
Abstract
Objectives:
To evaluate the characteristics of laryngopharyngeal reflux (LPR) in patients with different hypertrophic laryngeal diseases and to explore the relationship between LPR and these diseases.
Methods:
A retrospective analysis was performed. The clinical data of 154 patients were collected. According to their diagnoses, patients were divided into 3 groups. Group 1 included 49 patients with vocal cord polyps. Group 2 contained 52 patients with vocal cord leukoplakia. Group 3 included 53 patients with laryngeal carcinoma. The reflux symptom indexes (RSIs), reflux finding scores (RFSs), and Ryan scores of all patients were evaluated and compared.
Results:
Patients with vocal cord polyps were the youngest of the 3 groups, and those with laryngeal carcinoma were the oldest. A male preponderance emerged in each group. In total, 128 patients (83.12%) had positive RSI/RFS values and 60 (60/146, 41.1%) patients had positive Ryan scores. The positive RSI/RFS rates of both groups 1 and 2 (89.80% and 92.16%, respectively) were significantly higher than that of group 3 (69.81%). Moreover, the positive Ryan score rates in both groups 1 and 2 (39.58% and 53.85%, respectively) were significantly higher than that of group 3 (28.26%).
Conclusions:
Laryngopharyngeal reflux occurs in many patients with vocal cord polyps, vocal cord leukoplakia, and vocal cord carcinoma, indicating that LPR may be important in the pathogenesis of these diseases. Laryngopharyngeal reflux occurs more common in patients with vocal cord polyps and leukoplakia and less common in those with laryngeal carcinoma, suggesting the role of LPR on these diseases may be different.
Introduction
Recently, laryngopharyngeal reflux disease (LPRD) has attracted increased attention from otolaryngologists. Laryngopharyngeal reflux disease consists of a series of signs and symptoms caused by laryngopharyngeal reflux (LPR), in which gastric contents backflow beyond the upper esophageal sphincters. Symptoms of LPRD include pharyngalgia, globus pharyngeus, hoarseness, cough, dyspnea, and so on. 1 Laryngopharyngeal reflux disease is extremely common and is thought to occur in 50% of patients with voice problems and in 10% of patients treated in otolaryngology outpatient departments. 2 However, the relationship between LPR and other laryngeal diseases remains unclear. The damage caused by LPR has been reported as a possible pathogenic factor of benign and malignant vocal cord lesions.3,4 Yet, definitive conclusions are lacking. Additionally, whether the effects of LPR on benign and malignant hypertrophic laryngeal lesions are similar is unknown. Clinical and experimental studies are still needed to better identify the role of LPR in different conditions.
In this article, we summarized and compared the characteristics of LPR in patients with 3 types of hypertrophic laryngeal lesions to explore the relationship between LPR and these lesions.
Patients and Methods
Patients
In this study, we summarized the data of 154 patients treated in the Otolaryngology Department of the China-Japan Friendship Hospital from February 2015 to October 2019 who had various types of hypertrophic laryngeal lesion. According to their diagnoses, patients were divided into 3 groups. Group 1 included 49 patients with vocal cord polyps. Group 2 contained 52 patients with vocal cord leukoplakia. Group 3 included 53 patients with vocal cord carcinoma. All the diagnoses were confirmed by pathology after surgery. The exclusion criteria included incidences of laryngeal infection, allergy, trauma, administration of proton pump inhibitors in the past 3 months, history of previous laryngeal surgery, radiation of the throat, diseases of the spine, and acupuncture treatment of the neck and head. All patients had reflux symptom index (RSI) and reflux finding score (RFS) data, but only 146 patients received Dx-pH monitoring.
Consent was obtained from each patient. This study was approved by the ethics committee of the China-Japan Friendship Hospital.
