
Abstract
Purpose
This study investigated the characteristics, diagnosis, and treatment of Warthin tumors (WTs) to explore the possibility of managing patients by observation.
Methods
We reviewed the records of 1167 patients with benign parotid tumors who were seen in our department between September 1999 and April 2021. Among them, 387 cases were WT and 668 cases were pleomorphic adenoma. We evaluated preoperative diagnoses of WT by symptoms/signs, fine-needle aspiration cytology (FNAC), imaging, such as ultrasonography and magnetic resonance imaging, and technetium-99m pertechnetate (Tc-99m) scintigraphy. Fisher’s exact test and the Mann–Whitney U test were used in statistical analyses.
Results
Warthin tumors were treated by surgery in 238 cases and follow-up in 149 cases. The 238 patients were diagnosed as WT at the final pathology after surgery. Among them, 172 patients (72.3%) were determined as benign histological type by preoperative FNAC; in these 172 patients, 170 (71.4%) were correctly diagnosed as WT in the final pathology. Preoperative Tc-99m scintigraphy was performed in 69 patients diagnosed with WT by final pathology or FNAC, and the positive rate of Tc-99m scintigraphy in WT was 75.4%.
Conclusions
Combining FNAC and Tc-99m scintigraphy, as well as considering clinical findings, enables the diagnosis of WT in most cases. In particular, WT is more common in the elderly, grows more slowly, and is less likely to be malignant. Therefore, if WT can be diagnosed preoperatively with a high rate of correct diagnosis, it could be an accurate and effective means of managing patients through follow-up without surgery.
Keywords
Introduction
Pleomorphic adenoma (PA) is the most common benign tumor occurring in the parotid gland and accounts for 60% to 70% of cases. 1 The second most common type is Warthin tumor (WT), and PA and WT combined account for approximately 90% of all benign parotid tumors.2,3 However, the prevalence of WT has been increasing, and a report indicates that it is now more common than PA. 4
Because WT and PA comprise such a large percentage of benign parotid tumors, it is crucial to differentiate between them for preoperative diagnosis. Malignant transformation of PA can occur 5 and it develops in relatively young people; thus, most cases are indicated for surgery. In contrast, WT is more common in older adults and rarely transform to malignancy; therefore, it can be managed by observation, although aesthetic issues may remain. 6 Because of these differences between PA and WT, a reliable differential diagnosis is critical for determining the appropriate treatment approach. Besides symptoms/signs, fine-needle aspiration cytology (FNAC) and imaging, such as ultrasonography and magnetic resonance imaging, can be used for the preoperative diagnosis of parotid tumors. Moreover, technetium-99m pertechnetate (Tc-99m) scintigraphy may also be used to diagnose WT. 7
In our department, we have been diagnosing and treating parotid tumors for over 21 years. In recent years, the number of cases in which WT is managed without surgery has increased. Because we have now seen a total of over 1000 cases of PA and WT, we decided to investigate the differential diagnosis and other features of the two conditions, as well as the clinical characteristics and management of WT.
Materials and Methods
Patients
We reviewed the records of 1167 patients with benign parotid tumors (excluding recurrences) who were seen in our department between September 1999 and April 2021. Among them, WT (238 cases) and PA (668 cases) were confirmed by the final pathology of surgical specimen and WT (149 cases) which were managed by observation. In patients who underwent surgery, the tumors were histopathologically classified according to the 2017 WHO classification. 8 During the same period, we treated 222 cases of malignant parotid tumors.
The study was approved by our institutional review board (approval no. #2621-1).
Characteristics of WT and PA
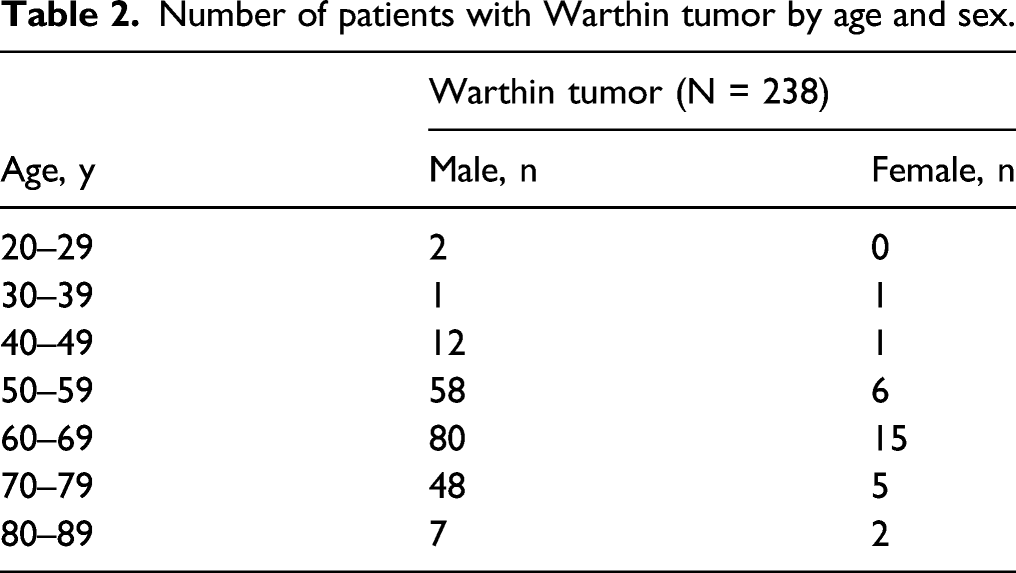
In patients receiving surgery for WT or PA, we evaluated age, sex, duration of disease, tumor diameter, tumor location, symptoms/signs, operation time, bleeding volume, and postoperative facial paralysis. A lower pole tumor was defined as a tumor whose center was more caudal than the marginal mandibular branch of the facial nerve. 9 The age distribution of patients with WT was examined separately for men and women.
