
Abstract
Introduction:
Sialolithiasis is the most common cause of symptomatic obstructive sialadenitis. Sialendoscopy represent a minimally invasive technique that has evolved significantly in the last 2 decades, with high success rates in managing sialolithiasis and allowing gland preservation. Lithotripsy assisted or not by laser represents the fragmentation of stone or lithiasis within the salivary duct followed immediately by removal of the fragmented pieces.
Results:
Sixteen papers meet inclusion criteria. The mean maximum diameter of lithiasis was 7.11 mm (min: 2 mm/max: 17 mm; standard deviation [SD]: 2.33; 95% CI = 1.573-4.463). Success rate described ranging from 71% to 100% with a mean of 87.3% (SD: 7.21; 95% CI: 5.326-11.158) and the gland preservation rate was 97%. Considering only “non retrievable–non floating stones” studies that include both parotid and submandibular stones: Eight clinical retrospectives, nonrandomized studies and 1 prospective, nonrandomized study report results from parotid and submandibular gland lithiasis. According to this, the most common gland involved was the submandibular gland (n = 153; 65.1%), in comparison to the parotid gland (n = 82; 34.8%).
Conclusion:
The current evidence supports LAS as a conservative, efficient, safe, and gland-preserving alternative technique, in experienced hands, for management of mid-size sialolith removal from major salivary glands, when the indication is appropriate.
Introduction
Sialolithiasis is the most common cause of symptomatic obstructive sialadenitis, accounting for more than 50% of all symptomatic cases. 1 -3 Sialolithiasis more often affect the submandibular gland (80%-90%) than the parotid (5%-10%). 4 This phenomenon can be hypothetically related to the long, tortuous upward path of the Wharton duct, the thicker consistency of submandibular saliva that is rich in phosphorous and has a high pH; factors that make the submandibular gland more conducive to stone formation. 5
Symptomatic sialolithiasis has been traditionally been managed with a range of therapeutic options. The paradigm has shifted now where in most scenarios, gland preservation is the primarily goal that has been afforded by minimally invasive techniques. 6 -8 Sialendoscopy is one of this minimally invasive technique that has evolved significantly in the last 2 decades, both in terms of the technology and technique, allowing sialendoscopist to achieve high success rates (>80%) in managing sialolithiasis and allowing gland preservation. 9
However, the ability to remove a salivary stone by pure endoscopic techniques depends on a variety of different factors that influence surgical access and visualization of the salivary stone within the duct such as the mobility of the stone, presence or absence of stenosis proximal to the stone, stone size, shape and orientation, location (ductal, hilar, or intraglandular), and composition (hard or soft). 9 Also, decisions about the salivary gland therapeutic in these cases can be supported by the lithiasis, stenosis and dilatation (LSD) classification develop by the European Sialendoscopy Training Center. 10 Usually, complete endoscopic removal with endoscopic forceps or stone baskets is more often successful with completely visible and floating stones, measuring usually less than 4 mm in their width. 11 Larger, immobile or impacted, or not completely visible stones offer challenges for pure endoscopic extraction and it becomes necessary to use other techniques such as intraductal laser-assisted lithotripsy, intraductal pneumatic lithotripsy, or combined techniques to successfully remove these stones. 12
Lithotripsy represents the fragmentation of stone or lithiasis within the salivary duct followed immediately by removal of the fragmented pieces. There are several types of lithotripsy depending on the energy used (piezoelectric, electromagnetic, electrohydraulic, pneumatic, or laser) and the approach (extracorporeal and intracorporeal). 13 Endoscopic laser lithotripsy in salivary glands was first described in the early 1990s, 14,15 when Gundlach et al using a pulsed excimer laser with a pulse width of 60 ns and a wavelength of 308 or 351 nm report their preliminary experience. In their series, 11 of 12 cases with submandibular gland sialolithiasis were successfully treated. After this, many case series have been published on the use of different lasers and their success rates of managing complicated intermediate-sized lithiasis. Today, use of laser for management of sialolithiasis (mostly intermediate-sized ie, 5-7 mm) is controversial with mixed result and varying opinions within the sialendoscopy community. While the advantages of laser lithotripsy are apparent, that is, stone fragmentation and avoidance of a transoral incision and dissection or external gland surgery; the concerns raised have surrounded the concerns for retained fragments, ductal trauma, and caused by heat generation and attempted basket retrieval of small pieces.
