
Abstract
Importance
The clinical significance of oncocytes in thyroid aspirate is uncertain, leading to inconsistent and possible over-treatment.
Objective
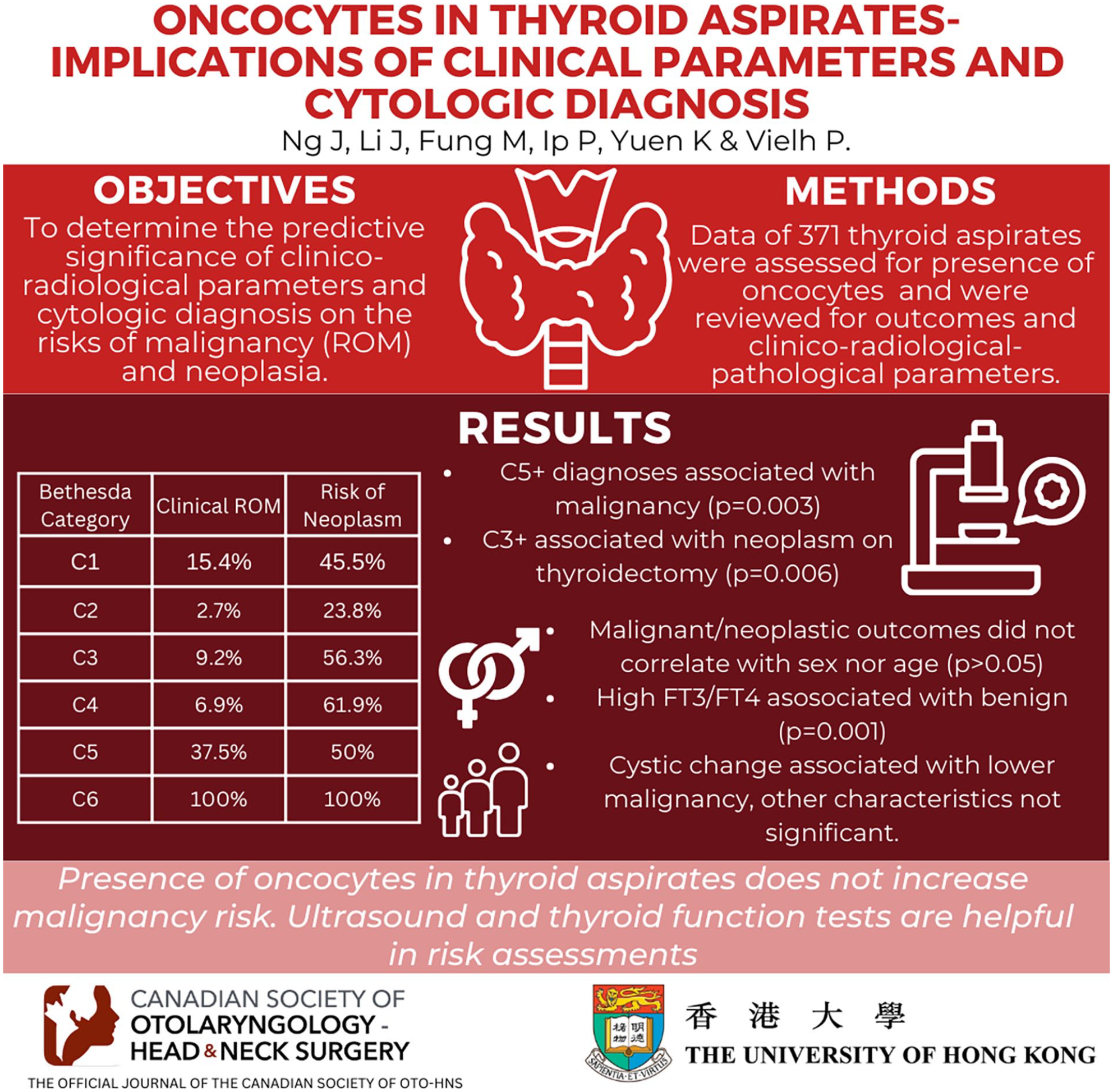
To determine the predictive significance of clinico-radiological parameters and cytologic diagnosis on the risks of malignancy (ROM) and neoplasia.
Design
Data of thyroid aspirates with the presence of oncocytes were reviewed for outcomes and clinical-radiological-pathological parameters.