Fine-Needle Aspiration Cytology
Ultrasound-guided FNAC was performed preoperatively in all patients undergoing surgery. We examined the preoperative FNAC findings in patients who were diagnosed with WT at the final pathology after surgery and the final pathology results in patients who were diagnosed as having WT at the preoperative FNAC. Fine-needle aspiration cytology results were categorized according to the Osaka Medical College salivary gland cytology classification system, which consists of 11 categories. 10
Technetium-99m Pertechnetate Scintigraphy
Preoperative Tc-99m scintigraphy was performed for the patients with parotid tumor according to the following principal. Preoperative Tc-99m scintigraphy was performed for the patients with 65 surgery cases and 46 observation cases. In surgery cases, Tc-99m scintigraphy was performed for the cases that WT was suspected by symptoms/signs and image findings, but not confirmed by FNAC. In observation cases, it was performed for the cases that WT was suggested strongly by various signs such as history, FNAC, symptoms/signs, and image findings. Lemon juice stimulation was used to measure Tc-99m.
Surgery
During the period targeted in this study, parotid tumors were diagnosed and treated under a predefined policy. 11 In principle, surgery was performed by a partial superficial parotidectomy under general anesthesia. An S-shaped incision was made in the skin to reveal the operative field. For processing the nerve, the main trunk of the facial nerve was identified, followed by the identification and dissection of the branch required for tumor resection. An electronic scalpel was used to resect parotid tissues. If a tumor was located just above the superficial layer of the main trunk, a peripheral nerve was then identified to perform a retrograde dissection due to the difficulty of nerve identification in the main trunk. For cases of deep lobe tumor, superficial lobe tissue was dissected to identify nerves then returned to its original position after resection of the tumor. Facial nerve monitoring was used from September 2014. No medication, such as steroids, was used when facial paralysis developed postoperatively.
Patients With WT Treated by Surgery or Observation
We compared the age, sex, tumor diameter, tumor location, symptoms/signs, use of Tc-99m scintigraphy, and FNAC findings between patients with WT who underwent surgery and those who were managed by observation.
Postoperative Facial Paralysis
We examined factors associated with postoperative facial paralysis in WT and PA, including age, sex, histopathological type, tumor diameter, tumor location, symptoms/signs, operation time, and bleeding volume. We also examined the time to recovery from paralysis in patients with WT or PA who developed postoperative facial paralysis and were followed up for at least 24 months after surgery.
Statistical Analysis
For WT and PA, Fisher’s exact test was used to compare sex, tumor location, pain/tenderness, adhesion, and presence of facial paralysis, and the Mann–Whitney U test was used to compare age, tumor diameter, operation time, and bleeding volume. Univariate and multivariate analyses were used to evaluate postoperative facial paralysis in WT and PA, respectively. In the univariate analysis, Fisher’s exact test was used for sex, tumor location, pain/tenderness, and adhesion, and the Mann–Whitney U test was used for age, tumor diameter, operation time, and bleeding volume. In the multivariate analysis, binomial logistic-regression analysis was used, with the presence or absence of postoperative facial paralysis as the dependent variable. In binomial logistic regression, bleeding volume was estimated to depend on operation time because correlations were observed between the 2 items (WT, r = .501; PA, r = .448; both P < .05 by Spearman’s rank correlation coefficient). Therefore, operation time was used, and bleeding volume was excluded from independent variables. To enable independent variables to be studied in detail, the following variables were recoded as categorical variables on the basis of the respective frequency distribution: age, which was divided into 3 categories (<45, ≥45 to <70, and ≥70 years); tumor diameter, which was divided into 2 categories (<25 and ≥25 mm); and operation time, which was also divided into 2 categories (<120 and ≥120 min). The reference categories for the independent variables were as follows: age, less than 45 years old; sex, male; tumor diameter, < 25 mm; tumor location, superficial lobe; pain/tenderness, none; adhesion, none; and operation time, < 120 minutes. In all analyses, a P value less than .05 was considered statistically significant.
Results
Characteristics of WT and PA
During the study period, 149 patients with WT were managed by observation; definite or suspected WT was diagnosed by FNAC in 141 of these patients and by Tc-99m scintigraphy in the remaining 8 patients. The symptoms/signs and other examinations in these patients did not contradict a diagnosis of WT.