Reflux Symptom Index and Reflux Finding Score
According to Professor Belafsky, the symptoms and signs of LPRD can be assessed using the RSI and RFS.5,6 All patients were asked to score their symptoms after they indicated that they completely understood the meaning and method of the scoring system (RSI). Two senior otolaryngological physicians, who were blinded to other patient information, independently examined each patient with a trans-nasal fiber-optic laryngoscope and assigned a score to each patient (RFS). The average of the 2 RFS values was used as the RFS value of the patient. If a patient had an RSI > 13 and/or an RFS > 7, then that patient was considered to have an abnormal RSI/RFS score (positive); otherwise, the score was considered to be normal or negative.
Dx-pH Monitoring
All patients underwent a 24-hour pH monitoring of the oropharynx with an Res-tech Dx-pH monitor. 7 The Dx-pH monitor was manufactured by Rayfield Company. When the monitor detected that the pH of the oropharynx was lower than 5.5 (upright) or 5.0 (supine), it recorded the event as 1 reflux episode. The change of pH caused by eating or drinking was eliminated from the record. An upright Ryan score > 9.41 (and/or a supine score ≥ 6.8) was considered to be a positive result, suggesting that the patient had a confirmed LPR event. Otherwise, the patient was considered to have a negative result.
Statistics
SPSS software version 18.0 for Windows (IBM) was used to analyze the data. The χ2 tests were performed for data analysis.
Results
Among the 154 patients, the youngest age was 23 years, and the oldest age was 86 years. The mean age was 56.09 (56.09 ± 13.52) years. The average ages of patients in the 3 groups were 45.67 ± 12.49, 58.06 ± 12.38, and 63.79 ± 8.77 years, respectively. Significant differences were found between each pair of groups when they were compared.
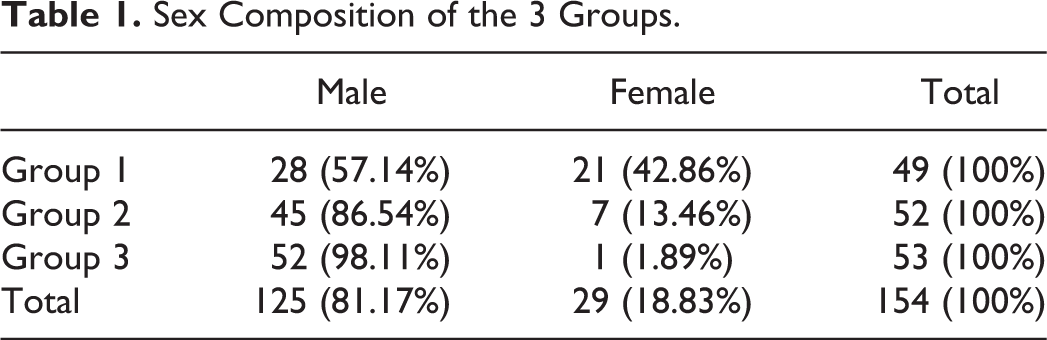
There were 125 male and 29 female patients in total (Table 1). Although the number of male patients was higher than that of female patients in each group, the sex composition was significantly different (P = .000). Significantly more female patients were included in group 1 than in groups 2 and 3 (groups 1 and 2, P = .001; groups 1 and 3, P = .000). However, the difference in sex composition between groups 2 and 3 was not significant (P = .062).
Sex Composition of the 3 Groups.
The RSIs and RFSs of the 3 groups are displayed in Table 2. Among all patients, 128 (128/154, 83.12%) had positive RSI/RFS values. There were 4 (8.16%), 19 (36.54%), and 7 (13.21%) patients with an RSI > 13 in the 3 groups, respectively. Additionally, there were 44 (89.80%), 45 (88.24%), and 36 (67.92%) patients with an RFS >7 in the 3 groups, respectively. The positive RSI/RFS rates of the 3 groups (89.80%, 92.16%, and 69.81%, respectively) were significantly different (P = .003). The positive RSI/RFS rates of both groups 1 and 2 were significantly higher than that of group 3 (Table 3).
RSIs, RFSs, and Ryan Scores of the 3 Groups (M ± SD).