Setting
Three regional institutes performing thyroid surgery and investigations.
Participants
From a population base of 1.3 million across a 9-year period, totaling 371 aspirates with oncocytes with an 85.0-month average follow-up.
Intervention
Fine-needle aspiration of thyroid.
Results
On clinical follow-up, the ROM for Bethesda categories C1-C6 was 15.4%/2.7%/9.2%/6.9%/37.5%/100%, while the risk of neoplasm (considering thyroidectomy follow-up) was 45.5%/23.8%/56.3%/61.9%/50%/100%, including 52 oncocytic follicular lesions (4 carcinomas and 48 adenomas) and 26 other carcinomas/malignancies. C5+ diagnoses were associated with malignancy (P = .003), and C3+ was associated with neoplasm on thyroidectomy (P = .006). Malignant/neoplastic outcomes did not correlate with sex or age (P > .05). High free triiodothyronine/free thyroxine levels were associated with a benign clinical outcome (P = .001). Cystic change on ultrasound was associated with a lower malignancy (P = .012) and neoplasm risk (P = .041). Lesion size, echogenicity, vascularity, multinodularity, lymphadenopathy, and solid areas on ultrasound were not significant in predicting malignancy or neoplasm (P > .05).
Conclusion
The presence of oncocytes in thyroid aspirates does not increase malignancy risk. Most malignant oncocytic thyroid aspirates are not attributable to oncocytic carcinomas but papillary thyroid carcinomas. Ultrasound and thyroid function tests are helpful in the risk assessment of these cases.
Relevance
For treatment or follow-up decisions in patients with oncocytes in thyroid aspirates.
Key Messages
The presence of oncocytes in thyroid aspirates does not increase malignancy risk.
Most malignant oncocytic thyroid aspirates are not attributable to oncocytic carcinomas but papillary thyroid carcinomas.
Ultrasound and thyroid function tests are helpful in preoperative risk assessment.
Introduction
The presence of oncocytes in a thyroid aspirate can be indicative of not only malignant or neoplastic lesions but also reactive changes or incidental findings. Although studies have confirmed that thyroid aspirates containing oncocytes are not associated with an increased risk of malignancy (ROM),1-3 most available data are limited to intermediate/neoplastic (atypia of undetermined significance, follicular neoplasm or suspicious for malignancy) cytologic diagnostic categories or only included cases with thyroidectomy confirmation.1,2,4 Cases with benign thyroid aspirates are underrepresented in studies as clinical follow-up is preferred and thyroidectomy is less often indicated or performed. This study reviews the clinical and histological outcome of a large cohort of thyroid aspirates with oncocytes, inclusive of benign aspirates and patients without thyroidectomy, with respect to clinical and radiological parameters. Findings will be useful in confirming the benignity of benign or unsatisfactory aspirates with oncocytes and identifying useful clinical and radiological parameters in supplementing the ROM and neoplasia assessment.
Methodology
Computerized searches of the pathology archives in 3 of the involved institutions (AHNH, NDH, and PWH) were performed, retrieving all consecutive thyroid aspirates with a microscopic description and/or diagnosis indicating the presence of oncocytes, from the period 2011 to 2019. Reports were reviewed for confirmation, and cytologic diagnoses were arranged into 6 categories according to the Bethesda System for Reporting Thyroid Cytopathology 2023, 5 namely:
Nondiagnostic or unsatisfactory: C1
Benign: C2
Atypia of undetermined significance: C3
Follicular neoplasm or oncocytic follicular neoplasm: C4
Suspicious for malignancy: C5
Malignant: C6
Patient records were reviewed for clinical, radiological, and pathological data. Clinical data retrieved included patient demographics, follow-up duration, and thyroid function tests taken within 12 months of fine-needle aspiration, and not taken after thyroidectomy; for radiological data, ultrasound reports at aspiration. Reports of corresponding thyroidectomy specimens were reviewed for histologic diagnosis. In cases without a definite diagnosis (ie, descriptive or differential diagnoses), aspiration cytology and/or thyroidectomy histology were reviewed. The histologic diagnosis of thyroidectomy, correlated with location and laterality, was considered as a reference for cases with a corresponding thyroidectomy. Cases without further thyroidectomy performed were considered as having a clinically benign outcome if subsequent follow-up for 12 months was uneventful. Cases with less than 12 months of clinical follow-up and no histology were excluded.