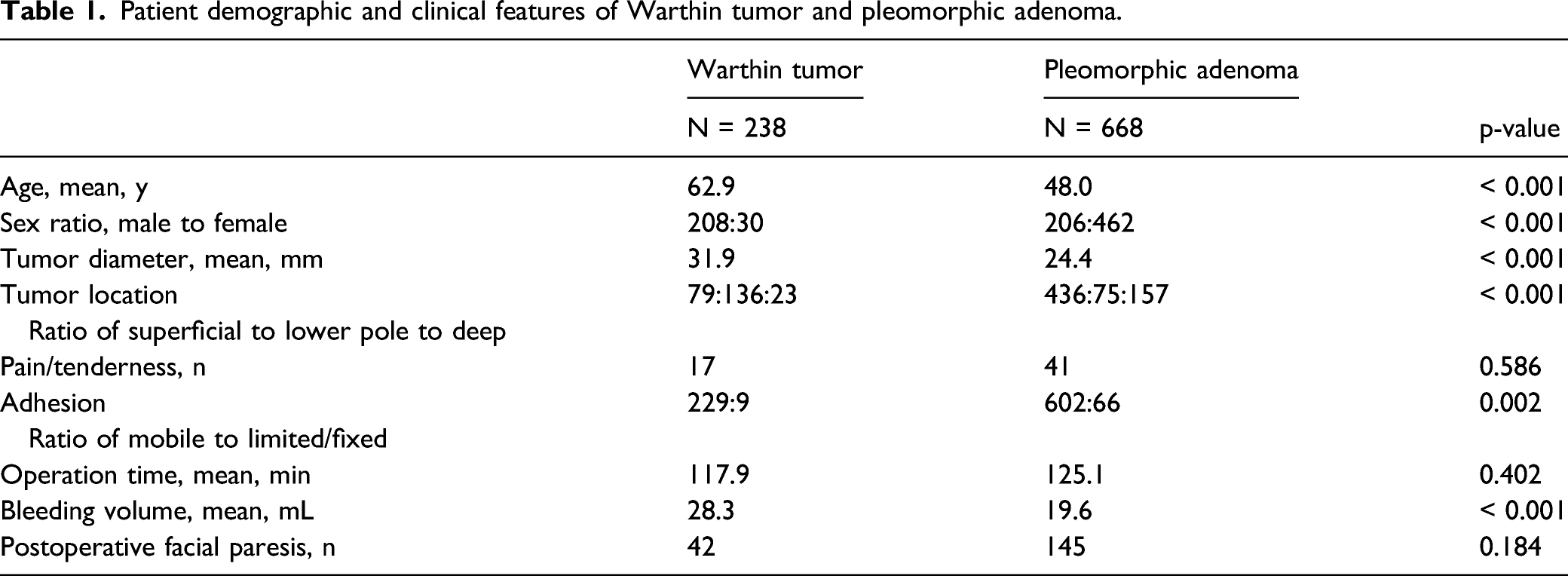
Patient demographic and clinical features of Warthin tumor and pleomorphic adenoma.
Number of patients with Warthin tumor by age and sex.
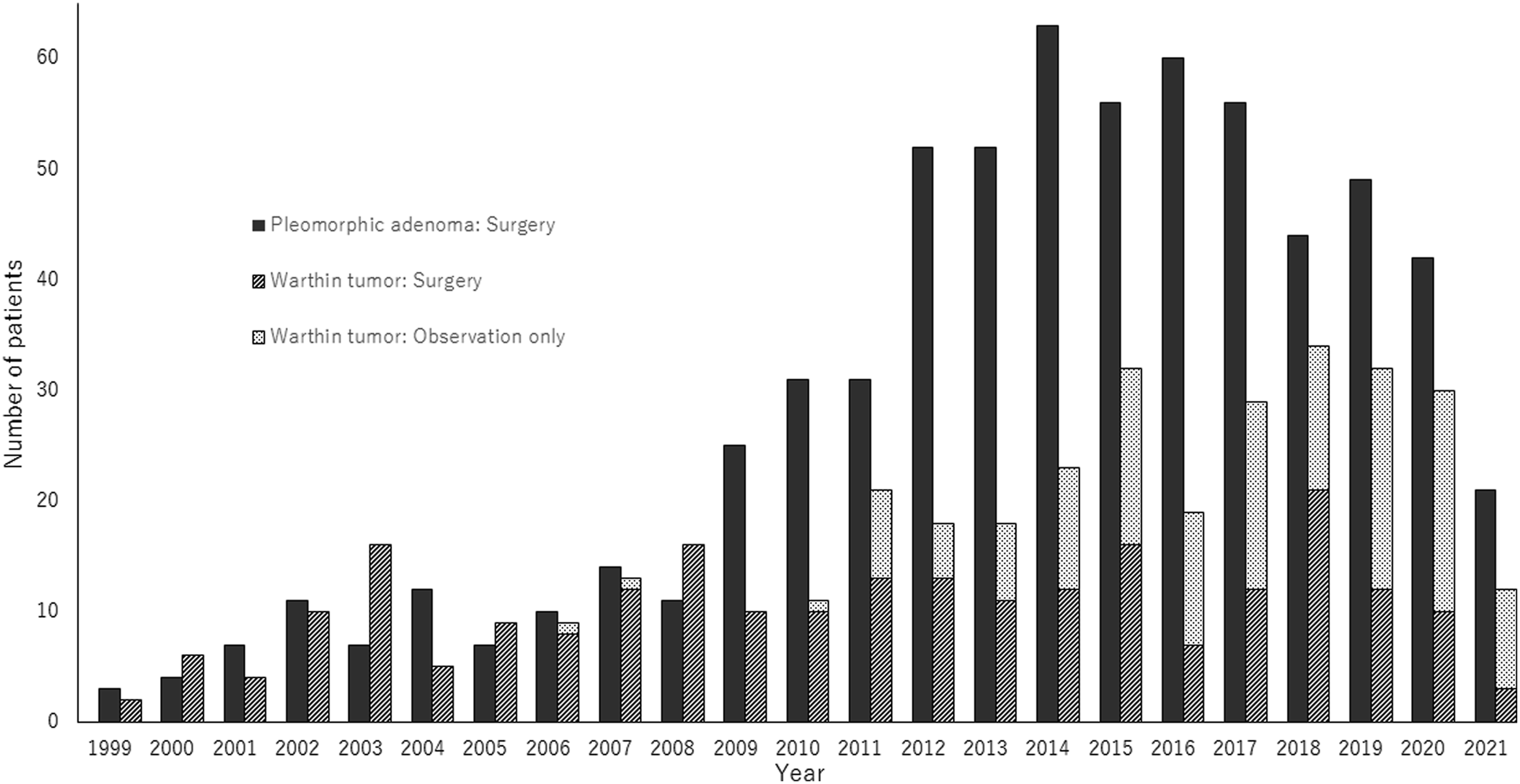
Cases of pleomorphic adenoma (PA) and Warthin tumor (WT) by year (1999–2021). In WT, management by observation has increased since 2011. The number of cases of PA has increased from 2012. The overall WT:PA ratio is 1:1.7.
