
Abstract
Keywords
Introduction
Salivary gland tumors account for 3% to 10% of head and neck tumors with a predicted incidence rate of 0.4 to 13.5 new cases in 100,000 population.1,2 Salivary gland neoplasms are characterized by a wide range of histopathological diversity and various types of lesions, including benign and malignant tumors and non-neoplastic diseases. 3 The parotid gland is the largest in this system and contains 75% to 80% of salivary tissues. 4 Parotid tumors commonly represent benign neoplasms, while the potential for malignancy increases in others, such as the submandibular and minor salivary glands. 5 These tumors typically present with a mass located in the preauricular or retromandibular region. 6
The accurate diagnosis of tumors located in the parotid gland is crucial to determine the appropriate treatment strategies and prognosis for patients. There are various cytopathological diagnostic tools available to clinicians, while fine needle aspiration cytology (FNAC) and frozen section (FS) are the primary preferred modalities for evaluating parotid gland tumors in current practice. 7
FNAC is a minimally invasive and rapid diagnostic procedure used to investigate cell groups, cellular materials, and the microstructure of tissues. 8 It is commonly preferred due to its simplicity, safety, and cost-effectiveness. 9 However, there are clinical implications related to its sensitivity, especially in distinguishing between benign and malignant neoplasms. 10 Some authors suggest parotidectomy for the diagnosis and treatment of all cases due to false-positive and false-negative results.11-13 However, some still require FNAC to determine benign or malignant lesions prior to surgery, as the surgical approach varies.14,15
FS is a more invasive and resource-incentive technique conducted intraoperatively. FS provides immediate feedback and improves the surgeon’s decision-making process. 16 Some authors rely on intraoperative FS, while others prefer to wait for permanent histopathology. The latter approach can necessitate subsequent surgery if the final histopathological findings suggest the need for a total parotidectomy, neck dissection, or a different adjustment in the surgical procedure.
The purpose of this study is to present detailed documentation of the 7-year results of FNAC, FS, and permanent histopathologies in our tertiary care hospital. Additionally, our objective is to evaluate the diagnostic capabilities of FNAC and FS by measuring their sensitivity, specificity, accuracy, and positive and negative predictive values. Furthermore, we will provide the true-positive, true-negative, false-positive, and false-negative results of FNAC.
Materials and Methods
Ethical Approval
The Clinical Research Ethics Committee approved this research, decision number 2019-18/15, on October 30, 2019.
Study Design and Patient Selection
This study is a retrospective analysis of patients who presented with parotid masses in the Department of Otorhinolaryngology of our hospital from January 2013 to 2019. Patients of all age groups who underwent parotidectomy in the institution were included. However, those with recurrent parotid neoplasms requiring revision surgery and those with local tumors invading the parotid or metastases to the parotid from distant sites were excluded.
Data Collection and Analysis
The medical records were retrospectively reviewed to obtain preoperative FNAC and intraoperative FS data. These were compared with permanent histopathological results after parotidectomy to obtain the diagnostic metrics of each test, such as sensitivity, specificity, accuracy, and positive and negative predictive values. Preoperative cytological reports that describe the subtypes of the lesion compared with histopathological results and the true-positive, true-negative, false-positive, and false-negative values of FNAC were achieved. Also, demographic information, such as age and sex, was collected.
Pathological Evaluation
FNAC samples and permanent histopathological sections were examined by a pathologist with more than 10 years of experience in pathology specializing in the head and neck area at our university hospital. Experienced pathologists also conducted FS evaluations in our institution’s operating theater frozen unit. We performed routine FNAC for every patient with a parotid gland mass. In cases where the FNAC results were inconclusive, we preferred to perform FS. Salivary gland FNAC smears were stained with May Grünwald Giemsa at the Department of Pathology and then evaluated. The samples received by the frozen unit were frozen at −35°C in a cryotome FS Thermo Scientific device, cut into 7-µm sections, stained with hematoxylin and eosin (H&E), and then evaluated. Permanent histopathological preparations were fixed in a 10% formalin solution, followed by routine tissue processing and H&E staining.
