their quality of life. The differential diagnosis is vast (e.g., infectious, inflammatory, Sjögren syndrome, radioiodine-induced sialadenitis (RAI), and obstructive disease without sialolithiasis). The clinical picture in multiple affected gland disorders is more complex and difficult to interpret. In this context, entities such as Sjögren syndrome are well described and studied in the literature.
Recent investigations showed a positive therapeutic effect with sialendoscopic intervention.14-16 However, many patients with multiple affected gland disorders still receive no diagnosis or efficient treatment. The literature is sparse, especially regarding the diagnostic and therapeutic work-up in these patients. Therefore, the purpose of this study is to report our experience regarding the diagnostic work-up, therapeutic procedures, and outcomes in patients with multiple affected salivary gland disorders.
Patients and Methods
Ethical Issues
Approval to perform this study was obtained from our Institutional Review Board (Kantonale Ethikkommission Bern, Switzerland, KEK-Nr. 2020-01483). The study was carried out according to the Declaration of Helsinki.
Patients and Data Extraction
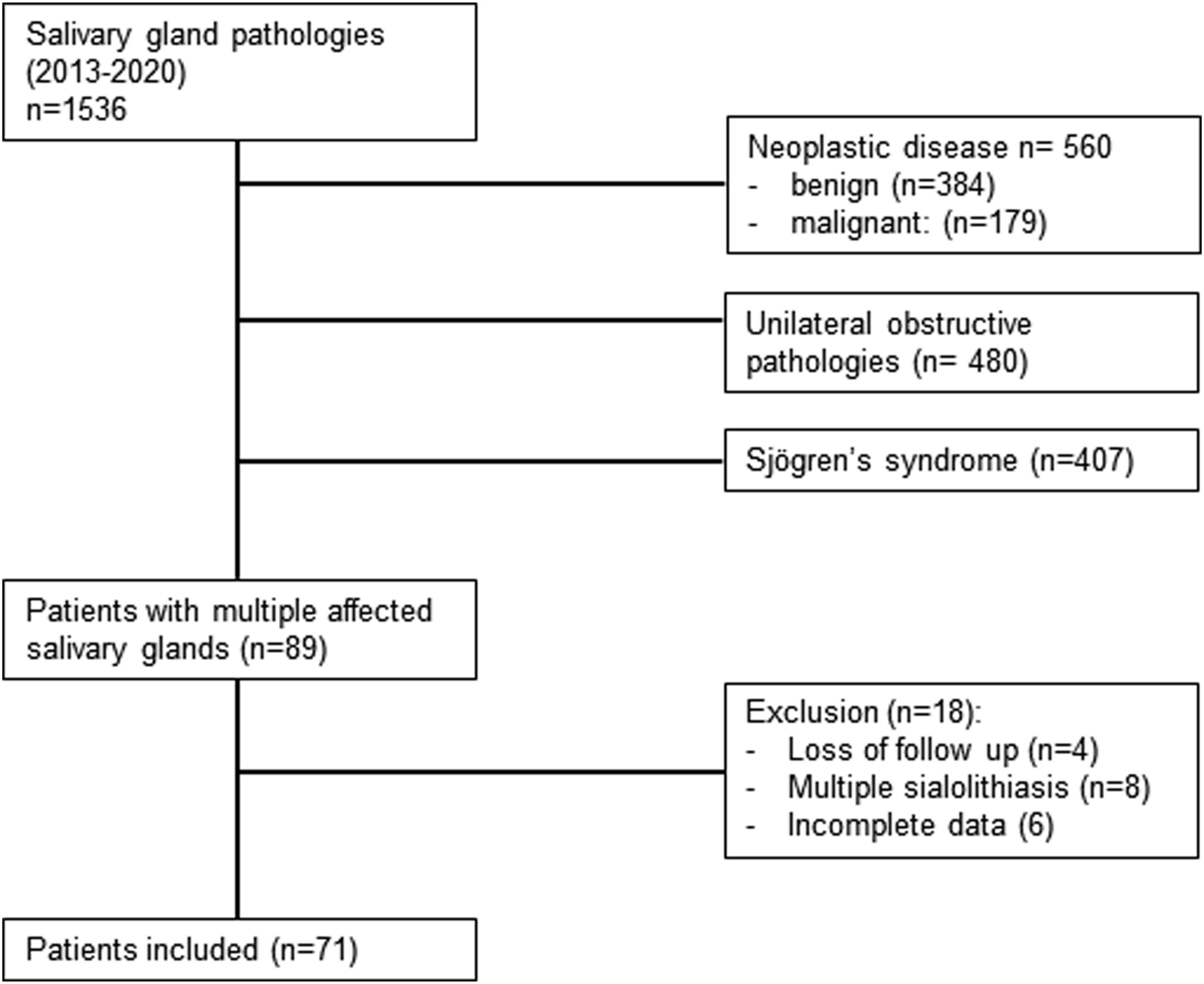
All patients treated between 2013 and 2020 in our tertiary reference center for salivary gland diseases were included in this study if at least 2 glands were affected. Patients with neoplastic lesions and multiple sialolithiasis were excluded. A minimum follow-up of 6 months was required - Ultrasonography was performed with a 10 MHz probe (GE Logiq S8 ultrasound system with a matrix linear transducer of 6-15 MHz). All examinations were performed by experienced