Current evidence and clinical experience has conclusive proven that sialendoscopy is a valuable tool that facilitate complete stone removal and symptom resolution in patients suffering from obstructive sialadenitis. However, the results of interventional sialendoscopy when it pertains to purely endoscopic stone removal is variable; since the possibility of sialolith removal depends on technical and human factors, and these can be related to the type of pathologic disorder, surgeon experience, or the set of instruments used. This explains why, intraductal lithotripsy laser-assisted lithotripsy with sialendoscopy (LAS) has gained attention in the last 2 decades as LAS makes it possible, in some cases, to overcome the limitations of traditional sialendoscopy for the management of mid to larger-sized salivary stones. 9 Consequently, the aim of this review was to analyze the current literature on the role of LAS in the treatment of major salivary gland lithiasis and provide an evidence-based perspective on clinical outcomes related to LAS.
Methods
The criteria for inclusion of studies for this systematic review were based on the population, intervention, comparison, outcome, timing, and setting framework. 16 The review was conducted with regard to the Preferred Reporting Items for Systematic Reviews and Meta-analyses checklist 17 and a formal protocol was presented in the International Prospective Register of Systematic Reviews (PROSPERO) according to the National Institute for Health Research (NIHR) (No. 149254). Heterogeneity among studies included due to the type of laser and absence of randomization limited ability to combine data statistically into a formal meta-analysis.
Types of Studies
Authors considered prospective, retrospective, case-series, controlled, or uncontrolled studies investigating the role of laser-assisted lithotripsy combined trough a sialendoscopic approach. Studies had to be published in English, German, Spanish, or French in peer-reviewed journals. Only studies reporting data for 10 patients at least were considered for inclusion. We also have considered basic science research for understanding the principles of laser lithotripsy.
Participants, inclusion/exclusion criteria
Publications were considered for analysis if they reported results of at least 10 adult patients treated by obstructive salivary gland disease through LAS approach. Also, studies need to describe the type of laser device used, type of gland affected, mean stone size, outcome, complications, salivary gland preservation.
Intervention and comparison
This study investigated the role of laser-assisted lithotripsy combined trough a sialendoscopic approach in the treatment of obstructive salivary gland disease.
Outcomes
The primary outcome evaluated in this study was symptom resolution after LAS, a secondary outcome was the salivary gland preservation.
Timing
The minimum median follow-up time considered was 3 months after surgery to evaluate symptom resolution.
Setting
Surgical hospital studies.
Search Strategy
The PubMed, Google Scholar, and Scopus search was conducted by 2 independent authors (C.M.C.-E. and C.S.-G.) to identifying articles published within the past 30 years (1990-2020) that included the use of LAS. Studies were screened if they had available full texts. The following keywords were used, “sialendoscopy,” “salivary gland,” “laser-assisted,” “lithotripsy,” “holmium-YAG,” “carbon-dioxide laser,” and “combined.”
Assessment of Quality
The evidence quality of identified studies was appraised using the Oxford Center for Evidence-Based Medicine Levels of Evidence. 18 According to this, prospective or retrospective studies with A or B grading were included. Also, we included a summary of bias analysis of the studies about LAS that were included in the systematic review, according to the Tool to Assess the Risk of Bias in Cohort Studies developed by the Clarity Group and Evidence Partner. 19 And for case-series we use the Quality Assessment of case series studies checklist from National Institute for Health and Clinical Excellence. 20
Results
The electronic search identified 396 papers, of which 16 papers met the inclusion criteria (Figure 1, Table 1). 14,21 -35 Among the included articles, 11 are clinical retrospective, nonrandomized, uncontrolled studies, 22,24,26 -35 and 5 prospective nonrandomized studies. 14,21,23,25,27 Eleven papers investigated the use of Holmium: Yttrium-aluminum-garnet (YAG) laser while 2 papers investigated the use of pulsed dye laser. One study explored the use of and CO2 laser, diode laser, thulium:YAG, erbium:YAG, and pulsed excimer, respectively. The study characteristics are summarized in Table 1.