Fine-Needle Aspiration Cytology
Fine-needle aspiration cytology (FNAC) results according to the Osaka Medical College (OMC) system.
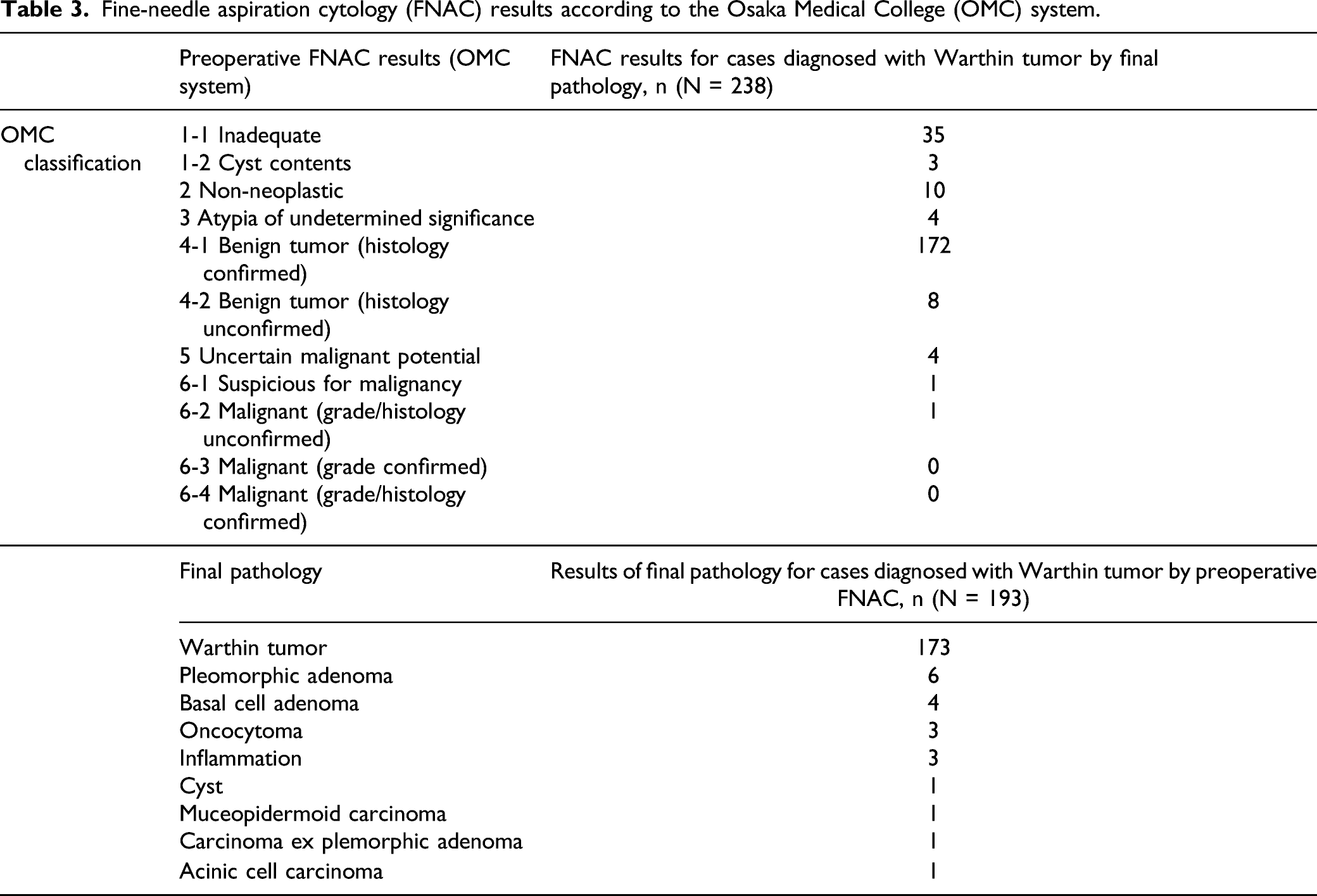
On the other hand, a total of 193 patients among all surgical cases were diagnosed with WT by preoperative FNAC. In these patients, the final pathology after surgery identified WT in 173 patients (89.6%), PA in six, and malignancy in three (1.6%) (Table 3).