sonographers, grading parenchymal changes (inhomogeneity, anechoic/hypoechoic areas, echogenic bands, and calcifications) as absent, minor, moderate, or severe. Any disagreement about data collection was resolved by consensus after reviewing stored videos and images of the sonography. - Blood test: These included complete blood count, C-reactive protein, serum immunoglobulins, mumps, HIV, CMV and Toxoplasmosis serology, serum amylase, autoimmune screening for Sjögren syndrome (SS-A, SS-B, Ro), and Sarcoidosis (ACE) or IgG4-associated diseases. - Sialo-MRI: Magnetic resonance sialography is a non-invasive technique that does not require salivary duct cannulation. Using a heavily T2-weighted sequence enables visualization of hyperintense saliva within the salivary duct system. This method is very effective for the detection of parenchymal and ductal alterations of the parotid glands.17,18. - Sialendoscopy: We followed the guidelines of the International Salivary Gland Society and the procedures were performed under local or general anesthesia. The salivary ducts were described according to Marchal’s lithiasis, stenosis, and dilatation (LSD) classification.19 The modular or all-in-one scope (Karl Storz, Tuttlingen, Germany) was used. All interventions were performed by the same surgeon (author UB). To irrigate, we used hydrodilation with cortisone (100 mL of saline with 125 mg of methylprednisolone). The scope itself or bougies were used to dilate any stenosis. A gastric feeding tube was used as a stent when necessary (5 Charrière). - Outcome was categorized using the subjective symptoms of the patient at the last follow-up and included the following: complete resolution (no more subjective symptoms), partial resolution (residual subjective symptoms but improved), unchanged (unchanged subjective symptoms), slightly worsened (slightly worsened subjective symptoms), and definitively worsened (requiring reintervention). Flow chart of inclusion and exclusion criteria for patients.
Data Analysis
Data were scored as numerical or categorical variables. For a synthetic presentation of data, summary statistics were calculated. Descriptive statistical analysis was performed with Prism 9.0 (GraphPad, San Diego, CA, USA).
Results
Patients and Disease Characteristics
Patient and Disease Characteristics.
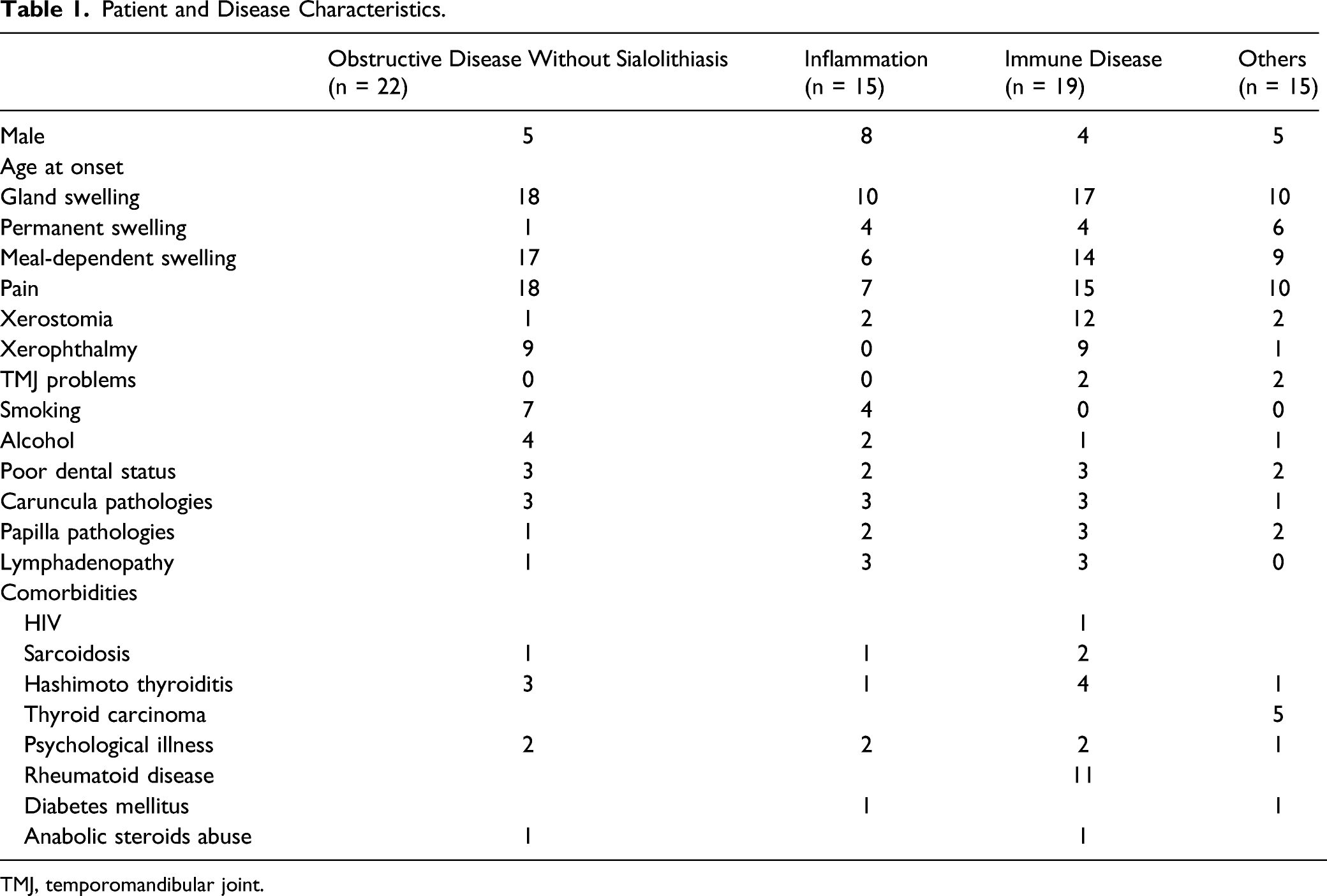
TMJ, temporomandibular joint.
Clinically, the combination of glands most affected was the following: bilateral involvement of the parotid gland (n = 57; obstructive disease without sialolithiasis: 17; inflammation: 12; immune disease: 15; others: 13). The second most significant finding was bilateral swelling of the submandibular gland (n = 22; obstructive disease without sialolithiasis: 6; inflammation: 5; immune disease: 6; others: 5).
Diagnostic Work-Up
In all cases, an ultrasound scan was performed as the first-line diagnostic intervention. In 8 cases, the salivary gland ultrasonography was normal.
Blood counts were performed in 50 patients. In 23 cases, the results of the blood test were pathological, mostly pointing to a possible underlying rheumatological disease.
Diagnostic Aspects (n = 71).
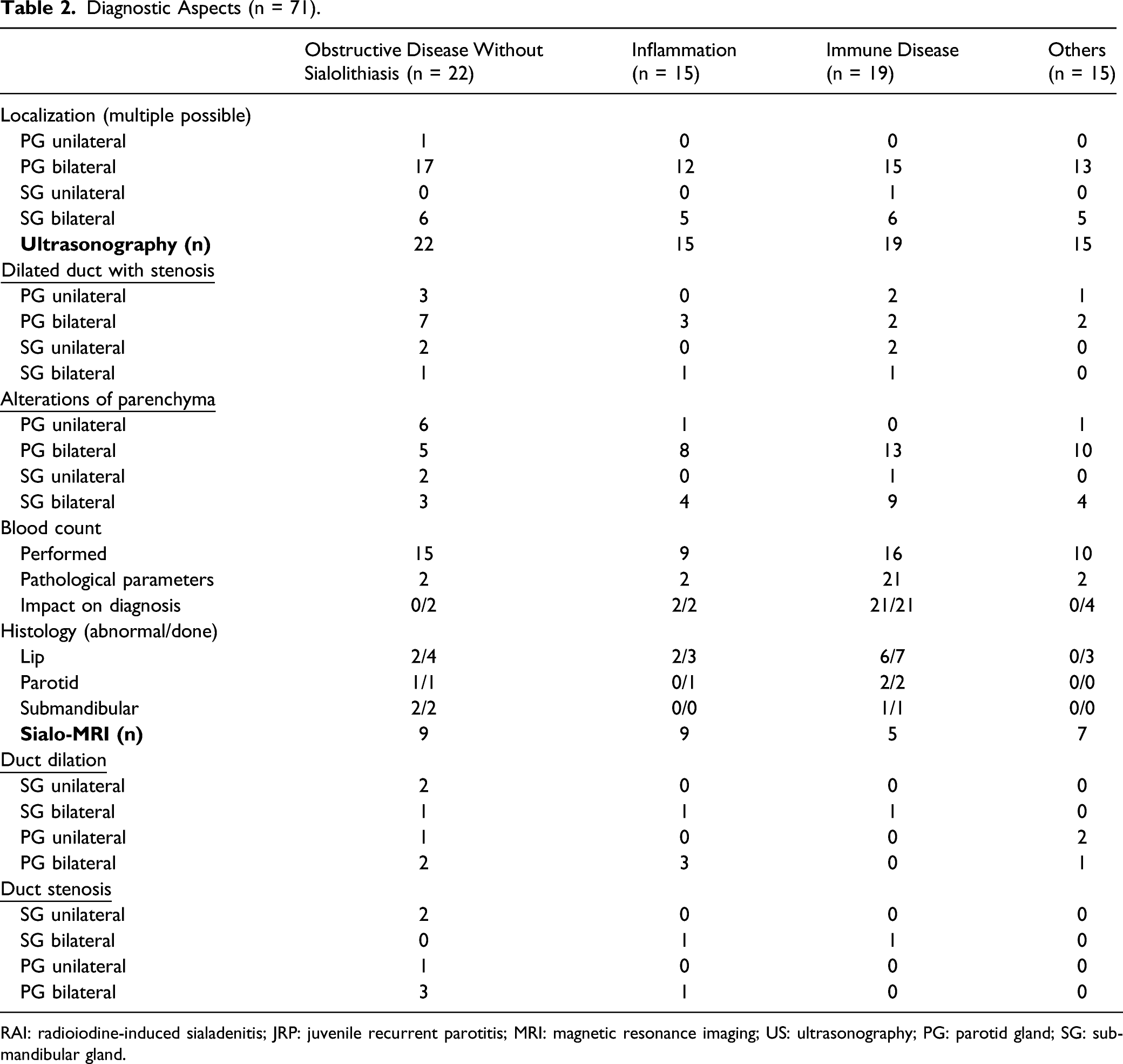
RAI: radioiodine-induced sialadenitis; JRP: juvenile recurrent parotitis; MRI: magnetic resonance imaging; US: ultrasonography; PG: parotid gland; SG: submandibular gland.