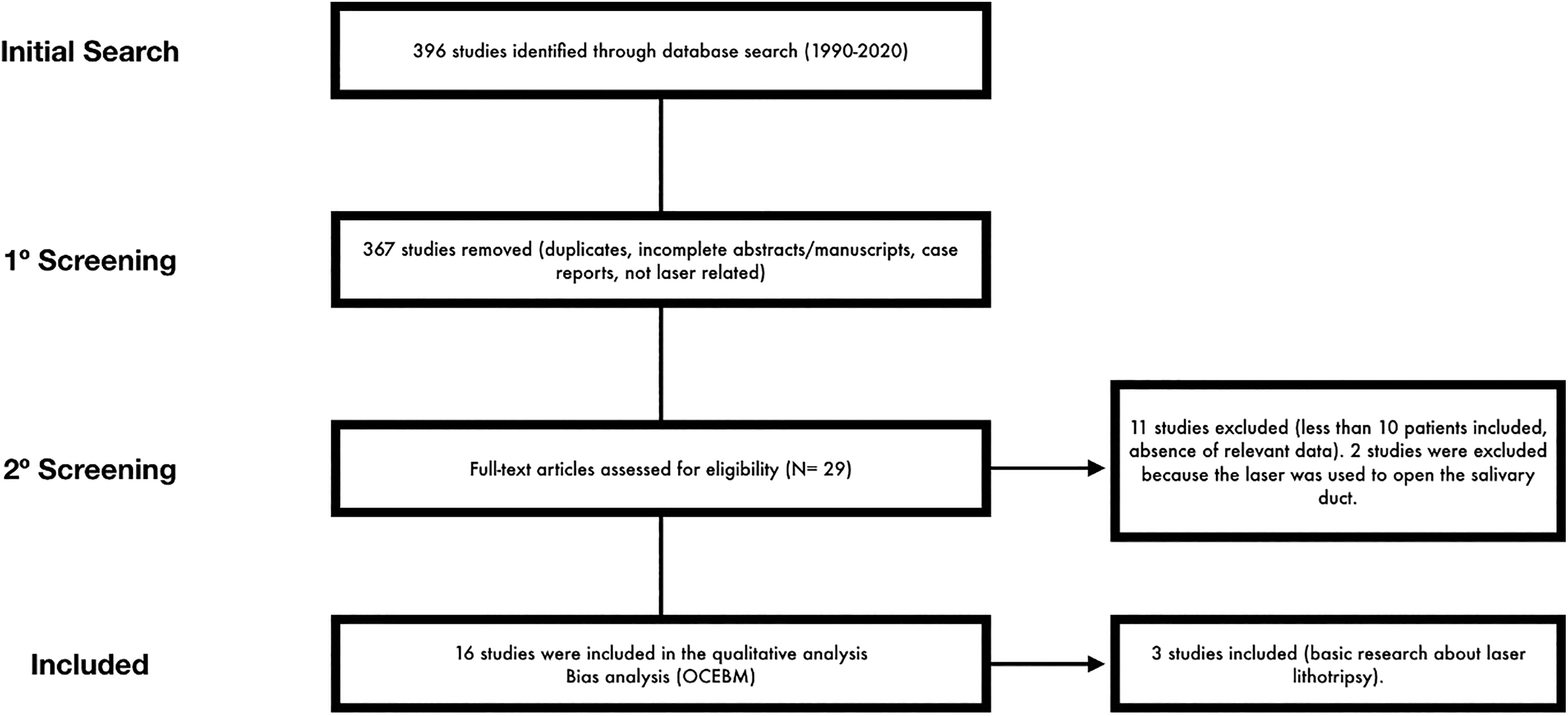
Algorithm of study selection.
Studies Investigating the Role of Laser-Assisted Lithotripsy With Sialendoscopy in the Treatment of Major Salivary Gland Lithiasis.