Categorization of FNAC and FS Results
FNAC results were classified into 3 groups: benign, malignant, and non-diagnostic. With the introduction of the Milan system, they were re-categorized: non-diagnostic, non-neoplastic, atypia of undetermined significance, benign neoplasm, neoplasm of uncertain malignant potential, suspicious for malignancy, and malignancy. The benign group comprised non-neoplastic, atypia of undetermined significance, and benign neoplasms, whereas neoplasms of uncertain malignant potential, suspicious for malignancy, and malignancy were categorized under the malignant group. Within the FNAC results, only those benign neoplasms and malignancies with reported histopathological subtypes are specifically noted. FS were classified into 3 groups: benign, malignant, and suspicious for malignancy. During the diagnostic analysis of FS, cases reported as suspicious for malignancy were excluded because the inability to definitively categorize them as benign or malignant neoplasm during intraoperative time did not change the extent of the surgical practice.
Statistical Analyses
The normal distribution of variables was tested using the Shapiro-Wilk test. For variables that did not follow a normal distribution, median values (minimum-maximum) were used to describe them. Categorical variables were shown as frequencies and percentages. The McNemar test was applied to compare categorical variables among dependent groups. To evaluate diagnostic performance, sensitivity, specificity, positive predictive value, negative predictive value, and accuracy statistics were calculated. A significance level of α = .05 was used. The statistical analyses were performed using IBM SPSS Statistics software, version 22.0.
Results
Overview of Parotidectomy Cases and Demographic Structure
During research, our institution performed 289 parotidectomies, including 22 cases with invasion of surrounding tissue or metastasis to the parotid from local or distant areas and 2 cases of recurrence. Therefore, we reviewed the medical records of 265 patients who underwent parotidectomy for primary parotid tumors and analyzed 246 FNAC and 67 FS reports.
The sex distribution in our study group comprised 153 (57.7%) male and 112 (42.3%) female participants. Age characteristics were as follows: male patients ranged between 13 and 92 years with a median age of 55, whereas female patients ranged from 17 to 81 years with a median age of 51.
FNAC and FS Associated Results