Thyroid carcinomas (anaplastic, follicular, oncocytic, medullary, papillary, and poorly differentiated carcinomas) and other malignancies, including lymphomas, were considered a malignant diagnosis for the calculation of ROM. In addition to malignant lesions, non-carcinomatous lesions, including thyroid adenomas (follicular and oncocytic adenomas) and borderline lesions (noninvasive follicular thyroid neoplasm with papillary-like nuclear features and well-differentiated thyroid tumor of uncertain malignant potential) were included as thyroid neoplasms.
Statistical Analysis
Statistical analysis was performed using SPSS statistical software (Windows version 23, IBM, USA). Results of thyroid function tests were classified into low, normal, and high based on local reference ranges. Cases with benign clinical outcomes were included for the calculation of ROM, while only cases with thyroidectomy performed were used as the denominator for neoplasia. The Chi-squared test (or Fisher’s exact test as appropriate) and t-test were used to compare outcomes and clinicopathological parameters as categorical and continuous variables. A P-value of <.05 was considered significant.
Results
Out of a total of 384 aspirates retrieved, 13 were excluded due to insufficient follow-up duration. No cytologic or histologic diagnosis was changed after the review of the slides. Of the 371 aspirates included for analysis, 55 were from male patients and 316 were from female patients, with an average age of 55.1 years. The average follow-up duration of the cohort was 85.0 months. There were 30, 147, and 194 with malignant histological, benign histological, and benign clinical follow-up, respectively (Figure 1, Table 1).

Case collection.
Demographics of the Cohort.
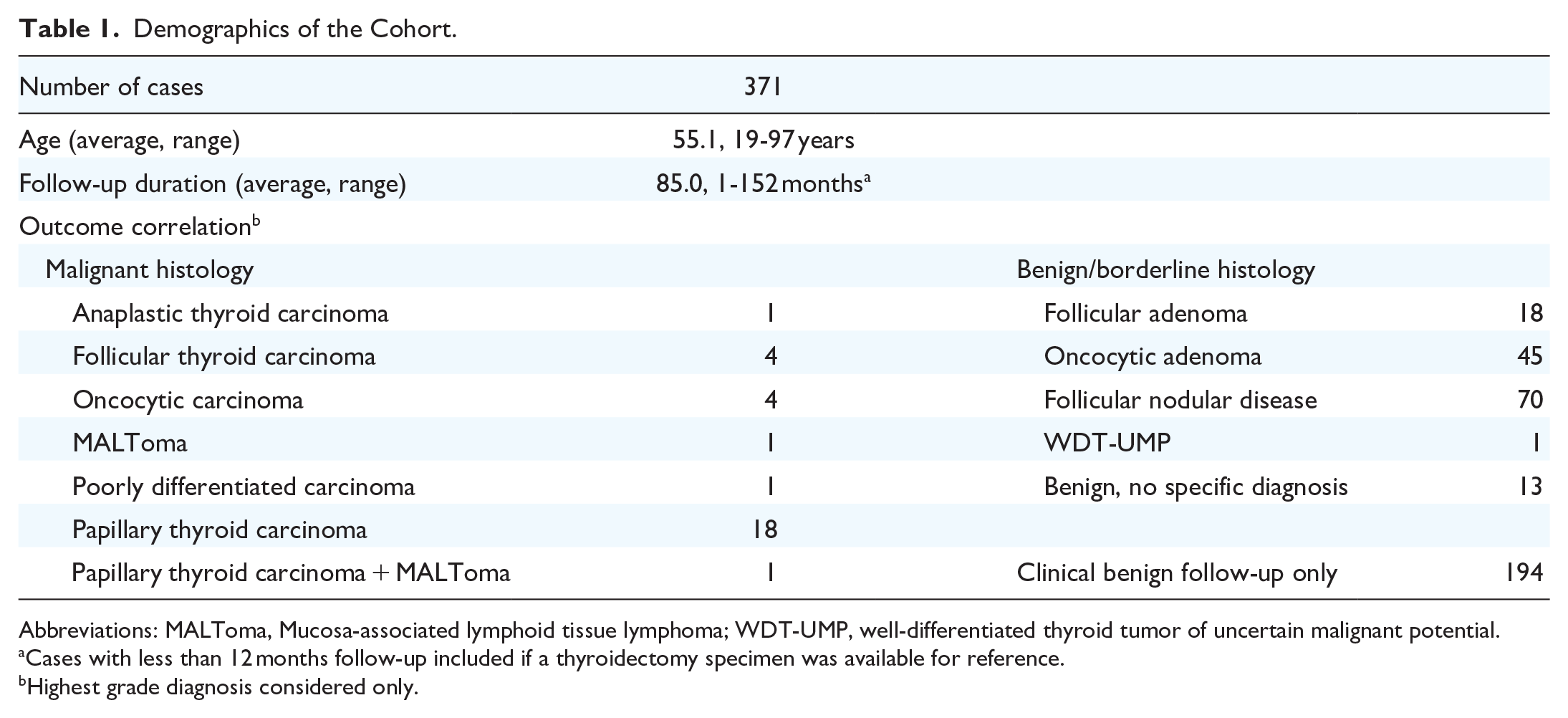
Abbreviations: MALToma, Mucosa-associated lymphoid tissue lymphoma; WDT-UMP, well-differentiated thyroid tumor of uncertain malignant potential.