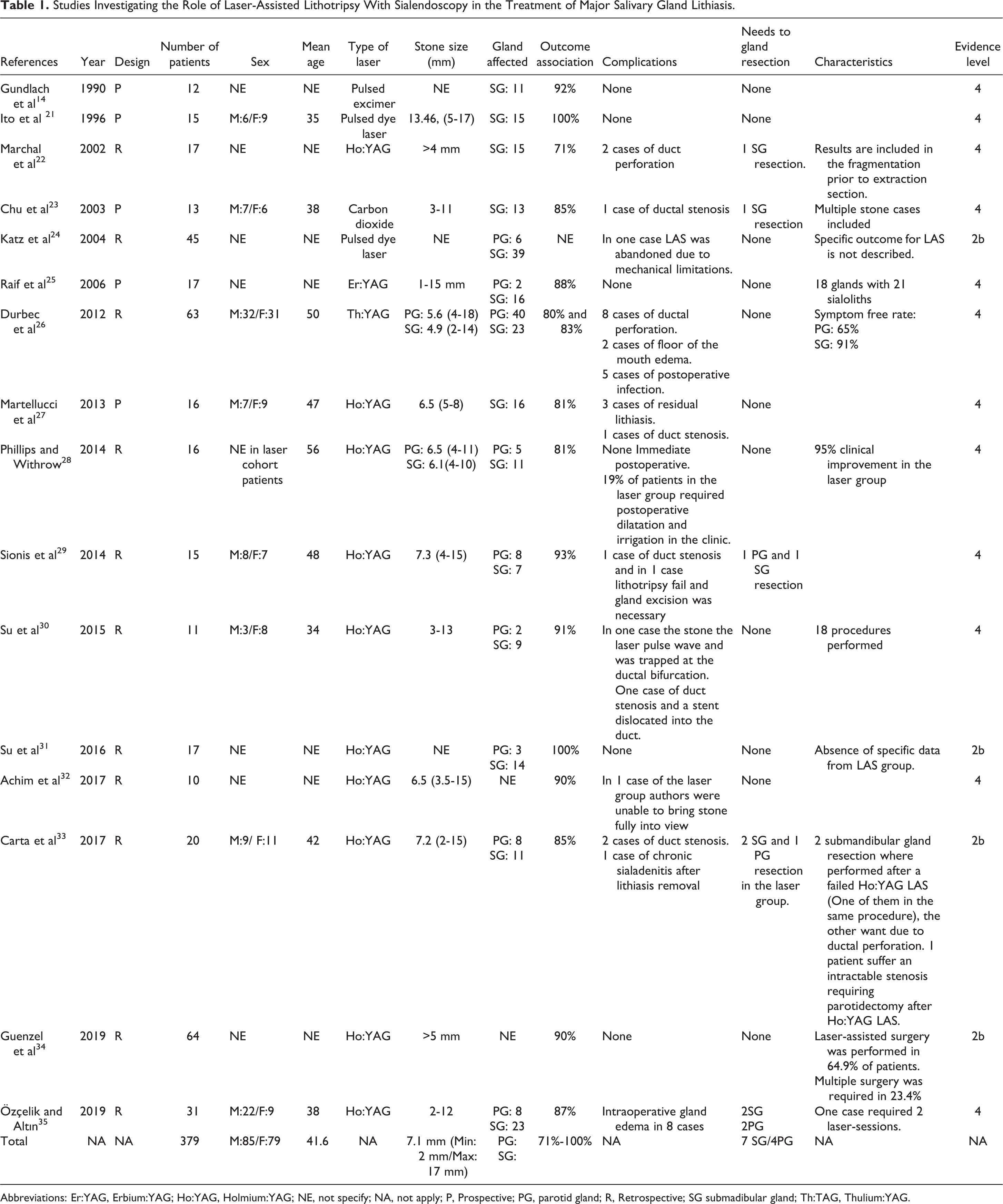
Abbreviations: Er:YAG, Erbium:YAG; Ho:YAG, Holmium:YAG; NE, not specify; NA, not apply; P, Prospective; PG, parotid gland; R, Retrospective; SG submadibular gland; Th:TAG, Thulium:YAG.
Type of Gland Affected
Eight clinical retrospectives, nonrandomized studies 24,26,28 -31,34,35 and 1 prospective, nonrandomized study 25 report results from parotid and submandibular gland lithiasis. According to this, the most common gland involved was the submandibular gland (n = 153; 65.1%), in comparison to the parotid gland (n = 82; 34.8%). In 4 prospective nonrandomized studies 14,21,23,27 and 1 retrospective 18 nonrandomized study, only patients with submandibular salivary gland lithiasis were included. Two retrospective, nonrandomized studies do not report the number and type of glands affected (Table 1).