Cytological data were classified according to the Milan system. The distribution was as follows: 14 non-diagnostic (5.7%), 51 non-neoplastic (20.7%), 4 atypia of undetermined significance (1.6%), 139 benign neoplasms (56.5%), 6 atypia with uncertain potential for malignancy (2.5%), 14 suspicious for malignancy (5.7%), and 18 malignant (7.3%).
When evaluating the identified pathology results within the 246 FNAC, definitive cytopathological results were present in 152 cases (61.7%). This included 139 patients (100%) with benign neoplasms and 13 out of the 18 patients (72.2%) with malignancies.
When reviewing FS records, it was observed that 67 patients underwent intraoperative frozen section analysis. Of these, 37 patients were found to have benign neoplasm (55.2%), 27 patients had malignant neoplasm (40.3%), and 3 cases were classified as suspicious for malignancy (4.5%).
Post-Parotidectomy Permanent Histopathological Data
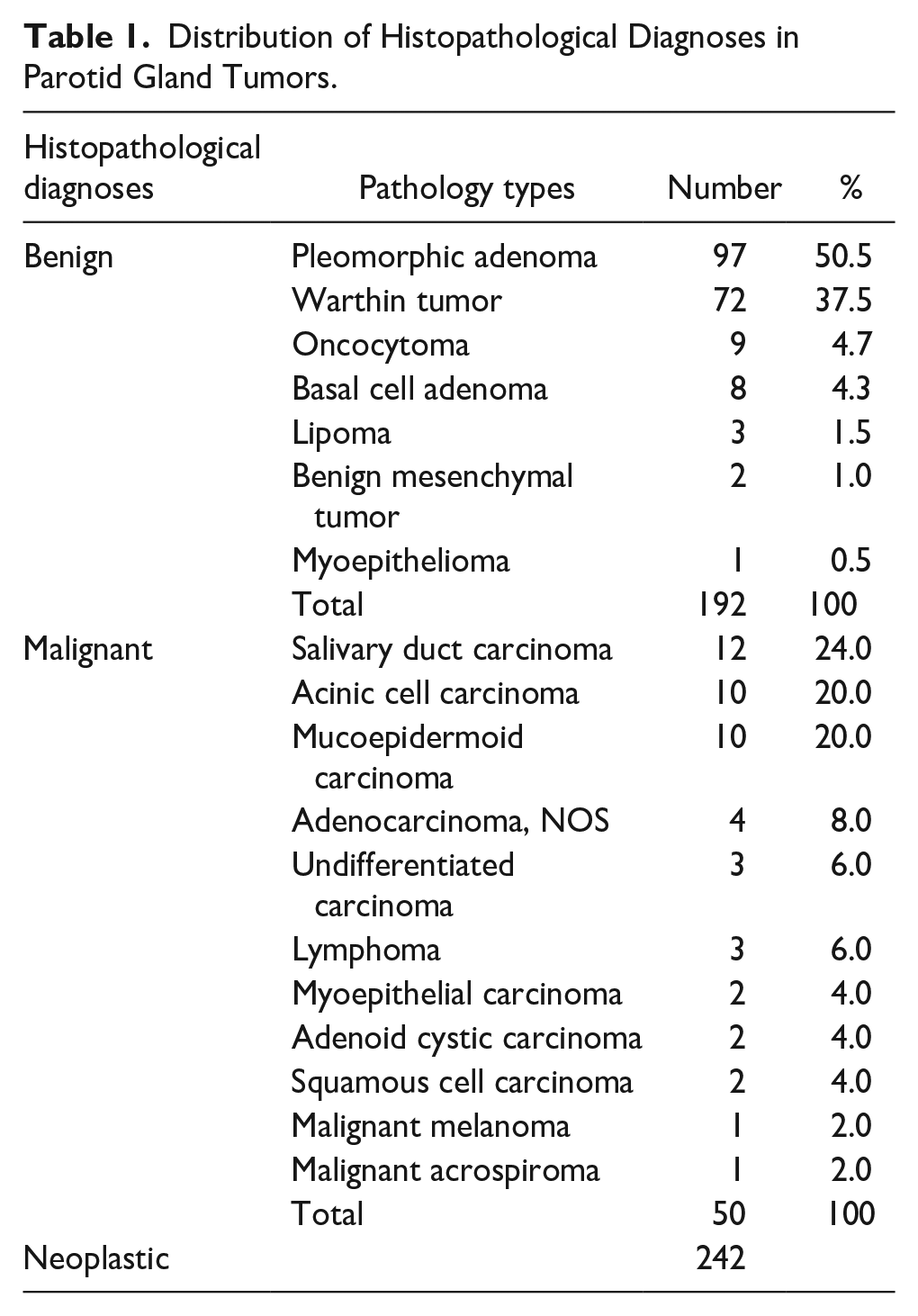
Upon reviewing the permanent histopathological results of 265 patients, 242 were found to be neoplastic (91.3%), and 23 were non-neoplastic (8.7%). Of the neoplastic cases, 192 were diagnosed as benign neoplasms (79.3%) and 50 as malignant neoplasms (20.7%). The most common benign neoplasm was pleomorphic adenoma, accounting for 97 cases (50.5%), followed by 72 cases (37.5%) of Warthin tumor. The distribution within the 50 malignant tumors in terms of the most frequently observed types, it was noted that there were 12 cases of salivary duct carcinoma (24%), 10 cases of acinic cell carcinoma (20%), and 10 cases of mucoepidermoid carcinoma (20%). The neoplastic tumors found in our parotidectomies are listed in Table 1.
Distribution of Histopathological Diagnoses in Parotid Gland Tumors.
Comparison of FNAC and Permanent Histopathology Results
After excluding 14 non-diagnostic FNAC cases, we conducted an analysis with 230 FNAC reports to compare the FNAC with histopathology. There were 187 cases of benign neoplasms and 43 cases of malignant neoplasms. Among the 43 cases confirmed as histopathologically malignant, 28 (65.1%) were identified as malignant and 15 (34.9%) as benign by FNAC. Out of the 187 cases confirmed as benign, the FNAC data showed 176 (94.1%) as benign and 11 (5.9%) as malignant.
Thus, the sensitivity of FNAC in achieving malignant permanent histopathological results was determined to be 65.1%, specificity 94.1%, accuracy 88.7%, positive predictive value 77.1%, and negative predictive value 92.1%. FNAC and histopathology results are listed in Table 2, and the frequencies of the risk of neoplasia and malignancy are presented in Table 3.
Correlation Between FNAC and Final Histopathological Diagnoses.