Technetium-99m Pertechnetate Scintigraphy
Results of preoperative technetium-99m pertechnetate scintigraphy in cases (N = 111) managed by surgery or observation.
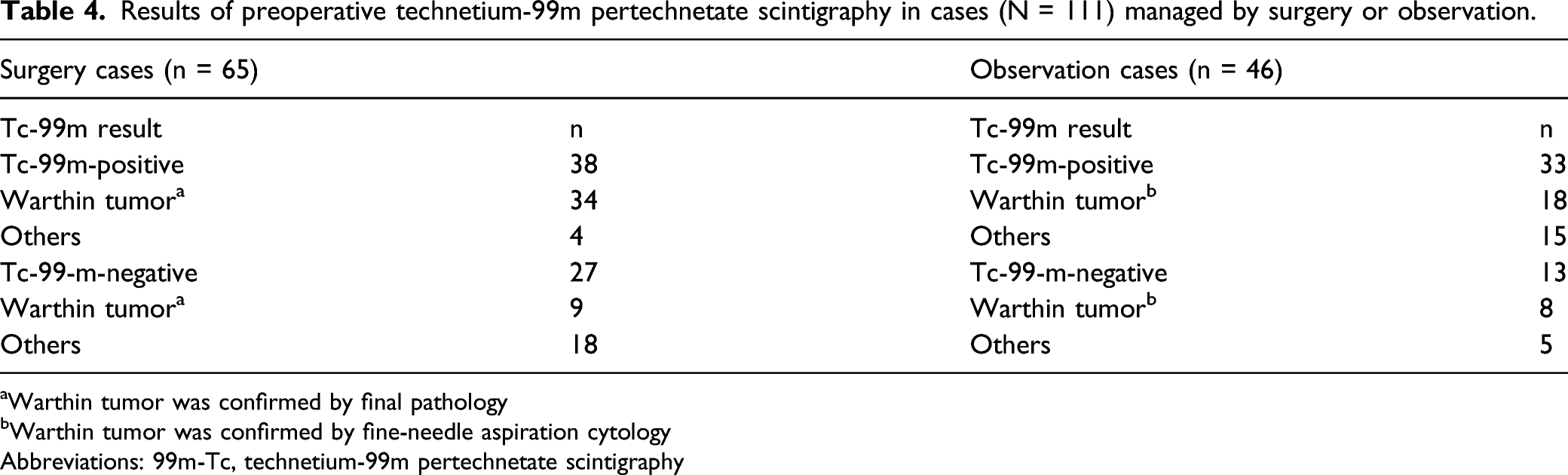
aWarthin tumor was confirmed by final pathology
bWarthin tumor was confirmed by fine-needle aspiration cytology
Abbreviations: 99m-Tc, technetium-99m pertechnetate scintigraphy
Patients With WT Treated by Surgery or by Observation
Characteristics of patients with a Warthin tumor managed by surgery or observation.
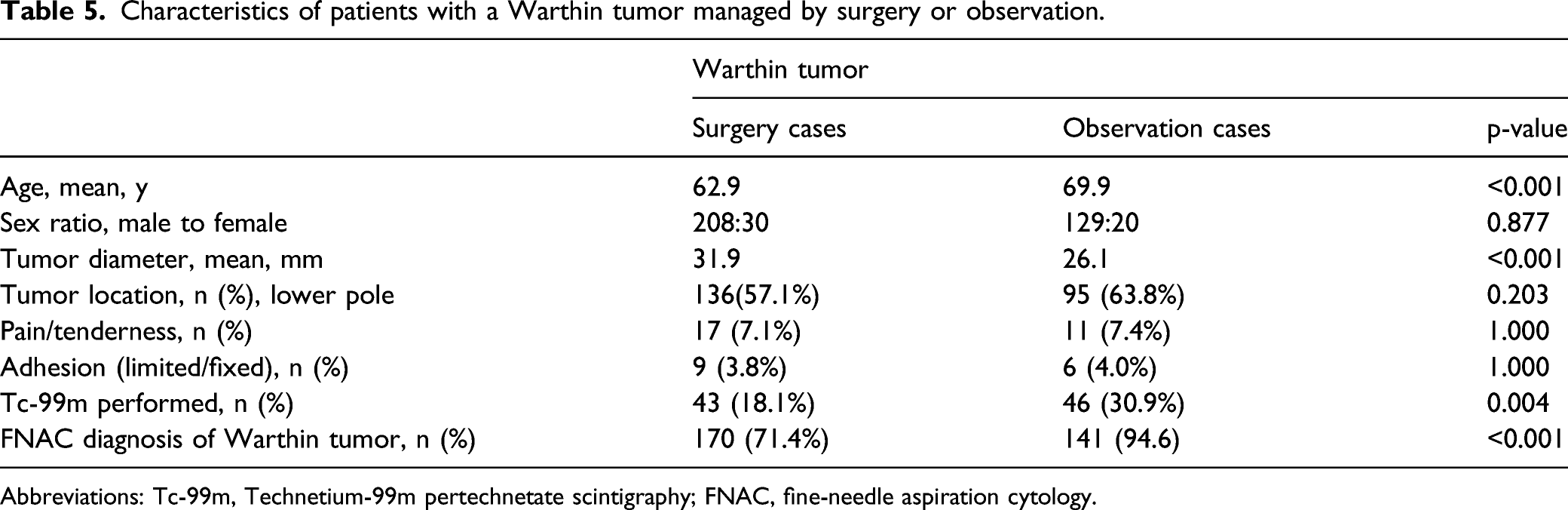
Abbreviations: Tc-99m, Technetium-99m pertechnetate scintigraphy; FNAC, fine-needle aspiration cytology.