Sialolith Size and Shape
When combining data from 5 clinical, retrospective, nonrandomized, uncontrolled studies (4EL: 4 and 1 EL:2b) 26,28,29,32,33 and 2 prospective nonrandomized study 21,27 (EL: 4), the mean maximum diameter of lithiasis is 7.11 mm (min: 2 mm/max: 17 mm; standard deviation [SD]: 2.33; 95% CI = 1.573-4.463). All of them correspond to endoscopically unremovable lithiasis. There was no specific data about stone shape (Table 1).
Surgical Outcomes and Gland Preservation Rate
Eleven clinical retrospective, nonrandomized, uncontrolled studies 22,25,26 -35 and 5 prospective nonrandomized studies 14,21,23,25,27 reported a high success rate ranging from 71% to 100% with a mean of 87.3% (SD: 7.21; 95% CI: 5.326-11.158). The gland preservation rate was 97%. Furthermore, sialadenectomy after LAS failure was performed in 11 patients in total (2.5%), corresponding to 7 (1.8%) submandibular gland resection and 4 (1%) parotid gland resection (Table 1).
Complications
All the studies included report the presence or absence of complications. 14,21 -25,26 -35 From the 379 patients included, 11 (2.9%) had a duct perforation, 9 (2.3%) had postoperative submandibular gland edema, 5 (1.3%) from a postoperative duct stenosis, 5 (1.3%) developed a postoperative infection, 3 (0.7%) had a residual lithiasis, 2 (0.5%) patients suffer a floor of the mouth edema, and 1 case needed to be abandoned due to mechanical limitations. There were no ranulas reported (Table 1).
Quality of Studies Included
Quality and risk of bias of studies included are summarized and described in Tables 2 and 3.
Analysis of LAS Treatment According to Population, Assessment of Exposure, Outcome of Interest at Start of Study, E/U and Outcome of Interest, Assessment of Prognostic Factors, Assessment of Outcome, Adequate Follow-Up Cohort, Cointervention as Described in Material and Methods and the Tool to Assess the Risk of Bias in Cohort Studies Developed by the Clarity Group and Evidence Partners.
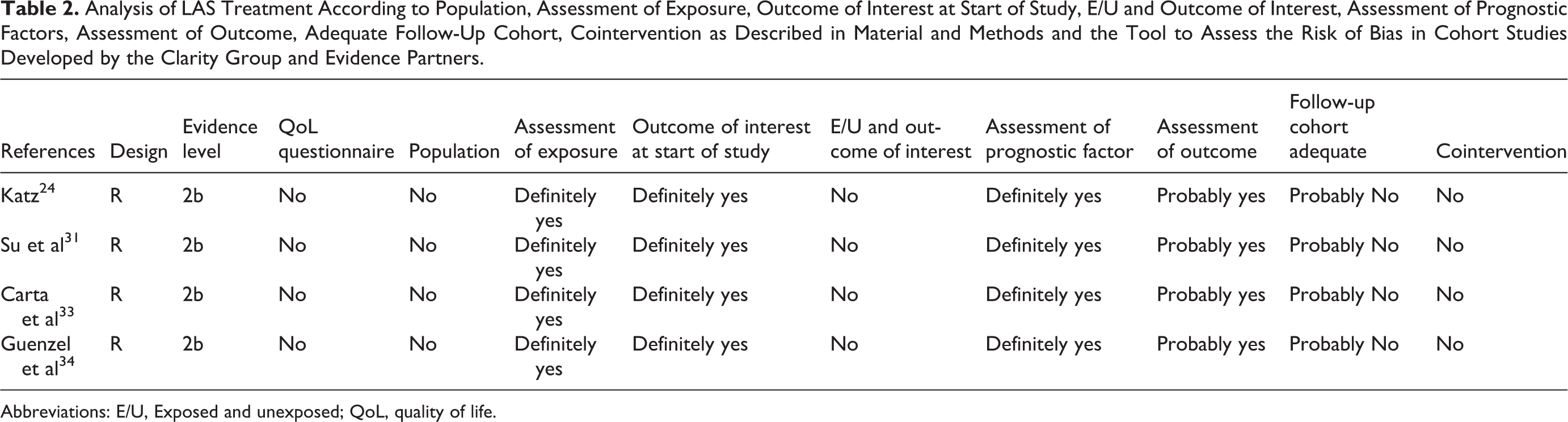
Abbreviations: E/U, Exposed and unexposed; QoL, quality of life.