Cases with less than 12 months follow-up included if a thyroidectomy specimen was available for reference.
Highest grade diagnosis considered only.
The ROMs for the C1 to C6 categories were 15.4%, 2.7%, 9.2%, 6.9%, 37.5%, and 100% respectively, whereas the percentages of cases with thyroid neoplasms for the C1 to C6 categories were 45.5%, 23.8%, 56.3%, 61.9%, 50%, and 100%, respectively. There was a total of 52 oncocytic neoplasms comprising 4 oncocytic carcinomas and 48 oncocytic adenomas, in which 3 cases of oncocytic adenoma presented with concurrent papillary thyroid carcinoma. C4 (40.5%) and C3 (31.3%) with oncocytic aspirates carried the highest risk of oncocytic neoplasm, followed by C1 (18.2%) and C2 (14.35%) aspirates. Neither C5 nor C6 aspirate corresponded to an oncocytic follicular neoplasm on thyroidectomy (Table 2). Diagnoses of C5 or above were strongly associated with a malignant diagnosis (P = .003), whereas diagnoses of C3 or above were strongly associated with a neoplasm (inclusive of carcinomas, lymphomas, borderline neoplasms, and benign adenomas) on thyroidectomy (P = .006) (Table 3).
ROM and RON.

Abbreviations: AUS, atypia of undetermined significance; FN, follicular neoplasm; ND, nondiagnostic; ROM, risk of malignancy; RON, risk of neoplasm; SFM, suspicious for malignancy.
Included cases of oncocytic cell adenoma with concurrent malignant diagnoses.
Correlation Between Bethesda Diagnostic Category and Outcome.

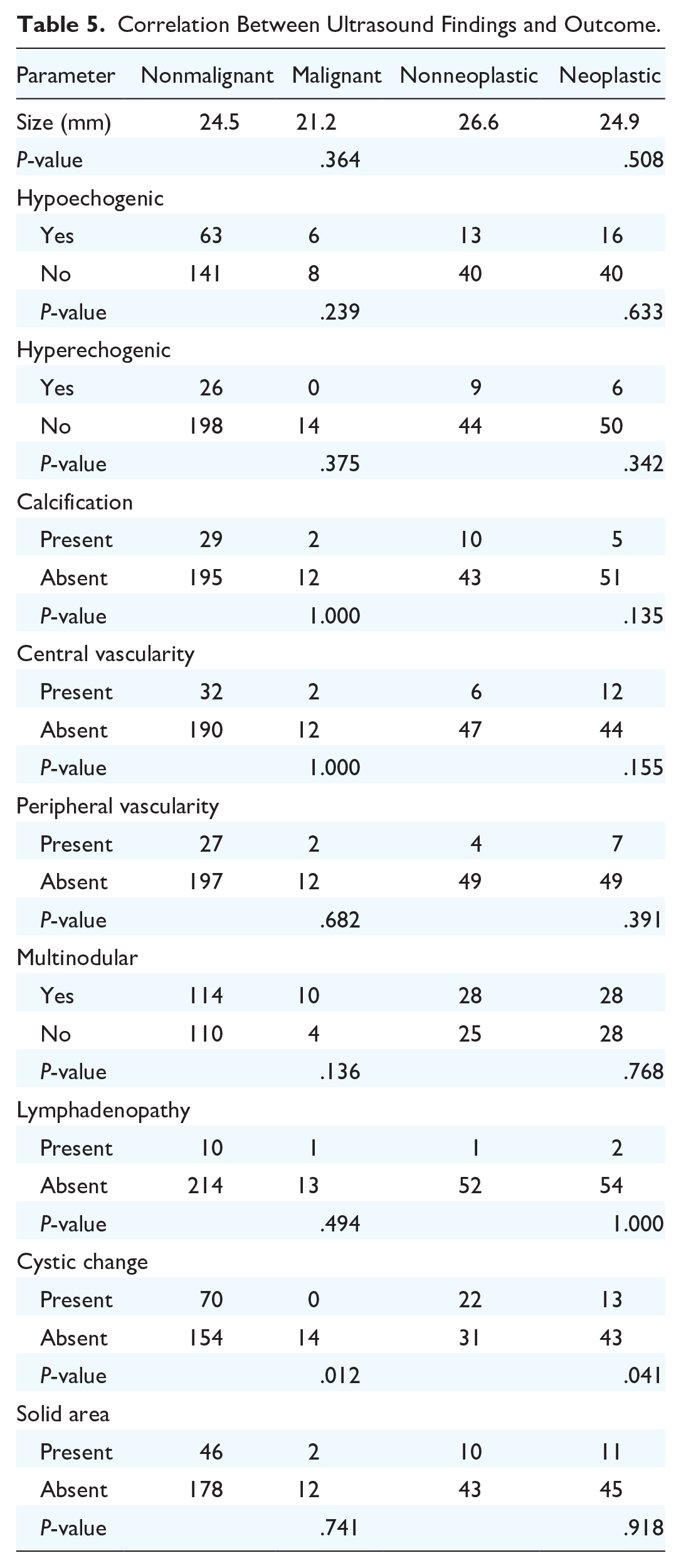
There were no correlations found between malignancy/neoplasm and sex or age (P > .05). A high free triiodothyronine (FT3) or free thyroxine (FT4) level was associated with a benign outcome (P = .001) (Table 4). For ultrasound findings, lesion size, echogenicity (hyper- and hypoechogenicity), vascularity, multinodularity, and lymphadenopathy were not associated with outcome (P > .05), but the presence of cystic changes was associated with a lower ROM (P = .012) and neoplasm (P = .041). The presence of solid areas on ultrasound did not correlate with outcome (P > .05) (Table 5).