Postoperative Facial Paralysis
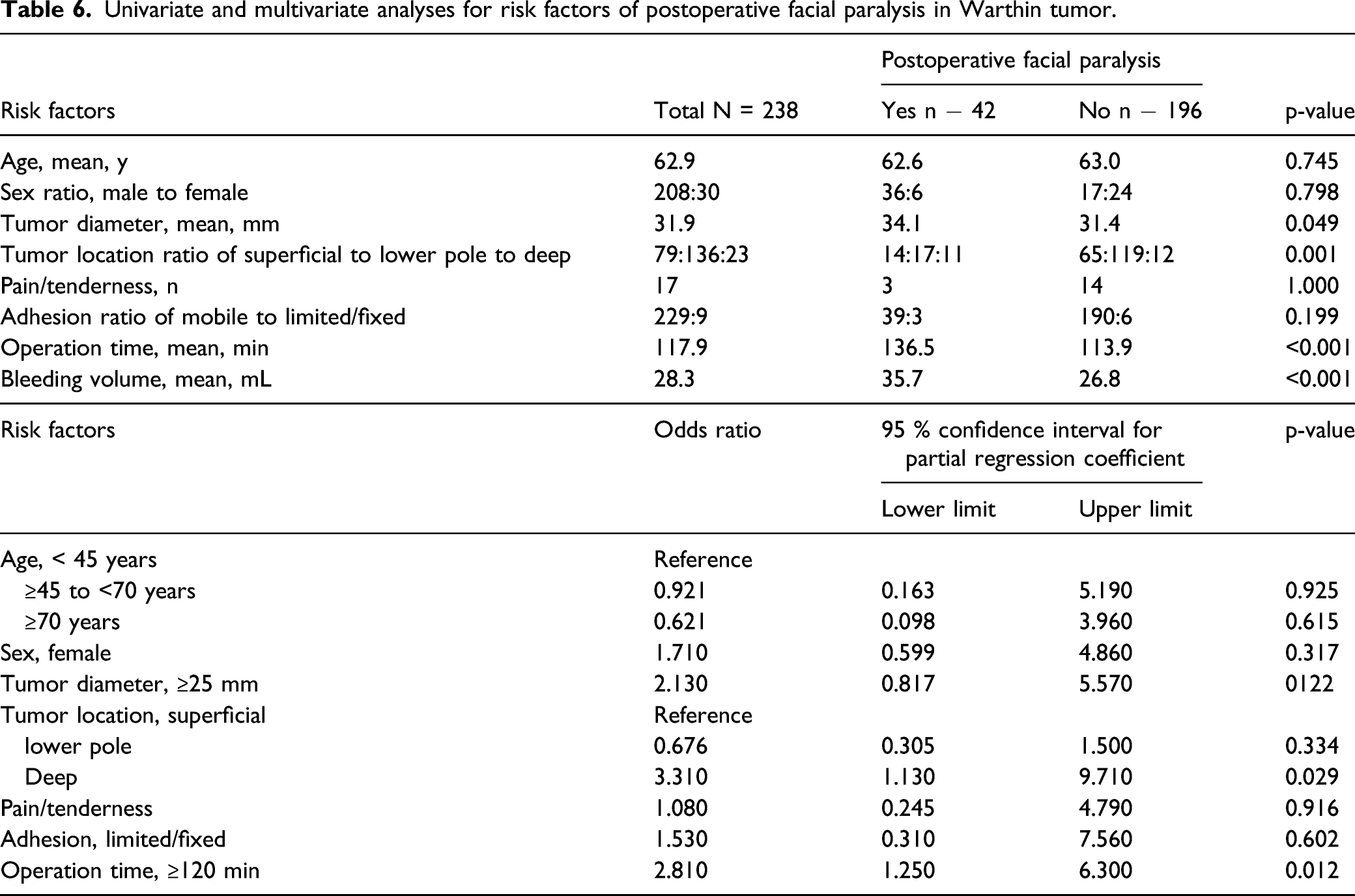
Univariate and multivariate analyses for risk factors of postoperative facial paralysis in Warthin tumor.