Analysis of LAS Treatment According to the Quality Assessment of Case Series Studies Checklist From National Institute for Health and Clinical Excellence.
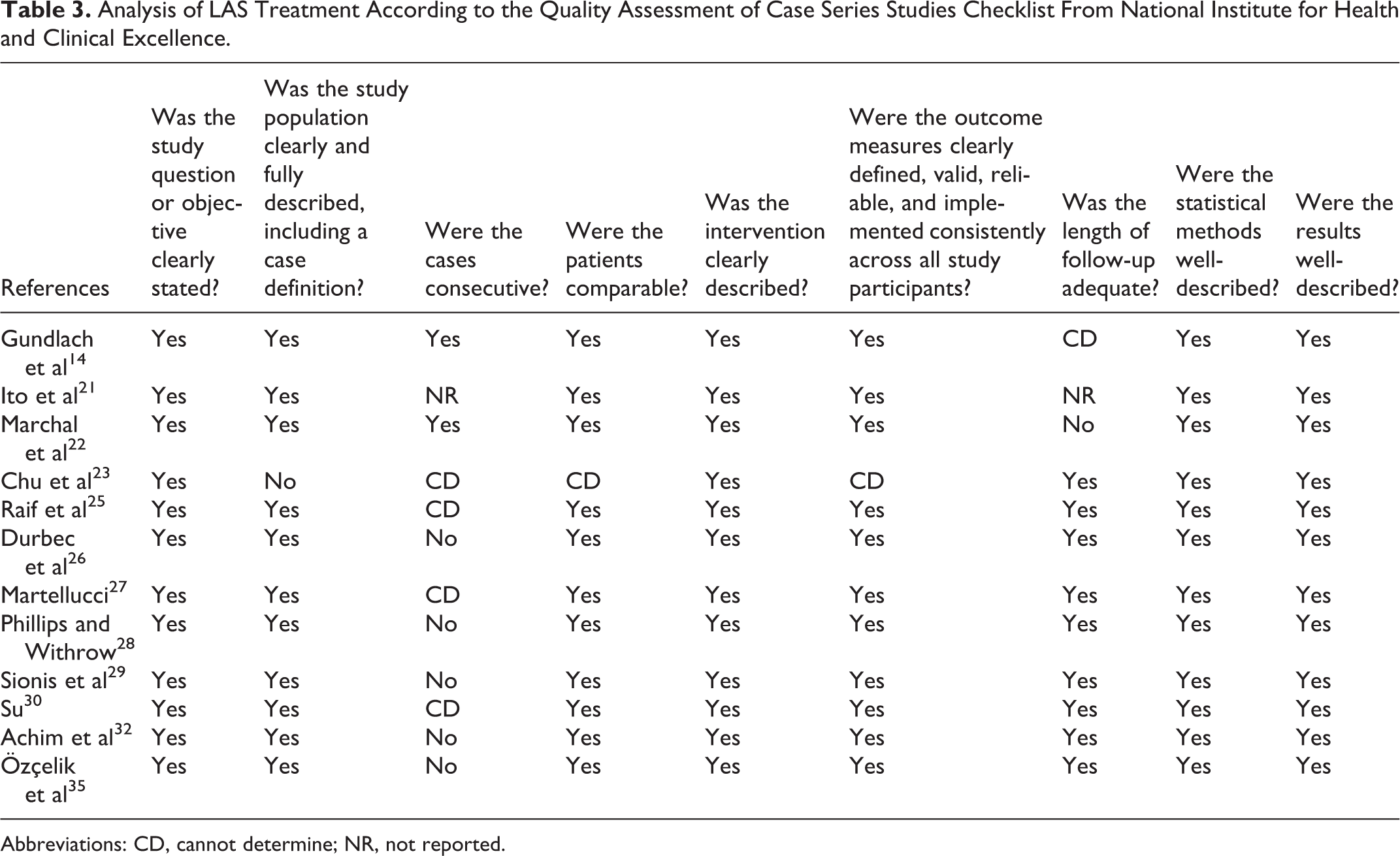
Abbreviations: CD, cannot determine; NR, not reported.