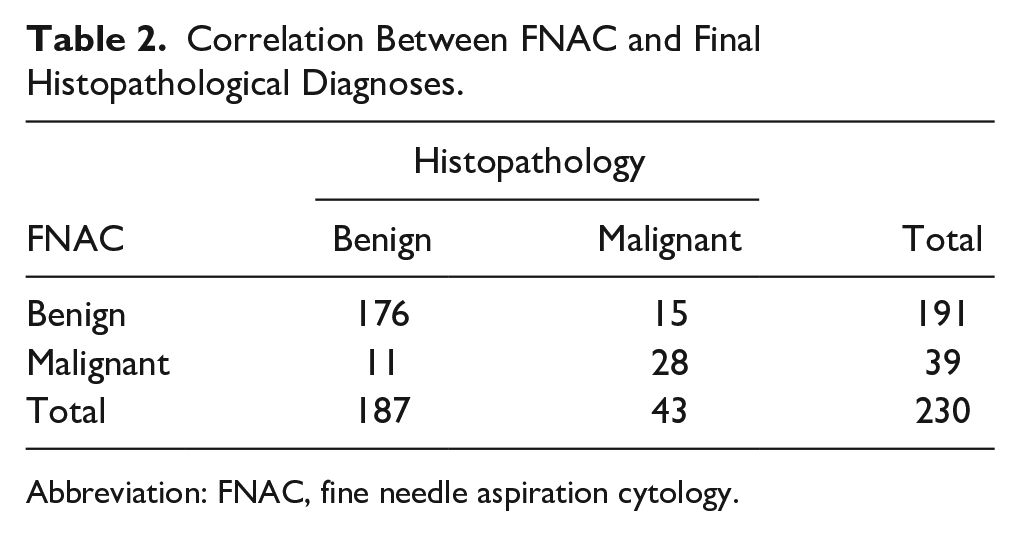
Abbreviation: FNAC, fine needle aspiration cytology.
RON and ROM According to the MSRSGC.
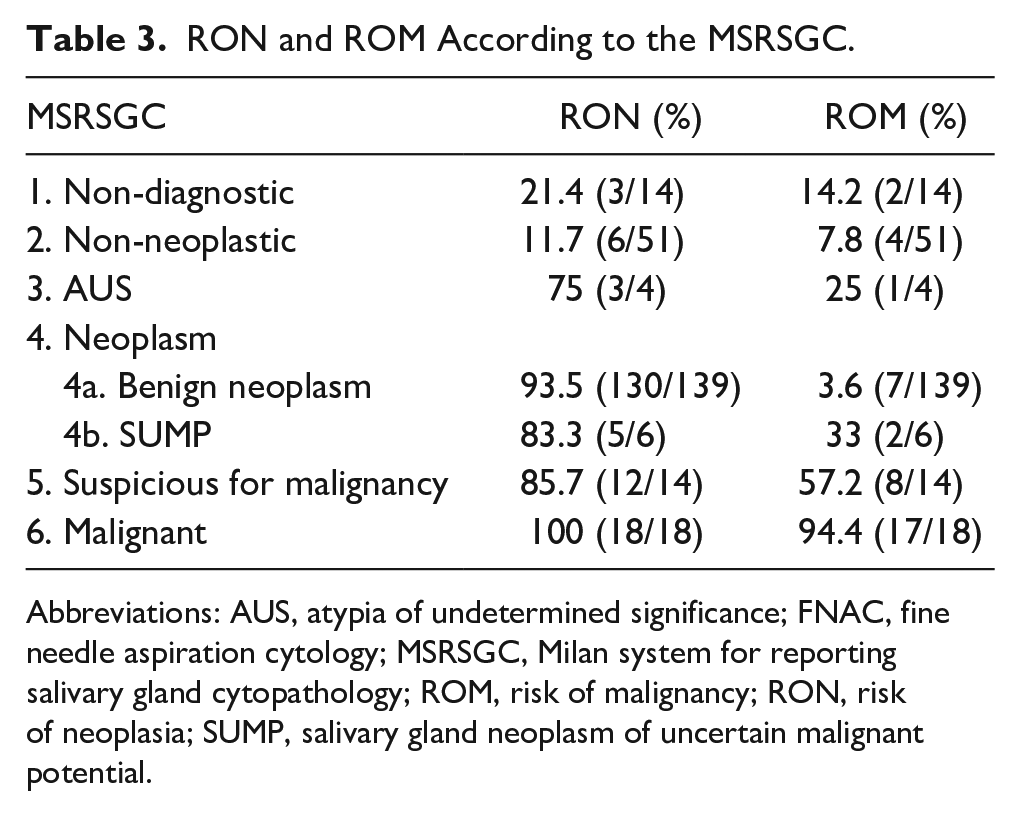
Abbreviations: AUS, atypia of undetermined significance; FNAC, fine needle aspiration cytology; MSRSGC, Milan system for reporting salivary gland cytopathology; ROM, risk of malignancy; RON, risk of neoplasia; SUMP, salivary gland neoplasm of uncertain malignant potential.