Abbreviations: RFS, reflux finding scores; RSI, reflux symptom index.
P Values of χ2 Tests for Comparisons of Positive RSI/RFS and Ryan Score Rates Between Various Groups.
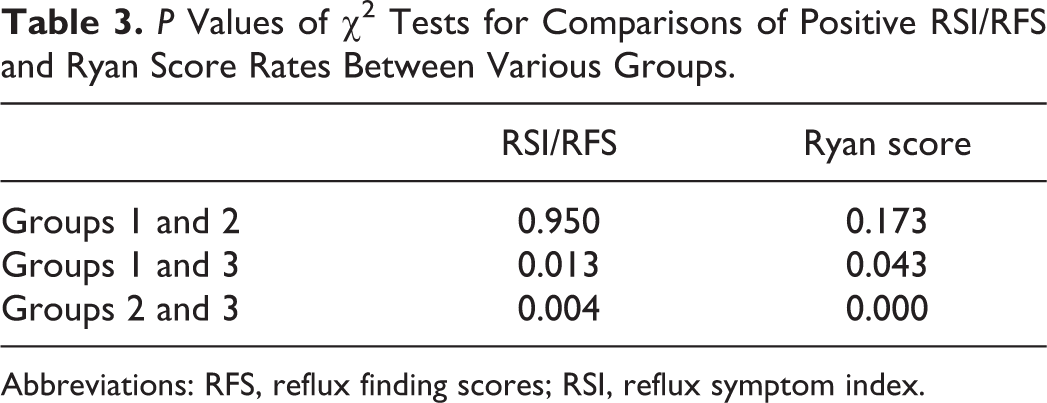
Abbreviations: RFS, reflux finding scores; RSI, reflux symptom index.
The Ryan scores of the 3 groups are also listed in Table 2. In total, 60 (60/146, 41.1%) patients had positive Ryan scores; among these, 1583 upright and 285 supine reflux episodes were detected, including 439 upright and 34 supine episodes in group 1, 889 upright and 221 supine episodes in group 2, and 255 upright and 30 supine episodes in group 3. The number of upright and supine episodes in group 2 was much higher than those in the other groups, but no significant difference was observed (P = .189 and .091, respectively). The positive Ryan score rates (39.58%, 53.85%, and 28.26%, respectively) were significantly different in the 3 groups (P = .001). The positive Ryan score rates in both groups 1 and 2 were significantly higher than that of group 3 (Table 3). The Ryan scores are listed in Table 4.
Upright and Supine Ryan Scores and Their Composition.a
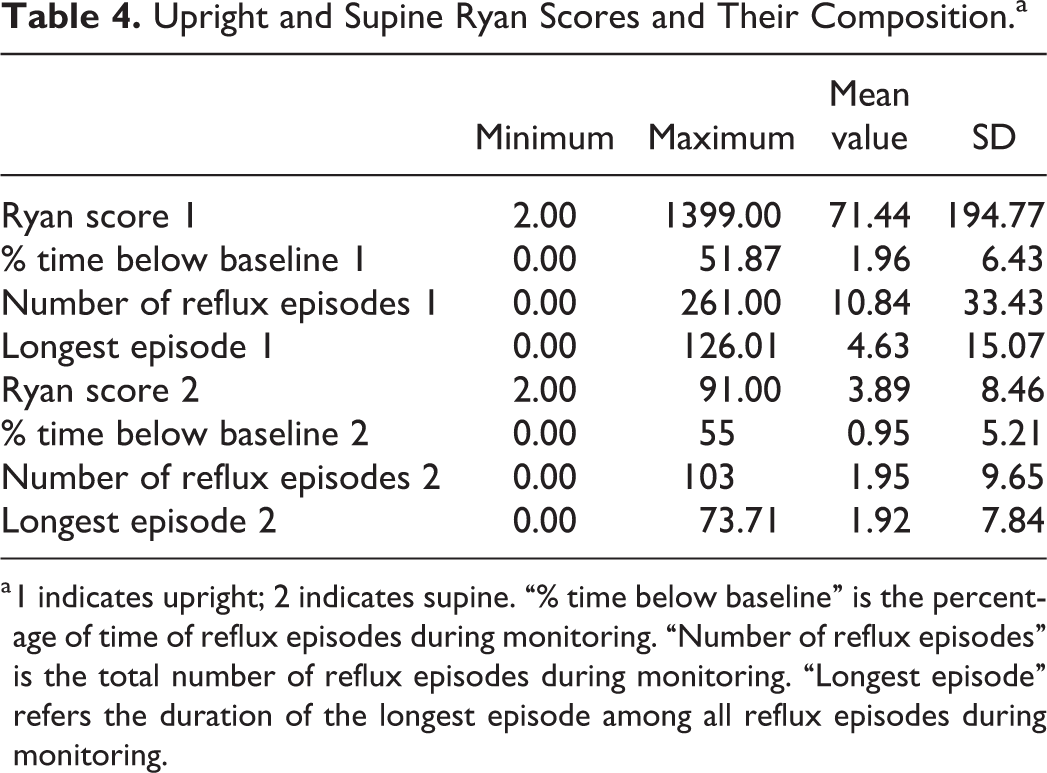
a 1 indicates upright; 2 indicates supine. “% time below baseline” is the percentage of time of reflux episodes during monitoring. “Number of reflux episodes” is the total number of reflux episodes during monitoring. “Longest episode” refers the duration of the longest episode among all reflux episodes during monitoring.
The percentages of patients who had symptoms of gastroesophageal reflux disease (GERD), such as regurgitation and heartburn, were not significantly different among the 3 groups (66.67%, 60.00%, and 50.94%, respectively, P = .271).
Discussion
Laryngopharyngeal reflux is found in patients with various laryngeal diseases, especially hypertrophic lesions. Injury from LPR could cause increased susceptibility of the vocal cord mucosa to damage and subsequent formation of polyps, nodules, or Reinke’s edema. 3 Additionally, LPR is associated with laryngeal malignancy. 