Discussion
To understand the advantages and limitation of laser lithotripsy, it is also important to understand the basic principles of laser energy and how they impact the salivary duct and its lumen—since the ductal lumen is our surgical field and access for intervention. To produce laser light, electrons of a particular substance or element have to be stimulated by an external source and raised to a higher energy level. There is an amplification of monochromatic, coherent light waves. 36 -38 Different amplification medium are described, and these can be a gas (CO2, excimer, argon), liquid (fluorescent alcoholic solutions, dyes), or solid (Neodymium:YAG [Nd:YAG], thulium:YAG [Th:TAG], holmium:YAG [Ho:YAG], erbium:YAG [Er:YAG], and chrysoberyl [alexandrite]), which can be stimulated to photon emission.
In 1963, Mulvaney postulated the principles for laser lithotripsy for urology. According to this, the laser pulse absorption causes plasma formation on the surface of the calculus, and the plasma rapidly expands a cavity of ions and electrons that collapses rapidly after the laser pulse. This action produces a mechanical shock wave. The saline solution used for irrigation confines the shock wave and concentrates its effect on the stone. This effect elevates the pressure created by shock waves under the stone, causing calculus fragmentation. That is how the efficiency of fragmentation was described by the efficiency of conversion from photonic energy to mechanical energies causing stone disintegration. Furthermore, absorption properties depend significantly on the material used and wavelengths. Laser wavelength can oscillate between 300 and 980 nm and due to the high absorption rate of typical human calculus, a shock wave can be generated by the process described previously, with moderate energy (20-100 mJ) and impulse duration in the microsecond range. 39
To translate this principle into the surgical field, a combination of wavelength, pulse duration, frequency, pulse energy, and fiber diameter will be essential to determine the size of the fragments produced by the laser. 40 This multiple shock waves phenomenon is responsible of generating fissures and promote the rapid crumbling of the stone. However, during surgery, just about 60% of the generated shock wave energy actually penetrates the stone, causing an effective fragmentation. The remaining 40% is partially reflected at the surface of the stone or causes adverse thermal effects in the surrounding tissue. 39 Hence, it is important for the surgeon to consider the energy settings and time that will be needed to fragment and extract salivary stones fragments since surgical access to the stone surface for LAS will be impacted by ensuing ductal edema due to thermal effects and further compounded by technical and human factors earlier described that impact successful endoscopic stone removal.
In the surgical setting, various lasers have been tasted for intracorporeal lithotripsy. An essential common condition among them is the small diameters of fibers (surrounding 200-250 microns). Also, the fiber flexibility allows surgeons to use it through flexible endoscopes, applying high-watt intensities for fragmentation of stones even in the periphery of the duct system or behind stenotic areas. According to data reviewed, the most common laser device used was the Ho:YAG, considered by most authors as the first choice due to the color absorption by stones and the cost-effectiveness of the method due to the availability in most hospitals within their urologic departments.
As we mentioned above, the submandibular gland is more commonly affected by sialoliths than the parotid gland. 5 Although our review confirms this tendency, differences are less significant. Considering only “nonretrievable–nonfloating stones” studies that include both parotid and submandibular stones, the submandibular gland was affected in 65.1% and the parotid gland was affected in 34.8% of the cases. Another relevant factor was the sialolith size. The mean diameter of stones is 7.11 mm. However, lithiasis size is very heterogeneous among studies (min: 2 mm/max: 17 mm). Several authors have reported standard treatment algorithms for sialolithiasis. They generally show a consensus that small, mobile stones with diameters of 3 to 4 mm or less can typically be removed via simple basket extraction. In contrast, larger, impacted stones with diameters greater than 8 mm are generally treated with combined endoscopic and transoral/transfacial approaches. 41 For midsized stones between 4 and 8 mm, the best means for treatment is more variable. Looking for evidence in order to establish a cohort value about the ideal size to perform a LAS, Marchal and Dulguerov recommended that stones larger than 4 mm in the submandibular duct or 3 mm in the parotid duct undergo fragmentation before an attempt to retrieval. Guenzel et al recommend LAS in stones larger than 5 mm 34 and Walvekar et al suggested similar recommendations with regard to size and added that the shape and orientation of the sialolith are also predictive of the success of endoscopic extraction. 42 According to the principle of action of LAS, we can hypothesize that the shape of the sialolith is relevant when we consider this kind of approach. Across the literature, different shapes have been described: oval, round, or irregular with different rates of success for removal (oval and round 76% vs irregular 22%). 9 However, no data about shape were found in the studies included in this review, being impossible to summarize enough evidence to prove it.