Comparison of Intraoperative FS and Permanent Histopathology Results
When comparing intraoperative frozen sections with permanent histopathology, among the 30 cases known to be histopathologically malignant, 26 (86.6%) were identified as malignant, 2 (6.6%) as benign, and 2 (6.6%) as suspicious for malignancy according to FS analysis. Of the 37 cases known to be benign, 35 (94.6%) were identified as benign, 1 (2.8%) as malignant, and 1 (2.8%) as suspicious of malignancy during FS analysis. After excluding 3 suspicious malignancies, FS and histopathology results are listed in Table 4.
Correlation Between FS and Histopathological Diagnoses.
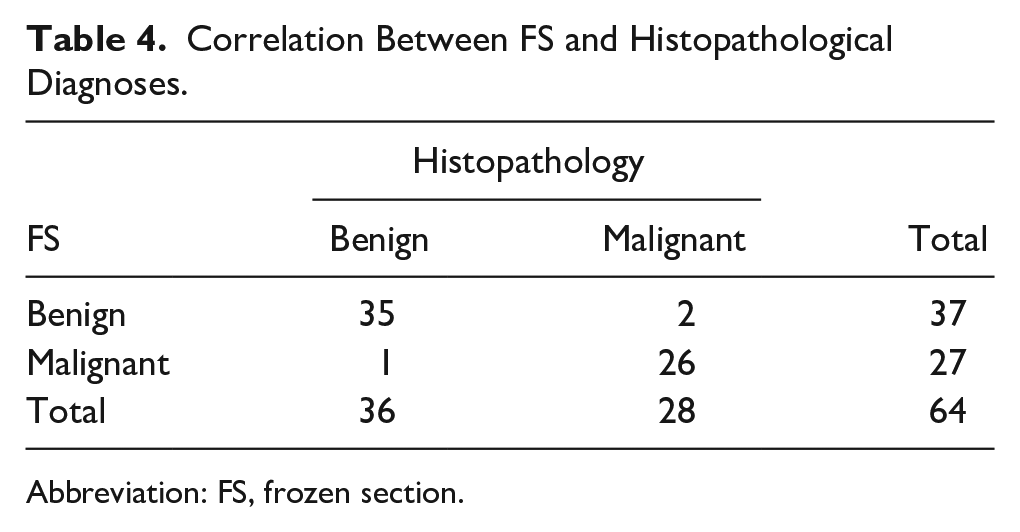
Abbreviation: FS, frozen section.
Thus, the sensitivity of FS in achieving malignant permanent histopathological results was determined to be 92.9%, specificity 97.2%, accuracy 95.3%, positive predictive value 96.3%, and negative predictive value 94.6%.
Detailed Documentation of False-Positive and False-Negative Results of FNAC
False-positive and false-negative FNAC cases are presented in Table 5.
Presentation of False-Positive and False-Negative FNAC Results.
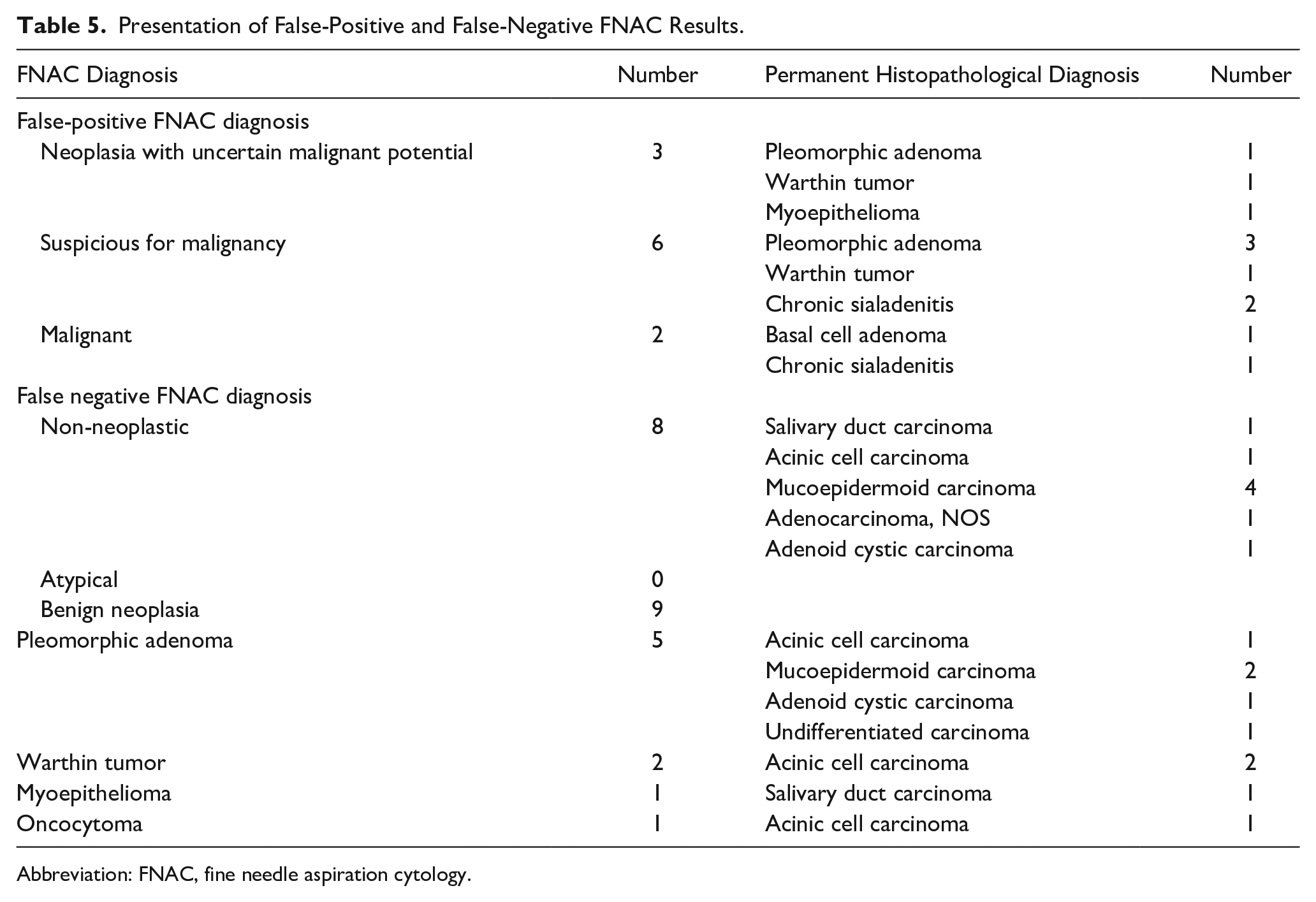
Abbreviation: FNAC, fine needle aspiration cytology.
Discussion
This study presents a comprehensive comparison between 2 methods for diagnosing tumors in the parotid gland: FNAC and FS. Our findings indicate significant differences in the diagnostic capabilities of these 2 methods, which have important implications for clinical decision-making and patient management.
FNAC is an important method used to diagnose head and neck lesions in the preoperative period. It is often preferred as an initial diagnostic method for salivary gland lesions. However, interpreting cytomorphological features can be challenging, especially when dealing with tumors that exhibit diverse morphologies and metaplasia. It has shown that FNAC has a sensitivity of 60% to 100% and a specificity of 86% to 100%12,17,18 in diagnosing salivary gland masses. According to some authors, preoperative FNAC is unnecessary due to false-positive and false-negative results and the treatment of parotid masses being surgical in all cases. 19 However, many investigators advocate the necessity of FNAC because the surgical approach of benign and malignant parotid masses is not the same.15,20