Correlation Between Patient Characteristics and Outcome.

FT3, free triiodothyronine; FT4, free thyroxine.
Correlation Between Ultrasound Findings and Outcome.
Discussion
The presence of oncocytes in a thyroid aspirate is associated with a variety of conditions. Oncocytes are not only seen in oncocytic neoplasms but also in other conditions, including Graves’ disease, lymphocytic thyroiditis, and following local irradiation. 3 The significance of oncocytes in thyroid aspirates is an area of controversy. There is evidence supporting that the presence of oncocytes does not increase the ROM.1-3 However, cohorts reported in the literature are often limited to either the C3 or C4 categories or only include cases with eventual thyroidectomy.1,2,4 The C1 and C2 categories and clinically benign cases are underrepresented, either when the oncocytes on the aspirate were of small quantity or of a benign impression, or when the clinical index of suspicion was low, thus thyroidectomy was not warranted.
As there are clinicians who consider oncocytes as an “atypical” diagnosis, 2 and also a possible predisposition for cytopathologists in issuing a C3 or C4 diagnosis when oncocytes are identified, 6 it is important to clarify the risks and prognosis of each Bethesda diagnostic category. An accurate assessment of the overall ROM for thyroid aspirates with oncocytes, particularly those of C1 and C2 categories, requires the inclusion of clinically benign cases with adequate follow-up. Hence, this study recruited cases from the previous decade with an average follow-up period of more than 7 years. Inclusion of cases with clinical outcomes potentially overlooks microcarcinomas that may only be detectable on thyroidectomy, but with a lengthy follow-up duration, such errors should have been minimized.