Sialendoscopic Treatment and Outcome
All patients had previously been treated by otorhinolaryngologists in private practice with conservative measures including sialagogues, a short course of NSAIDs, and antibiotics when appropriate. If the patient had only minor complaints or significant improvement after conservative treatment, no sialendoscopy was indicated. Diagnostic and therapeutic sialendoscopy was performed in 42 patients (obstructive disease without sialolithiasis: 21; inflammation: 3, immune disease: 10, RAI: 4, JRP: 4).
The indication for sialendoscopy was swelling or pain and subjective suffering of the patient. In total, 66 procedures were performed in 113 salivary glands. As therapeutic procedures, 108 glands were treated by hydrodilation with cortisone (100 mL of saline with 125 mg of methylprednisolone) during the procedures, 99 ducts were dilated, and 38 stents were inserted.
Sialendoscopy: Findings and Treatment.
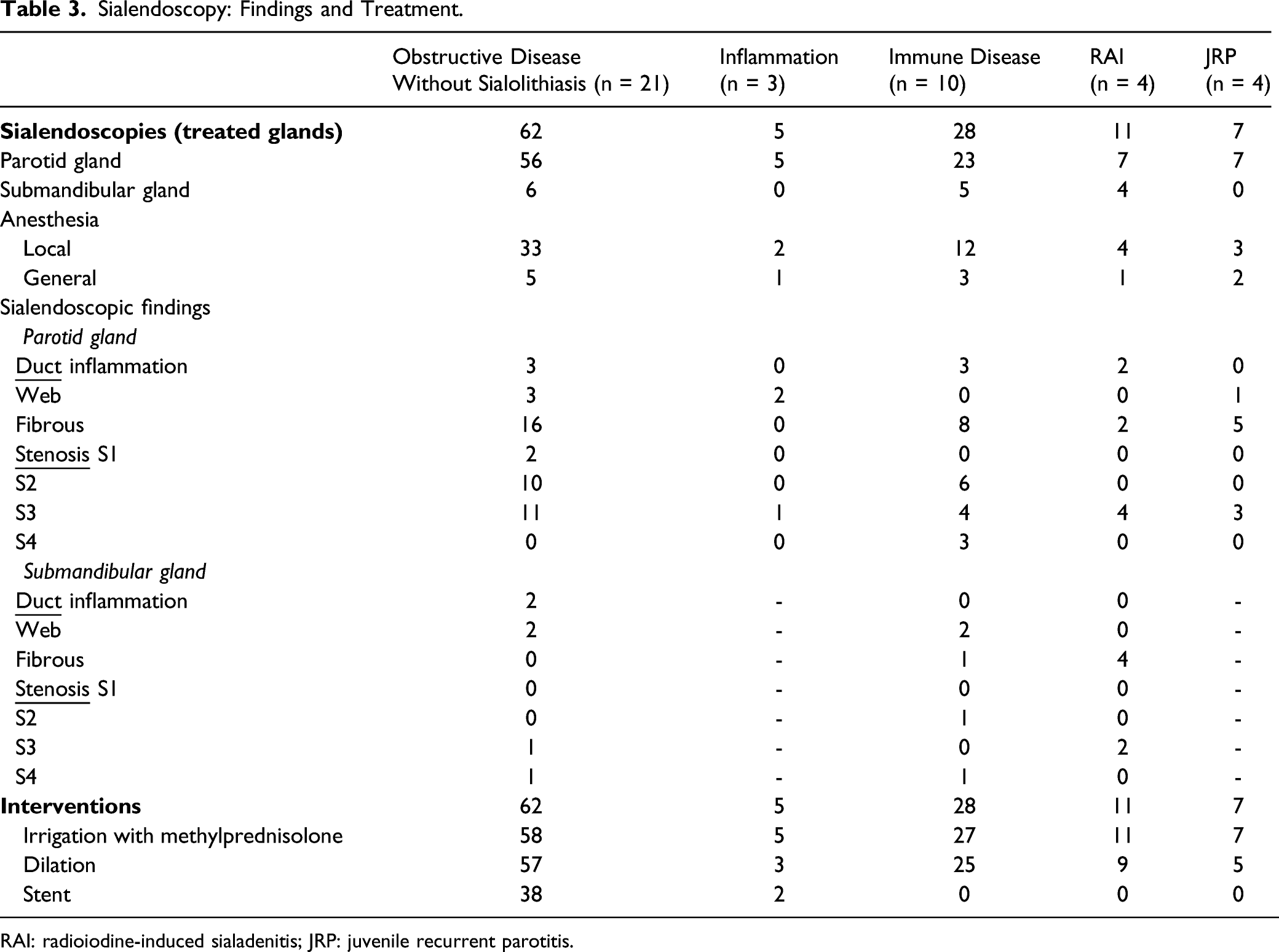
RAI: radioiodine-induced sialadenitis; JRP: juvenile recurrent parotitis.
In the “obstructive disease without sialolithiasis group,” sialendoscopies were performed in 21 patients (18 with dilation and 8 with stent insertion), of whom 13 patients had complete resolution (61.9%), 6 partial resolution (28.6%), 1 patient described no change in symptoms (4.8%), and 1 patient described slightly worsened symptoms (4.8%) postoperatively. In patients with ductal inflammation and gland inflammation, 3 sialendoscopies were performed (2 with dilation and 1 with stent). One patient described complete resolution and 2 patients had partial resolution postoperatively. In the group of autoimmune-related diseases, 