
Abstract
Smoking is known to increase laryngeal inflammation and laryngopharyngeal reflux (LPR), which cause laryngeal irritation. Thus, the aim of this study is to evaluate the changes in the symptoms and the findings of laryngeal irritation in smokers after a smoking cessation period. The reflux symptom index (RSI) and the reflux finding score (RFS) were used for evaluating the symptoms and findings of laryngeal irritation in smokers. Endoscopic examination of the laryngeal structures for RFS and symptom inquiry for RSI were performed at the beginning of the study and after a 2 months of cigarette cessation period. This study was carried out in 24 volunteers (14 female and 10 male), between the ages of 24 and 62 years. When we compared the results of RSI and RFS that were performed before and after the cigarette cession period, we found that there was a significant improvement both in RSI and in RFS (P < .001 and P < .001, respectively). Also, there was significant correlation between the cigarette smoking period and RFS score that was determined at the beginning of the study (P = .006, r = .54). A significant improvement was found both in RSI and in RFS after smoking cessation period, which might be the evidence of improvement in laryngeal irritation possibly caused by inflammation due to smoking and LPR. A significant positive correlation was found between smoking period and RFS, especially with vocal fold edema and posterior commissure hypertrophy.
Introduction
Smoking is an important public health problem and a very common habit. Smoking is associated with cardiovascular diseases, respiratory diseases, and, especially, cancers. 1 -4 The most effective method of getting rid of the morbidity and mortality is to quit smoking. 5,6
Chronic laryngeal inflammation, which causes the symptoms of laryngeal irritation, is commonly attributed to smoking, reflux, allergies, vocal abuse, or a combination of these factors. 7,8 There were many articles about the toxic effects of smoking on respiratory tract mucosa in the literature. 7 -9 Also, smoking is known to increase the laryngopharyngeal reflux (LPR). 10 However, there was a lack of data about the effect of smoking cessation on laryngeal irritation.
Reflux symptom index (RSI) was a questionnaire that was validated for LPR and found reliable on examining the effect of treatment modalities on LPR. 11 -14 Reflux finding score (RFS) was a laryngopharyngeal endoscopic scoring system that was also validated for LPR and widely used in the literature for evaluating the effect of treatment modalities for LPR. 11 -14 However, RSI and RFS were all subjective scoring systems, and recent literature found these tests unreliable for evaluating LPR without an objective pH monitorization. 15 When the content of the RSI and RFS scoring systems were evaluated, it was seen that these scoring systems were suitable for investigating the laryngeal irritation symptoms and the inflammation of laryngeal mucosa. Therefore, the aim of this study is to evaluate the changes in the symptoms and findings of laryngeal irritation in smokers after a smoking cessation period using RSI and RFS.
Materials and Methods
We conducted a prospective cohort study, including 24 volunteers, who were admitted to the cigarette cessation section of family care department of our hospital. All investigations were performed in accordance with the declaration of Helsinki on biomedical studies involving humans, and informed consent was obtained from all study participants. The study was approved by the local institutional review board (E-18-1836).
Participants were excluded from the study if they had a history of gastric, intestinal surgery, or laryngeal surgery. Also, participants who were diagnosed with a neurodegenerative disease (Parkinson or dementia), psychiatric disease (psychosis, severe depression, and so on), and mental retardation were excluded. Moreover, a detailed otorhinolaryngologic examination including an endoscopic evaluation of the nasal cavity and laryngeal structures was performed prior to the study. Patients with chronic rhinosinusitis, allergic rhinitis, and nasal polyposis were also excluded. None of the participants used medications for reflux during the follow-up period. The RSI and the RFS, which have been formerly validated for diagnosing LPR, were used for evaluating the symptoms and findings of laryngeal irritation in smokers. 13,14
Endoscopic examinations of the laryngeal structures for RFS was performed using 70-degree, 4-mm rigid telescope and LED light source. Endoscopic images were recorded using endoscope camera system (Karl Storz SE & Co. KG, Tuttlingen, Germany). In participants who had nausea or cough impeding visualization of the laryngeal structures, lidocaine sprayings were applied to the pharynx of the participant and waited for 5 minutes before trying the endoscopic examination. The initial and the postcigarette cessation recordings of the endoscopic laryngeal examinations were scored in a blinded fashion by 2 different otolaryngology specialist, and the mean value of the 2 different experts’ RFS was noted. Endoscopic laryngeal examination and symptom inquiry for RSI were performed at the beginning of the study and after 2 months of cigarette cessation period.