The ROMs of the C1, C2, and C6 categories were comparable with the reference range from the Bethesda system,7,8 and the false negative diagnosis correlated to either small papillary thyroid carcinomas (<1 cm) or follicular/oncocytic carcinomas. The difference in ROM of C5 (37.5%, reference: 67%-83%) may be attributed to a small sample size (n = 8). As for the C3 and C4 categories, the clinical ROMs in the current cohort were 9.2% and 6.9% respectively, lower than the reference ranges of 13% to 30% and 23% to 34%, 7 but normalizing to 14.6% (C3) and 11.9% (C4) when cases with only clinical follow-up were excluded, reflecting the discrepancy between clinical and histological follow-up.9,10 Inclusion of cases with long and reliable clinical outcomes will give ROMs greater clinical relevance. The current cohort demonstrated that the ROMs of oncocytic aspirates were either comparable or lower across all Bethesda categories, indicating that the presence of oncocytes in thyroid aspirates itself should not heighten the suspicion of malignancy, whereas thyroid function test results and radiological findings were more useful in predicting malignancy. Of note, the RON of C1, C3, and C4 categories were high (45.5%-61.9%), which is a factor in consideration of surgical intervention other than malignancy risk.
The cases with a C5 or C6 corresponding to malignant histology were all papillary thyroid carcinomas on thyroidectomy. The nuclear features of papillary thyroid carcinoma are consistently reproducible on aspiration cytology, 11 allowing for accurate diagnosis. These cases in the current cohort, and similar cases in the available literature, include papillary thyroid carcinomas with oncocytic change, background thyroiditis, or concurrent oncocytic neoplasms. 12 As for oncocytic carcinomas, the 4 cases in the cohort were diagnosed as C1, C2, C3, and C4, respectively. The C1 and C2 diagnoses were likely attributable to sampling and adequacy issues. The other diagnoses correspond to the literature reporting that oncocytic adenomas and carcinomas were most commonly diagnosed as C3 and C4. 13 Akin to classical follicular neoplasms, the differentiation between oncocytic adenomas and carcinomas is not possible solely based on aspiration cytology, 14 and data from this cohort reflect that the majority of malignant cytologic and histologic diagnoses in aspirates with oncocytes are attributed to non-oncocytic neoplasms.
Clinical and radiological parameters are predictive of the final outcome and are often incorporated for clinical risk assessment. 15 Parameters commonly referenced include patient demographics, lesion size and appearance on ultrasound (which often accompanies fine-needle aspiration), and thyroid function test results for the thyroidal lesions.16,17 Giorgadze et al, in a cohort of oncocytic neoplasms, found that greater lesion size and older age increase the ROM. 16 These associations were also seen in larger cohorts not limited to oncocytic neoplasms. 18 The current cohort demonstrates that a high FT3 and/or FT4 level was associated with a benign outcome, in line with the adage that “hot” thyroid nodules are mostly indolent. 19 Cystic change on ultrasound was the only parameter that demonstrated significant association with both malignancy and neoplasia, with its presence favoring a benign and nonneoplastic lesion. This association is also reported in radiological correlational studies.20,21 However, cystic malignant lesions of the neck and thyroid can be a pitfall,22,23 and the entire clinical picture should be taken into consideration for risk assessment in thyroid diseases.
Conclusion
The ROM of thyroid aspirates with oncocytic features for the C1 (15.4%) and C2 (2.7%) categories are comparable while those of the C3 (9.2%) and C4 (6.9%) categories are low compared with general thyroid aspirates in the Bethesda system, supporting that oncocytes per se do not indicate suspicion. However, thyroid neoplasms are found in follow-up of a high percentage of oncocytic aspirates (C3—56.3%, C4—61.9%). Cytologically malignant oncocytic aspirates are likely to represent papillary thyroid carcinomas with oncocytic changes, concurrent oncocytic neoplasms, or thyroiditis, but not oncocytic carcinomas. A high FT3 and/or FT4 level is associated with benignity, and cystic changes present on ultrasound indicate a lower ROM and neoplasm.
Footnotes
Author Contributions
JKMN: conceptualization, data curation, investigation, methodology. JJXL: conceptualization, investigation, methodology, visualization, writing—original draft. MMHF: validation. KKWY: validation. PPCI: writing—review and editing. PV: methodology, validation, writing—review and editing.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Ethics
The study was approved by the Joint Chinese University of Hong Kong—New Territories East Cluster Clinical Research Ethics Committee (2022.053).