FNAC errors can be categorized into 4 steps. The first is a sampling from a non-tumorous area during the aspiration phase, and the second involves triage errors by the pathologist, followed by issues related to the nature of the cytological material, such as hypocellularity, and finally, interpretation errors. 21 Two main types of lesions pose significant challenges: cystic tumors and hypercellular tumors. Cystic or necrotic tumors often produce an abundance of poorly cellular cytological material, making reliable analysis difficult. Conversely, like lymphomas, hypercellular tumors generate plentiful cytological material consisting of small round cells with minimal morphological features, which complicates the diagnostic process. 22
Various factors and circumstances influence the choice between FNAC and FS in the diagnostic process. Each method highlights several strengths and limitations. FNAC is known for being minimally invasive and comfortable for patients; however, it showed lower sensitivity but higher specificity in both the literature and our study. This finding is consistent with the known limitations of FNAC, particularly in distinguishing between malignant and benign lesions. On the other hand, FS demonstrated higher accuracy in real-time surgical decision-making, although its invasive nature and resource requirements present practical challenges. 23
Among the true negative cases with non-neoplastic FNAC reports, a significant number were identified as Warthin tumor, followed by oncocytoma. Lesions containing oncocytes, such as oncocytoma and Warthin tumor, can be mistaken for inflammatory or reactive changes, leading to their interpretation as non-neoplastic. Additionally, the lymphoid component of Warthin tumor can be confused with an inflammatory process. Similarly, reactive changes in oncocytes can also be misinterpreted as a non-neoplastic process. Myoepithelioma has been reported in 2 cases in FNAC, even though it is diagnosed as pleomorphic adenoma in the final histopathology. This is because both myoepithelioma and pleomorphic adenoma can have similar cell types like myoepithelial and ductal cells in their structures. This similarity can make it challenging to make a definitive distinction with a limited tissue sample. Since FNAC collects only a limited tissue sample, the sampled area may not represent the entire tumor. If the FNAC sample is taken from a part of the pleomorphic adenoma that contains more myoepithelial cells, it can lead to a misdiagnosis of myoepithelioma.