10 sialendoscopies were performed (all with dilation, no stent was inserted); 7 patients described complete resolution (70%), 2 partial resolution (20%), and 1 patient had no change in symptoms postoperatively (10%). In the RAI group, 4 patients were treated with sialendoscopy (3 with dilation, no stent was inserted), 2 patients had complete resolution of symptoms (50%), 1 patient had partial resolution (25%), and 1 patient had unchanged symptoms postoperatively (25%). Regarding the 4 patients with JRP, all showed an improvement (3 with dilation, no stent was inserted).
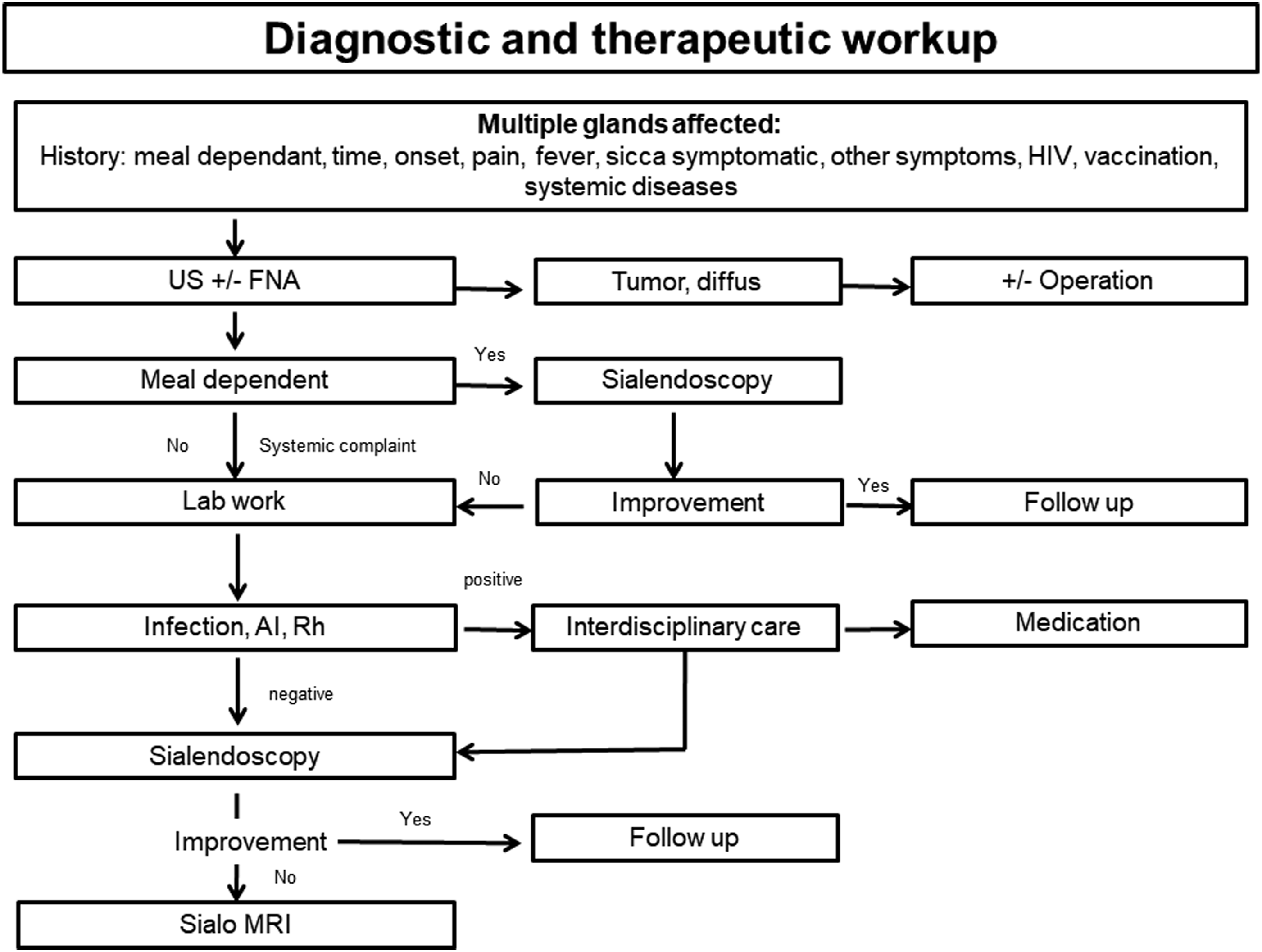
After sialendoscopy, outcomes at the last follow-up included completely (n = 27, 64.3%) or partially (n = 11, 26.2%) improved symptoms in most cases. Three patients reported unchanged symptoms and 1 patient reported progression of disease as illustrated in Figure 2. Consequently, a diagnostic workflow is proposed based on the experiences reported here and illustrated in Figure 3. The results of the treatment (JRP: juvenile recurrent parotitis; RAI: radioiodine-induced sialadenitis; results of sialendoscopic treatment: +: success, –: no effect). Diagnostic workflow (AI: auto immune; Rh: rheumatological factors; US: ultrasonography; FNA: fine needle aspiration).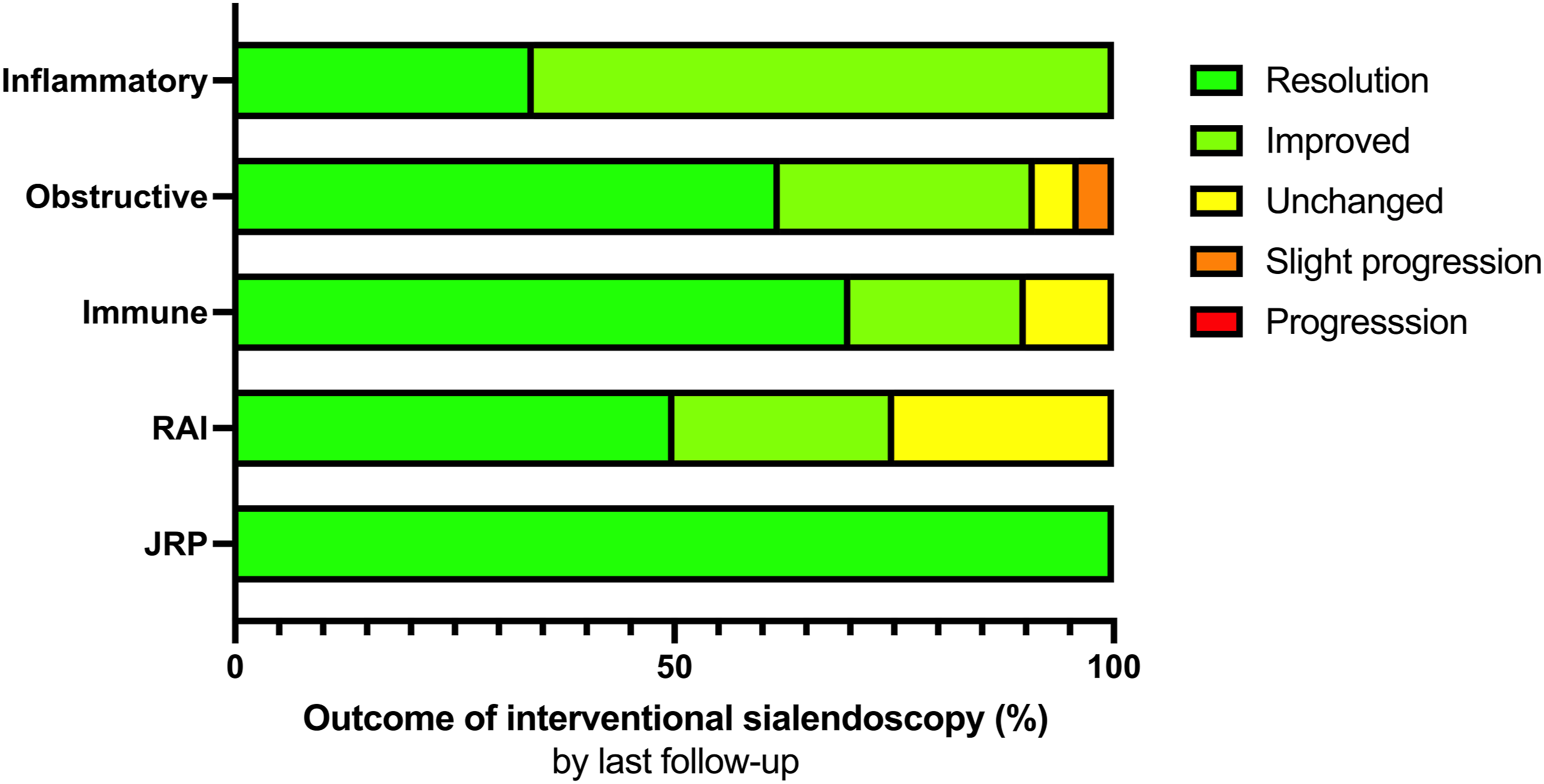
Discussion
This study investigated clinical presentation, diagnostic work-up, and therapeutic options in a retrospective cohort of patients with multiple affected salivary gland disorders. Interventional sialendoscopy was found to be a valid therapeutic option to efficiently treat disease-related complaints. Complete resolution of symptoms postoperatively was observed