4 However, whether LPR has the same effect with regard to benign and malignant laryngeal lesions remains unknown. In this article, we summarized the characteristics of LPR in 3 types of laryngeal hypertrophic lesions: vocal cord polyps (benign hypertrophic lesions), vocal cord carcinoma (malignant lesions), and vocal cord leukoplakia (lesions in the range between benign and malignant classification).
The age composition differed in the 3 groups in our study. Patients with vocal cord polyps had the youngest average age, and patients with laryngeal carcinoma had the oldest average age. This is consistent with other studies. Tsui et al found that patients with benign phonotraumatic lesions (vocal nodules, polyps, and cysts) were predominantly younger, and patients with glottic neoplasms were older. 8 Zhukhovitskaya et al noted that patients with vocal cord leukoplakia were the oldest group among patients with benign vocal cord lesions. 9 In one analysis of vocal cord leukoplakia, age was confirmed as an independent factor associated with malignancy. 10 Therefore, the age trend in our study was reasonable and may be due to different types of vocal cord lesions.
A male preponderance was observed in the 3 groups, which is similar to other reports. Zhukhovitskaya et al and Malik et al found that vocal cord polyps and leukoplakia occurred predominantly in men.9,11 Tsui et al reported that patients with glottic neoplasms were predominantly male, but patients with phonotraumatic lesions (including vocal nodules, polyps, and cysts) were predominantly female. 8 The latter is different from other reports and our study. The reason may be due to differences in the sample size or races of patients. It is interesting to note that the sex composition in our study was significantly different, although male patients exceeded female patients in each group. More female patients were included in group 1 than in the other 2 groups. This probably occurred because of the limited number of patients in our study. However, this also may have been an actual tendency that requires further research to explore the mechanism.