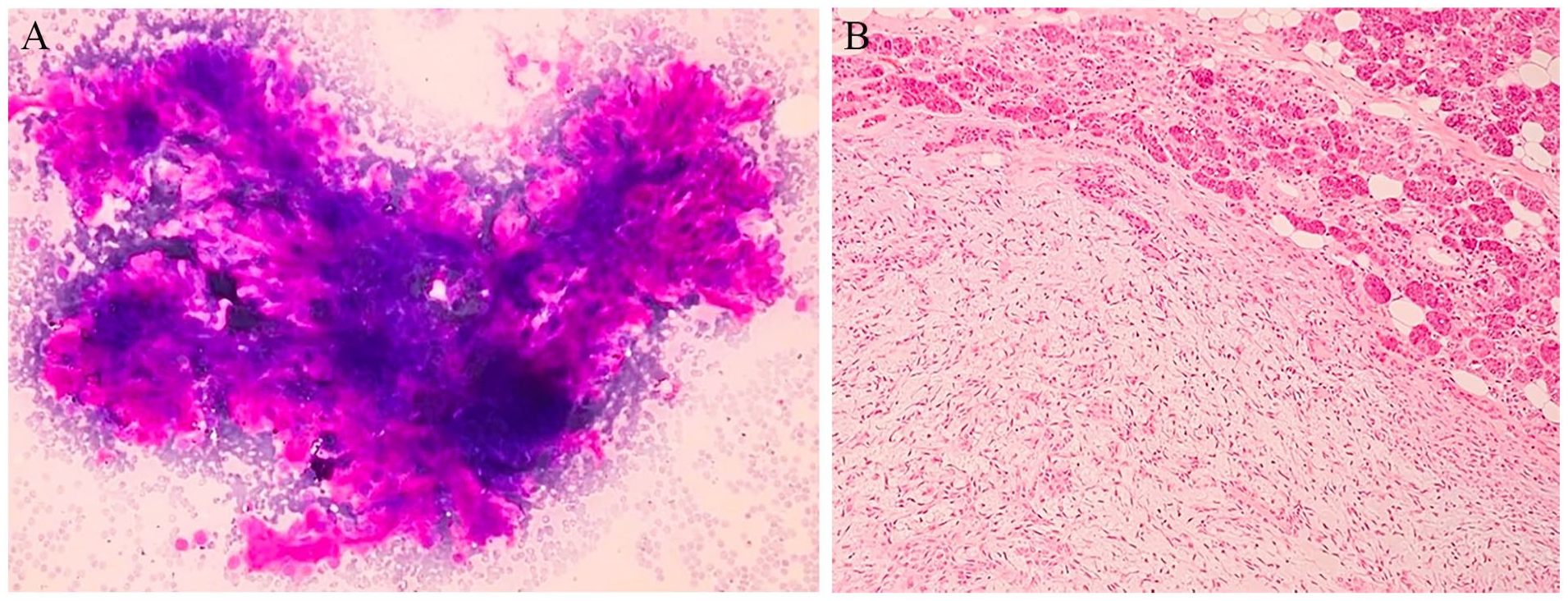
One of our false negative cases is an example where a tumor was initially thought to be a Warthin tumor with FNAC (Figure 1). Still, it was later determined to be a mucoepidermoid carcinoma upon surgical resection. These 2 types of tumors can appear similar in cellular samples. Warthin tumor consists of oncocytic epithelial cells and lymphoid stroma, while mucoepidermoid carcinoma comprises mucus-secreting cells, squamous cells, and various other cell types. It can be difficult to differentiate these cells in FNAC samples. The variability of tumors, mainly those such as mucoepidermoid carcinoma that consist of different cell types, can result in inaccurate findings if the FNAC needle samples an area of the tumor that doesn’t represent the whole. Insufficient or inaccurate sampling can also lead to these misleading results (Figures 2 and 3).