in 27 patients (64.3%) and partial improvement in symptoms in 11 patients (26.2%). Owing to the rarity of the disease, we did not have a control cohort and the group sizes were relatively small. As a result, no comparative statistical analysis could be performed. This is still the case. However, given the relative rarity of the disorder, our experience is encouraging, especially regarding the use of sialendoscopy.
The study cohort showed considerable heterogeneity in pathological findings. Obstructive disease without sialolithiasis was the most common finding, followed by diffuse inflammation of the gland. Underlying disease was found in only a minority of cases indicating the diagnostic challenge in these patients. Most often, the diagnosis remained descriptive. A well-known and probably very frequent diagnostic entity in the context of multiple affected salivary glands is Sjögren syndrome, a systemic autoimmune disease that affects .2-.4% of the population.20,21,22 Frequently encountered symptoms are xerostomia, xerophthalmia, pain, fatigue, and in 20-40%, systemic manifestations such as synovitis, vasculitis, and skin, lung, renal, and neurological involvement. 23 Capaccio et al. showed that interventional sialendoscopy with irrigation using steroids reduced the number of episodes of sialadenitis and oral dryness in patients with Sjögren syndrome.15,24,25 In our cohort, only a few patients with an atypical presentation of Sjögren syndrome were included. Thus, our group is subject to a considerable selection bias when assessing the incidence of Sjögren syndrome. However, since our patients responded very well to interventional sialendoscopy, our findings are consistent with the above-mentioned studies.