Statistical Analysis
Data were analyzed by means of SPSS version 16.0 (SPSS Inc, Chicago, Illinois). Paired samples t test was used for comparing the olfactory test results that was performed at the beginning of the study and after 2 months of cigarette cessation period. Also, Pearson correlation analyses were performed between the duration of cigarette smoking and the amount of smoking. The level of significance was set at .05.
Results
This study was carried out in 24 volunteers (14 female and 10 male) between the ages of 24 and 62 years. The mean age of the patients was 44.6 ± 11 years. The mean duration of smoking was 26.3 ± 13 years (range: 6-50 years), and the participants were smoking 21.4 ± 5.9 cigarettes/day (range: 10-30 cigarettes/d).
When we compared the results of RSI and RFS that were performed before and after the cigarette cession period, we found that there was a significant improvement both in RSI and RFS (P < .001 and P < .001, respectively). Descriptive statistics of the results from RSI and RFS are given in Tables 1 and 2, respectively.
The Changes in the Parameters of the Reflux Symptom Index (RSI).a
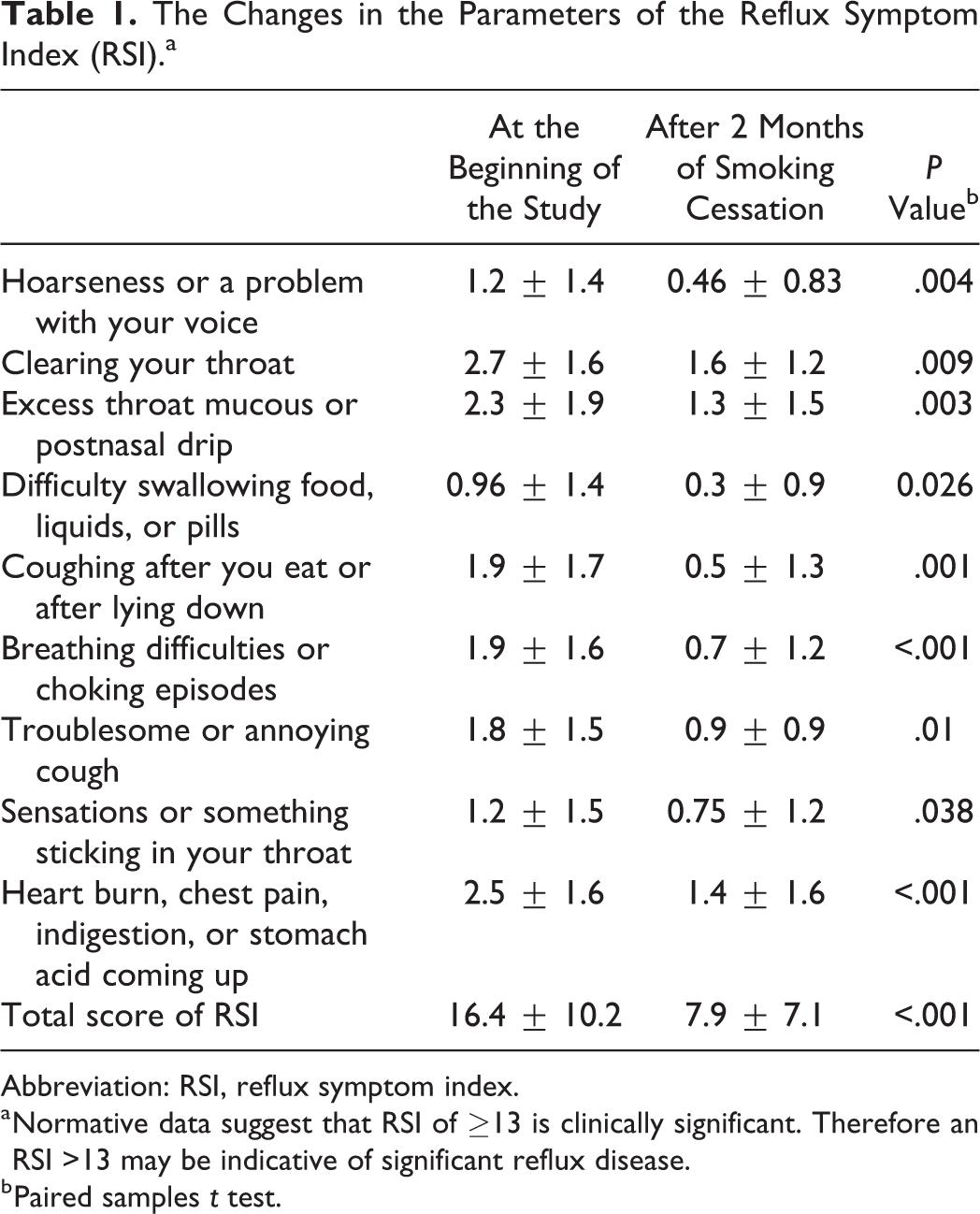
Abbreviation: RSI, reflux symptom index.