The advantages of a successful LAS and complete stone removal are avoidance of transoral incision or external approach for gland removal and possibly faster recovery and less discomfort as opposed to the more invasive alternatives mentioned earlier. However, it is important to consider the disadvantages of LAS that are unique to this technology and more frequent complications associated with it. From the beginning, some of the lasers used for lithotripsy of salivary stones showed a high risk of tissue damage (perforations of the duct, secondary stenosis, development of abscesses requiring gland removal) 15,21,25 possibly related to the high temperature inside the salivary duct. Durbec et al described a ductal wall perforation in up to 13% of the cases. 26 Luers et al tested a diode laser fiber of 980 nm and found that the temperature next to the salivary stone increased to around 30 °C during the active lithotripsy. Nonetheless, with continuous rinsing and keeping a distance of 2 mm, the temperature around the laser fiber tip was reduced by about 50% with relatively limited damage to the surrounding tissue. 43
Vision reduction during the surgical procedure by floating fragments has been described too. Those fragments interrupt the case until irrigation is performed, and baskets or forceps need to be used to remove the fragments. Hence, LAS can become time consuming mainly because of the frequent interruptions and the precautions needed to avoid tissue damage. Also, another disadvantage of lasers is the high cost of equipment which is a barrier to widespread use of this technique. Considering the availability of Ho:YAG in many urological departments, the costs can be limited by using the laser already available within the hospital setting.
Some factors related to time-consumption of LAS have been described like the learning curve associated with initially implementing sialendoscopy techniques, lithiasis size (>7-8 mm), a steadily improving optimization of laser settings, case selection, and operative technique. 28 A factor that may not have been considered, that could impact times for LAS is the type of laser. A more specific example is the Er:YAG laser; this laser is not transmitted through a fiber rather a hollow guide of 1 mm diameter is required. However, the fragments produced are smaller than most other lasers affording clearance using irrigation. We can overcome the problems with fragment size and laser manipulation if we continue to explore for the most optimal laser energy for LAS and salivary stone fragmentation. 25
Finally, the limitations of our study need to be addressed. In the absence of randomized studies comparing LAS against other lithotripsy techniques, it is impossible to establish proper comparisons or perform a meta-analysis. Our review is also limited by the heterogeneity of the included studies regarding lithiasis size, instrumentation and surgical expertise, and by the exclusion of studies due to the lack of relevant data. 44 A cost-related analysis of LAS in comparison with other techniques was not possible due to the absence of data. Our literature review found several gaps in data and inconsistencies in reporting data across studies; consequently, we propose that to better understand the role of LAS in the management of sialolithiasis, a multicenter prospective randomized study that can compare different types of intraductal lithotripsy (laser vs pneumatic), intraductal versus external, also comparing different type of lasers. While evaluating technical and clinical results is vital, these studies should also strive to capture information on symptom score and the quality of life of patients before and after each procedure using tools such as Chronic Obstructive Sialadenitis Symptoms (COSS) questionnaire (UCSF article by Will Ryan and Jolie Chang), in order to establish best practice recommendations, according to the different options available.
Conclusion
In summary, this study suggests that LAS can be a conservative, efficient, safe, and gland-preserving alternative technique, in experienced hands, for management of midsize sialolith removal from major salivary glands, when the indication is appropriate. However, due to the low evidence level, additional prospective-randomized trials are needed to determine the definitive role of this technique in the management of obstructive salivary gland disorders and make stronger and more precise recommendations for use of laser technology for management of not only larger stones but also other obstructive pathology such ductal stenosis. Also, if these results can be translated into improved surgical safety and improved patient satisfaction.
Footnotes
Authors’ Note
Informed consent for the use of medical images was obtained from patients included.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.