Moreover, it can be hypothesized that similar pathophysiological mechanisms (inflammation of the gland parenchyma and ducts as well as concomitant stenosis) may be present in patients with multiple salivary gland involvement and therefore interventional sialendoscopy remains a viable therapeutic option. In fact, treatment with radioiodine (I-131) can result in acute and chronic salivary dysfunction in 2-7% of patients.26,27 In this context, Bulut et al. reported that sialendoscopy is a clinically valuable and effective minimally invasive treatment option, especially in patients experiencing treatment-resistant xerostomia after radioiodine therapy. 28 Although limited by the small number of patients suffering from RAI in our cohort, the benefit from interventional sialendoscopy was also observable in those patients.
Regarding the diagnostic work-up, the ultrasonographic examination is the first-line procedure of choice. It offers a fast, cost-effective, and non-invasive assessment of duct stenosis with stasis from parenchymal inflammations. Moreover, concomitant imaging of all major salivary glands permits identification of all affected glands and establishes a diagnostic and therapeutic strategy. Ultrasonography allows cost-effective monitoring of the disease during follow-up.
Regarding autoimmune diseases, comprehensive analysis of blood samples usually gave important hints with referral to rheumatologists for further work-up. In all other patients, the blood examination had no diagnostic or therapeutic impact. Therefore, comprehensive analysis of blood samples should only be performed upon clinical suspicion of immune disease.