a Normative data suggest that RSI of ≥13 is clinically significant. Therefore an RSI >13 may be indicative of significant reflux disease.
b Paired samples t test.
The Changes of Endoscopic Laryngopharyngeal Examination According to the Reflux Finding Score (RFS).a
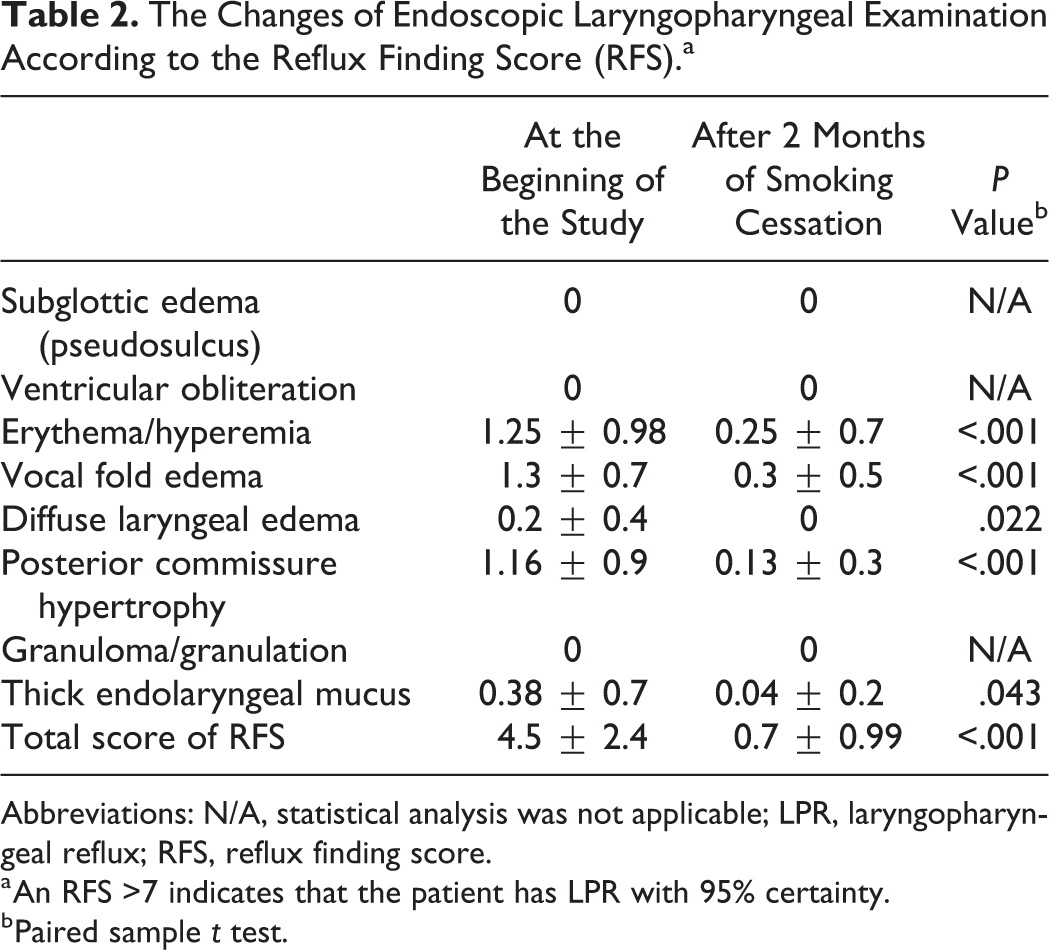
Abbreviations: N/A, statistical analysis was not applicable; LPR, laryngopharyngeal reflux; RFS, reflux finding score.
a An RFS >7 indicates that the patient has LPR with 95% certainty.
b Paired sample t test.