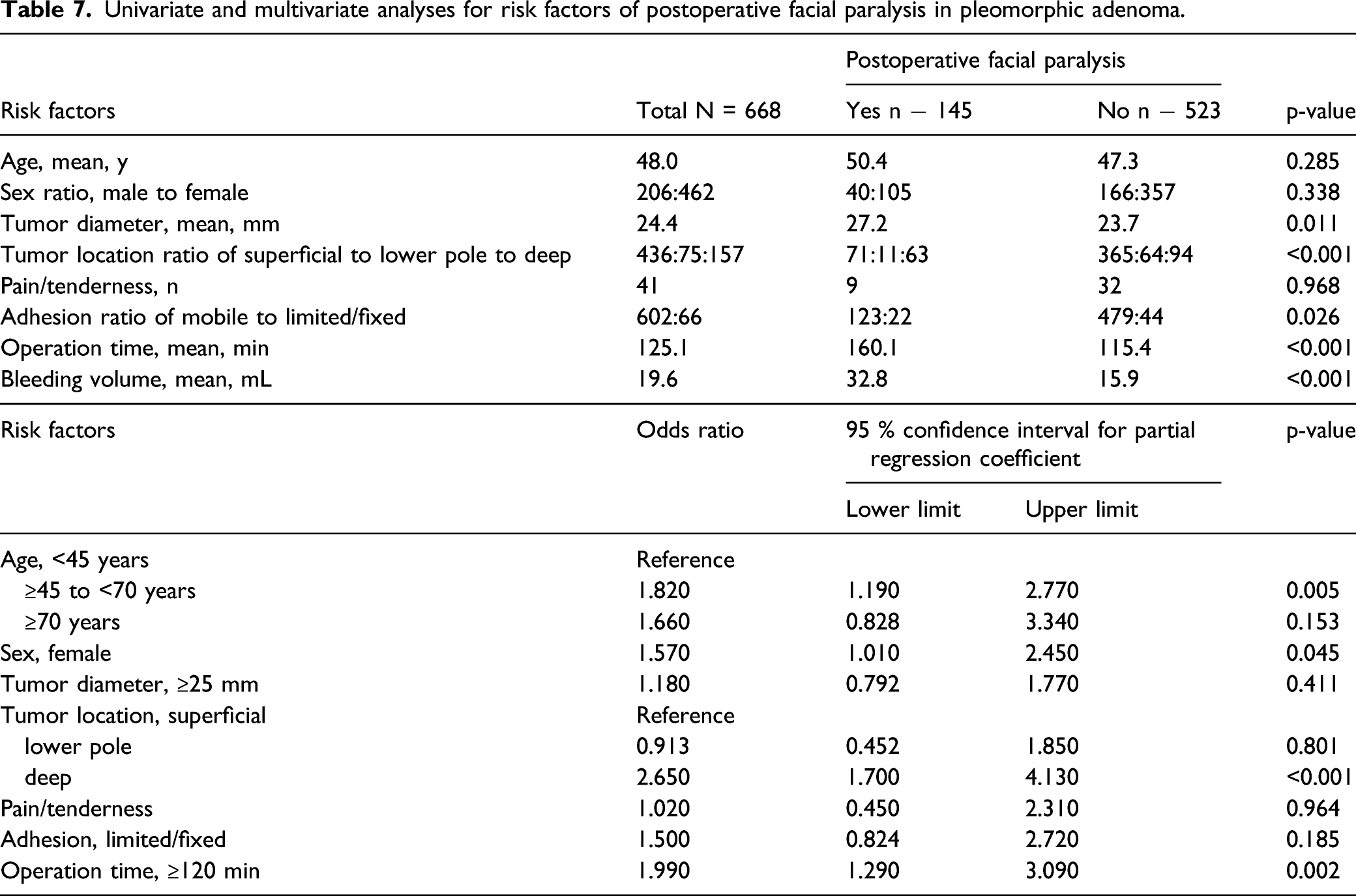
Univariate and multivariate analyses for risk factors of postoperative facial paralysis in pleomorphic adenoma.
Discussion
Pleomorphic adenoma is generally perceived to be the most common histological type of benign parotid tumor and WT to be the second most common histological type. 12 However, recent studies, primarily from Europe, found that cases of WT are increasing. Luers et al.1 showed that cases of WT increased approximately two-fold from 1990 to 2014, to a PA:WT ratio of almost 1:1. Psychogios et al. 4 reported on 201 patients with WT and 138 with PA who underwent surgery between 2014 and 2018 and found that WT was the most common type of benign parotid tumor. Reasons for the increase in WT may be that it is more common in advanced age people, and life expectancy has been increasing in recent years; furthermore, surgery is becoming safer to perform in older people. Other reasons may be related to improved detection rates because of advances in imaging technologies and increased awareness of parotid tumors among general practitioners. Moreover, advances in surgical techniques may have increased the safety of operations on parotid tumors. Our study shows that cases of PA increased markedly from 2012 onward. Furthermore, the number of cases of WT that were managed by observation only rose from 2011 to 2021, increasing the ratio of surgery cases to observation cases to approximately 1:1. However, in the overall study period, the case number ratio of PA to WT was 1.7:1, and the number of cases of PA remained higher. When examining the PA to WT ratio in the future, studies will need to clarify whether the sample consists of only surgery cases or hospital-based cases.