A central diagnostic element in our study cohort was the food dependence of the symptomatology. Worsening symptoms with meals indicated structural salivary stasis with congestion. In these situations, sialendoscopy is a key element in describing the extent of the disease and further characterizing pathological changes in the gland, such as sialodochitis. If sialendoscopy does not reveal relevant pathological findings or patient complaints do not improve, we suggest performing a Sialo-MRI. The rationale behind this additional imaging study is to depict further parenchymal and ductal changes. Sialo-MRI is a non-invasive technique that does not require salivary duct cannulation. Special T2-weighted sequences allow visualization of hyperintense saliva within salivary ducts. The advantage is that multiple sequential stenosis can be identified, which cannot usually be clearly visualized by ultrasound. Another advantage is that parenchymal changes can also be detected.17,29
In general, autoimmune diseases require additional interdisciplinary work-up and treatment, which are subject to international consensus guidelines. However, in most cases and especially when a definitive diagnosis cannot be established, diagnostic and interventional sialendoscopy is a viable option to improve patient complaints.
Due to the minimally invasive nature of the treatment, it can be performed under local anesthesia (84.9% of our cases) and in an outpatient setting, which has a favorable impact on the socio-economical burden of the treatment. Through sialendoscopy, the stenosis can be mechanically dilated (dilatators and balloons) and the ducts can be flushed with cortisone. In addition, stent insertion may further improve the long-term efficacy of treatment. With regard to ductal stenosis, Koch et al. reported a success rate of 80-100% for sialendoscopy with complete relief of symptoms in up to 70-90% of patients. 11 Inflammatory stenosis can be treated by irrigation with cortisone, whereas fibrous stenosis requires additional surgical treatment for dilation. Capaccio et al. confirmed the value of intraductal cortisone administration, concluding that sialendoscopy with intraductal steroid irrigation was more effective than interventional sialendoscopy alone. 30 In our study cohort with more extensive and complex disease affecting multiple glands, the outcome after sialendoscopy at the last follow-up included completely (n = 13, 61.9%) or partially (n = 6, 28.6%) improved symptoms in most cases.
In addition, we observed 15 patients with inflammatory disease of the salivary gland parenchyma. These patients typically did not complain of meal-dependent swelling. During ultrasound, the ducts were found to be of normal caliber but revealed an inflammatory and heterogeneous parenchyma. Usually, the etiology of the disease could not be further elaborated and typically symptoms were self-limiting under conservative treatment. In this subgroup, only 3 patients needed sialendoscopy, revealing a correlating sialodochitis without stenosis. One patient had complete resolution and 2 had partial resolution after hydrodilation and flushing the ducts with cortisone (100 mL of saline with 125 mg of methylprednisolone). This finding is consistent with Capaccio et al. who described interventional sialendoscopy as effective for the treatment of recurrent sine causa sialadenitis. 30
Wood et al. found that JRP is the second most common salivary gland disease in children after mumps.31,32 According to Leerdam et al., a blood test should be performed to detect any viral or bacterial infections and to exclude mumps or other possible associations such as HIV, Sjögren syndrome, or general immunodeficiency. 33 Interventional sialendoscopy has an important therapeutic benefit of reducing the number of recurrences of acute episodes of parotitis, thus giving patients a better quality of life until puberty, when the disease is usually self-limiting. In our cohort, we treated 4 patients by sialendoscopy, dilation, and cortisone flushing. All patients obtained a reduction in the number of acute episodes of parotitis. Two of them experienced a recurrence of symptoms after a mean follow-up of 20 months. However, the episodes were less severe and less frequent until the end of follow-up.
Our study is limited by its retrospective design and the relative rarity of the disease. Therefore, the heterogeneity of the cohort resulted in smaller subgroups. However, all patients had multiple affections of the salivary glands in common and interventional sialendoscopy showed satisfactory efficacy despite the lack of a definitive diagnosis. Another limitation of our study is that the outcome after therapy was not controlled with a standardized questionnaire. To ensure comparability of the results, all follow-up examinations have been performed by the same investigator focusing on patient-reported complaints with patient-reported outcome measures (PROMS).
Conclusions
Multiple affected salivary gland diseases are diagnostically challenging and patients show considerable heterogeneity with respect to the etiology of the disease. However, interventional sialendoscopy offers an effective and safe therapeutic option and should be considered in all patients with a sufficiently high disease-related disorder.
Footnotes
Author’s contribution
UB, MR, CA, and LA had the original idea, designed the study, and wrote the first draft of the article. UB and LA performed the analysis, provided input to the study design, and wrote sections of the paper. UB, MR, JK, EP, MC, MvW, and LA helped to interpret the results and wrote sections of the paper. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. UB is the guarantor.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Ethics
Approval to perform this study was obtained from our Institutional Review Board (Kantonale Ethikkommission Bern, KEK-Nr. 2020-01483). The study was performed according to the Declaration of Helsinki. Formal written informed consent is not required for this type of retrospective study and was waived by the local ethics committee.
Availability of Data and Material (Data Transparency)
Available via the corresponding author
Code Availability (Software Application or Custom Code)
Available via the corresponding author