The RSI and RFS were proposed to evaluate the symptoms and signs of LPRD patients.5,6 Because of their simplicity, convenience, validity, and reliability, these indexes are widely used in clinical practice. Commonly, if a patient’s RSI is greater than 13 and/or their RFS is greater than 7, the patient can be diagnosed with suspected LPRD. In our study, 128 patients in total had positive RSI/RFS values, indicating that most patients with hypertrophic laryngeal lesions had suspected LPRD and that LPR may play an important role in the pathogenesis of these lesions. The results agreed with those in the literature.3,4 Meanwhile, the positive RSI/RFS rates of groups 1 and 2 were significantly higher than that of group 3. Patients with vocal cord polyps and leukoplakia seemed to have LPR more commonly than patients with vocal cord carcinoma. However, further discussion is needed to reach a conclusion. First, the RSI and RFS have their limitations. Although the RSI and RFS are the most frequently used measures to assess clinical outcomes, they are incomplete and only take into account some aspects of LPR symptoms and findings. 12 Reflux symptom index contains 9 items, 8 for pharyngolaryngeal and respiratory symptoms and 1 for digestive symptoms, without other complaints such as ear, nose, oral cavity, and so on.13,14 Moreover, RSI considers the severity of symptoms but not their frequency. 14 That is why reflux symptom score (RSS) is proposed recently and seems more accurate and promising. 14 But RSS is a newer index which is later than our research in this article and should be applied in the future study. Reflux finding score only evaluates some laryngeal signs, omitting signs of other tissue, such as the coated tongue, uvula erythema, and so on. 15 So the reliability of RFS in diagnosing LPR is controversial. 16 Second, the RSI and RFS are evaluated by patients and/or physicians; therefore, they are not objective scores and may differ among individuals. So RSI and RFS are insufficiently specific screening tools for LPR diagnosis. Third, the sample size of this study is limited.
Restech Pharyngeal pH monitoring (Dx-pH monitoring) was introduced to detect aerosolized and liquid acid and overcome the artifacts that occur when measuring pharyngeal pH with the existing catheters.17-19 As this device is minimally invasive, sensitive to pH changes, more tolerated by patients, and easily manipulated, it is widely used to evaluate LPR. 20 In our study, 60 patients had positive Ryan scores, which indicated that pathological LPR was present in these patients and may have played a pathogenic role in their condition. This result was in accordance with other studies.3,4 Reflux episodes detected were mainly in an upright position which conformed to the characteristics of LPR. However, the positive rates of Ryan score in all patients and each group seemed lower than those for the RSI/RFS (P = .029). This may be due to the limitations of RSI/RFS and Restech Pharyngeal pH monitoring. The limitations of RSI/RFS are discussed in the previous paragraph. One disadvantage of Restech Pharyngeal pH monitoring is that it only detects acidic episodes and only records a portion of weak acidic episodes (upright pH < 5.5, supine pH < 5.0). 19 That is, the patients with LPR confirmed by Dx-pH monitoring are mainly severe acid LPR patients. However, even in asymptomatic subjects, most pharyngeal reflux is nonacid because of “shrinking” and “buffering” phenomena. 21 Duodenogastroesophageal reflux, as a type of nonacidic reflux, can exist independently or combined with GERD, and nonacid refluxate can damage the larynx, pharynx, and other extraesophageal tissues. 22 Laryngopharyngeal reflux patients without GERD had a higher proportion of nonacid and mixed reflux episodes than LPR/GERD patients. 23 Therefore, Restech Pharyngeal pH monitoring may omit some nonacid reflux episodes, which may explain the inconsistency of positive rates between the RSI/RFS and Ryan score. Moreover, refluxates other than gastric acid also can damage extragastric tissues, 24 which may also contribute to the inconsistency between RSI/RFS and Ryan score.
The percentages of patients with symptoms of GERD were not significantly different among the 3 groups. This indicated the incidence rates of GERD in 3 groups were similar.