Also, Pearson correlation analyses were performed for investigating the effect of cigarette smoking period and the amount of cigarettes smoked per day on RSI and RFS scores. We find that there was statistically significant correlation between the cigarette smoking period and the RFS score that was determined at the beginning of the study (P = .006, r = .54). Moreover, when we investigate the subtitle examinations of RFS, we found that cigarette smoking period was significantly correlated with vocal fold edema and posterior commissure hypertrophy (P = .001, r = .66; P = .005, r = .56, respectively). On the other hand, we did not find a similar correlation between the number of cigarettes smoked per day and RFS score. Also, we did not find any correlation between RSI score, smoking period, and the number of cigarettes smoked per day.
Discussion
The current investigation had 2 major findings. (1) A significant improvement was found both in RSI and in RFS after smoking cessation period, which was an evidence of improvement in the laryngeal irritation. (2) A significant positive correlation was found between smoking period and RFS, especially with vocal fold edema and posterior commissure hypertrophy.
The larynx is exposed to many toxins due to smoking, which causes chronic laryngeal inflammation in the mucosal structures of the larynx. Laryngopharyngeal reflux, chronic nasopharyngeal discharges due to allergic rhinitis or rhinosinusitis, vocal overuse, and environmental airborne toxins also cause laryngeal inflammation which lead to laryngeal irritation. 16,17
In LPR, the respiratory tract is affected by the reflux of the stomach contents into the airways. The laryngeal irritation is one of the important reasons for applying to the family practitioner. There are anatomical barriers and mechanisms that prevent the formation of LPR in the body. The upper esophageal sphincter, peristaltism, salivation, gravity, and lower esophageal sphincter are the most important components of this barrier. 10,18,19 With the loss of function in these barrier mechanisms, the stomach content backflows into the larynx, causing epithelial damage, inflammation, and altered sensitivity. Acid, bile salts, and pancreatic enzymes may play a role in this damage. However, it is a known fact that nonacid reflux may also lead to this process. 18 -20
Smoking causes duodenogastric reflux. 10 Thus, bile and pancreas content in duodenum can lead to LPR. 5 It is a known fact that smoking causes reflux by loosening the lower and upper esophageal sphincters. With the cessation of smoking, these sphincters become functional again. In addition, with smoking cessation, gastric emptying time is accelerated, and the stomach content that leads to LPR is rapidly discharged from the stomach. 5,6 These mechanisms, which are normalized again as a result of smoking cessation, may lead to decreased RSI and RFS scores in our study.
After the cigarette cessation, the disappearance of chronic chemical irritation may also lead to reduction in RFS and RSI scores. The toxic materials in the cigarette cause laryngeal irritation, which leads to the need to clean the throat in the person. In addition, vocal cord edema and associated hoarseness, as well as respiratory problems and shortness of breath, increase with smoking.
Smoking causes vocal cord edema with chemical trauma, and the posterior commissure of the vocal cords undergoes hypertrophy with LPR which may be increased by smoking. The reflux content comes into contact with the posterior commissure due to the flow direction. The chronic laryngeal irritation is a physiological response to posterior commissure inflammation and hypertrophy.
The major limitation of the study was not to perform the oropharyngeal pH monitoring for confirming whether the LPR was present or not. Although both RSI and RFS were validated for LPR, these diagnostic tools were highly subjective. That is why, the improvements detected by RSI and RFS might be due to both removal of the smoking-related toxins from laryngopharyngeal mucosa and decreased reflux due to smoking cessation.
Conclusion
With cessation of smoking, RSI and RFS scores were decreased in patients with LPR. There was a relationship between smoking period and RFS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.