Transient postoperative facial paralysis, the most problematic postoperative complication after surgery for parotid tumors, occurred in both PA and WT, and the frequency did not differ significantly between the two histological types. Multivariate analysis showed that the odds ratio for facial paralysis in both WT and PA was higher in patients with a tumor in the deep lobe than in those with one in the superficial lobe. Regardless of histological type, deep lobe tumor resection requires a larger area of nerve dissection and the operation time is often longer, which may explain the higher odds ratio for this tumor location. The time to recovery from postoperative facial paralysis was 6 months in 80% to 90% of patients, which was similar to previous reports.13-15 Time to recovery was slightly shorter in patients with WT than in those with PA, and all patients with WT recovered within 8 months, whereas some with PA needed longer time to recover. The reason for this difference may be that WT occurs more often in men, who tend to have larger nerve diameters than women and are therefore less likely to experience paralysis in case of nerve damage, and that WT is often located in the lower pole, thereby requiring only a small amount of dissection.
Because WT is more common in advanced age people, progresses slowly, and rarely becomes malignant, managing patients by observation without surgery is a valid option for this type of tumor. A study on the rate of enlargement of WT reported an increase of .26 cm per year. 6 When deciding to treat patients with WT by observation only, a histological diagnosis of WT should be established preferably. In the present study, about 90% of cases proved to be an accurate histopathology (WT) by the final pathological diagnosis when the parotid tumors were diagnosed as WT by preoperative FNAC, and only 3 patients (1.6%) were diagnosed as having a malignant tumor at the final pathology. Jechova et al. 16 reported that 93.1% of 216 patients diagnosed with WT by FNAC were confirmed to have WT and 7 (3.2%) were found to have a malignant tumor. Borsetto et al. 17 conducted a similar study and found that 89% of patients were diagnosed with WT and only 4.2% had a malignant tumor, while the rate of correct histological diagnosis in preoperative FNAC among patients diagnosed with WT at the final pathology was approximately 70% in our study.
Another useful tool for preoperative diagnosis of WT is Tc-99m scintigraphy. In this study, the positive rate of Tc-99m scintigraphy in WT was 75.4%. Miyake et al. 7 reported that acid-stimulated Tc-99m scintigraphy had a positive rate of 94% in WT. The positive rate in benign tumors other than WT is only 8%; thus, suggesting that this test is specific to WT. The present study found good sensitivity and specificity of Tc-99m in WT.
Taken together, the above findings suggest that more than 90% of parotid tumors can be correctly diagnosed preoperatively as WT by combining FNAC and Tc-99m scintigraphy. In addition, the preoperative diagnosis rate may improve by including the typical characteristics of WT, such as advanced age, male sex, lower pole location, and bilaterality.
In theory, if WT is found to require less invasive surgery and to have fewer postoperative complications compared with PA, surgical treatment may be seen as the best treatment approach. However, we saw no evidence to support that kind of treatment strategy. Rather, because WT is more common in advanced age people and can be accompanied by systemic complications at a constant rate, an observation-only strategy is preferable in many patients. Although a reliable preoperative histological diagnosis of WT is necessary when deciding to manage a patient by observation only, this study demonstrated that this approach is nevertheless feasible in the majority of cases. If WT can be reliably diagnosed by histology, the observation approach becomes a viable option, although aesthetic issues may remain. In the future, the indication of extracapsular dissection, a less invasive operative method, may be expanded to include WT because WT commonly occurs in the lower pole and recurrence is rare 18 ; however, this procedure also requires a reliable preoperative histological diagnosis.
One limitation of this study was the handling of observation cases because patients with WT that were either confirmed or suspected on the basis of FNAC or Tc-99m scintigraphy were considered as having WT. The correct diagnosis rate of WT by FNAC is about 90%, and the false-positive rate of Tc-99m scintigraphy is about 20%. Therefore, this group may have included about 10% of histological types other than WT. However, because the characteristic findings of WT were also used as the basis for the diagnosis, we believe that misdiagnosis was likely limited to a small percent of patients. Another limitation is that observation cases were followed up by outpatient visits for about 1 year after the decision was made to take the observation approach. However, few patients continued to visit our hospital after that time. Some of these patients may have received surgery at other hospitals, depending on the subsequent course of their condition.
Conclusion
In patients with WT, 238 underwent surgery, and 149 were managed by observation. Among the 238 patients confirmed by the final pathology to have WT, 170 (71.4%) were diagnosed with WT preoperatively by FNAC. The positive rate of Tc-99m scintigraphy in WT was 75.4%. Combining FNAC and Tc-99m scintigraphy, as well as considering clinical findings, enables the diagnosis of WT in most cases. If a reliable histological diagnosis can be made preoperatively for WT, managing patients by observation may be a viable approach, in particular because WT is more common in older adults and rarely undergoes malignant transformation.
Footnotes
Author Contributions
Ryo Kawata designed and supervised the study. Hiromi Nishimura, Ichita Kinoshita, and Ryo Kawata wrote the manuscript. Masaaki Higashino, Tetsuya Terada, and Shin-Ichi Haginomori acquired all clinical data. Takeshi Tochizawa and Ichita Kinoshita assisted in the statistical analyses. All authors performed data analysis and interpretation and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by our Institutional Review Board (approval no. #2621-1, 2020).
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Date Availability
Data available on request due to privacy/ethical restrictions.