Despite the limitations of both the RSI/RFS and Pharyngeal pH monitoring, 2 similar and interesting phenomena were observed in our study. First, positive rates were considerable for both the RSI/RFS and Ryan score in the 3 groups, which strongly indicated that LPR occurs in patients with hypertrophic vocal cord lesions, and LPR may play an important role in the pathogenesis of these lesions. These results coincided with the findings in the literature. Laryngopharyngeal reflux can damage the epithelium of the larynx and induce inflammation and formation of nodules, polyps, or Reinke’s edema. 3 Additionally, LPR is associated with the development of vocal fold leukoplakia and the presence of laryngeal malignancy.4,25 Second, the positive rates of both the RSI/RFS and Ryan score in groups 1 and 2 were significantly higher than those of group 3, although the percentage of patients with symptoms of GERD in 3 groups was similar. Laryngopharyngeal reflux seemed to be more often present in patients with vocal cord polyps and vocal cord leukoplakia and less often present in those with vocal cord carcinoma, indicating the role of LPR in vocal cord carcinoma may differ from that in vocal cord polyps and leukoplakia. This tendency has not been previously proposed and requires further discussion and research. We suppose laryngeal carcinoma may emerge when some kind of reflux emerges or damage caused by LPR reaches a certain degree or coordination of some kind of factors exists. Recently, some carcinogenetic mechanisms in nonacidic environments have been found which indicates laryngeal carcinoma may be caused by nonacid reflux. Pepsin, at pH 7.0, significantly altered the expression of 27 genes implicated in carcinogenesis, which supports the role for refluxed pepsin in the promotion of epithelial proliferation and carcinogenesis of the larynx and pharynx. 26 Pepsin (pH 7.0) also induces epithelial mesenchymal transition of cells in laryngeal carcinoma through the IL-8 signaling pathway, which indicates that it has a potential role in enhancing cell proliferation and metastasis of laryngeal carcinoma. 27 Exposure of hypopharyngeal cells to pepsin at pH 7.4 damaged mitochondria and the Golgi complex and induced cell toxicity. 28 Animal and human studies suggest that duodenogastroesophageal reflux is involved in the pathogenesis of laryngeal carcinoma.29,30 Gastroduodenal reflux has been confirmed to play a role in hypopharyngeal carcinogenesis, and its effect is mediated through activation of the nuclear factor-κB pathway. 31 Because these possible carcinogenetic mechanisms occur in nonacid environments, we suggest that LPRs in patients with laryngeal carcinoma may be more nonacid refluxes compared to patients with vocal cord polyps and leukoplakia. Compared to acid reflux, it is probable that nonacid reflux is relatively fewer in total. And some nonacid reflux cannot be detected by Pharyngeal pH monitoring. These may explain why fewer patients with laryngeal carcinoma had positive RSI/RFS and Ryan scores than patients with vocal cord polyps and leukoplakia. This finding requires further research for confirmation.
Certainly, this study had some limitations, such as the limited sample size and the disadvantages of RSI/RFS and Restech Pharyngeal pH monitoring. However, any method or instrument has defects that should be considered when discussing the results, and methods should be proposed to overcome these limitations in the future.
In summary, many patients with hypertrophic vocal cord lesions had positive RSI/RFS and/or Ryan scores, which indicated that LPR may play a role in the pathogenesis of vocal cord polyps, leukoplakia, and carcinoma. The positive rates of both the RSI/RFS and Ryan score in patients with vocal cord polyps and leukoplakia were higher than those of patients with laryngeal carcinoma, indicating that LPR may be more common in the former 2 types of lesions and less common in the last type, and the role of LPR on different hypertrophic laryngeal diseases may be different. Further research is needed to explore this. In addition, the average age of patient groups increased in the following order: vocal cord polyps, leukoplakia, and carcinoma. A male predominance was observed in all 3 of these diseases.
Footnotes
Acknowledgments
The authors thank the colleagues of Gastroenterology Department of China-Japan Friendship Hospital for their help in the oropharynx pH monitoring.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by China-Japan Friendship Hospital (Grant 2015-2-QN-40 and 2015-2-MS-7).