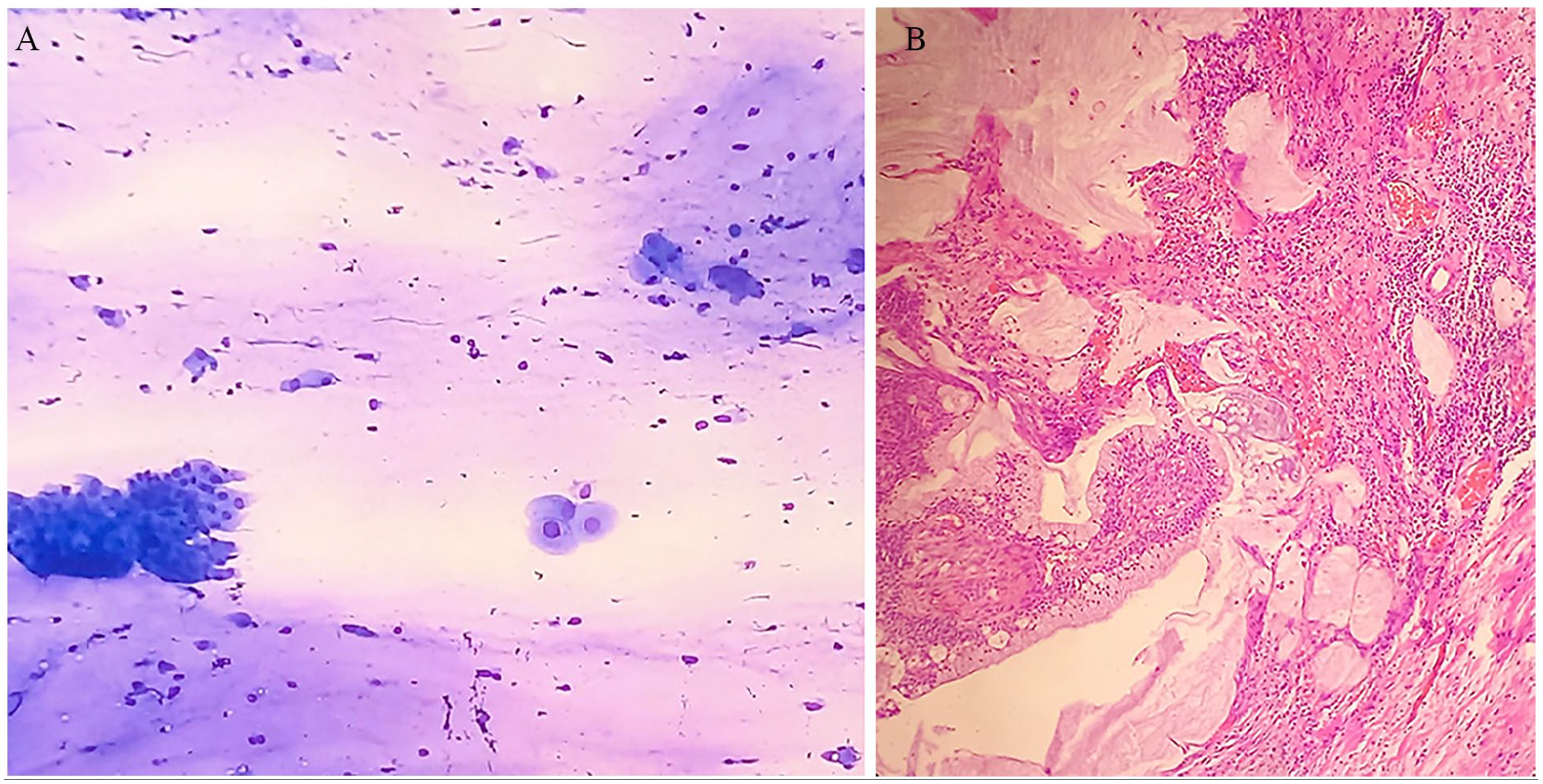
Mucoepidermoid carcinoma false negatively misinterpreted as a Warthin tumor in FNAC. (A) The smear shows clusters of oncocytoid cells, histiocytes, and numerous lymphocytes with a mucoid or proteinaceous material background. The nuclei of these epithelial cells appear relatively benign, with minimal atypia, suggesting a non-neoplastic process or a low-grade lesion and interpreted as Warthin tumor (May Grünwald Giemsa ×200). (B) In the resection material of the same case, tumoral tissue consisting of mucous and squamoid cells surrounding cystic spaces, with mucous material and numerous lymphocytes in the periphery (H&E ×200). FNAC, fine needle aspiration cytology; H&E, hematoxylin and eosin.
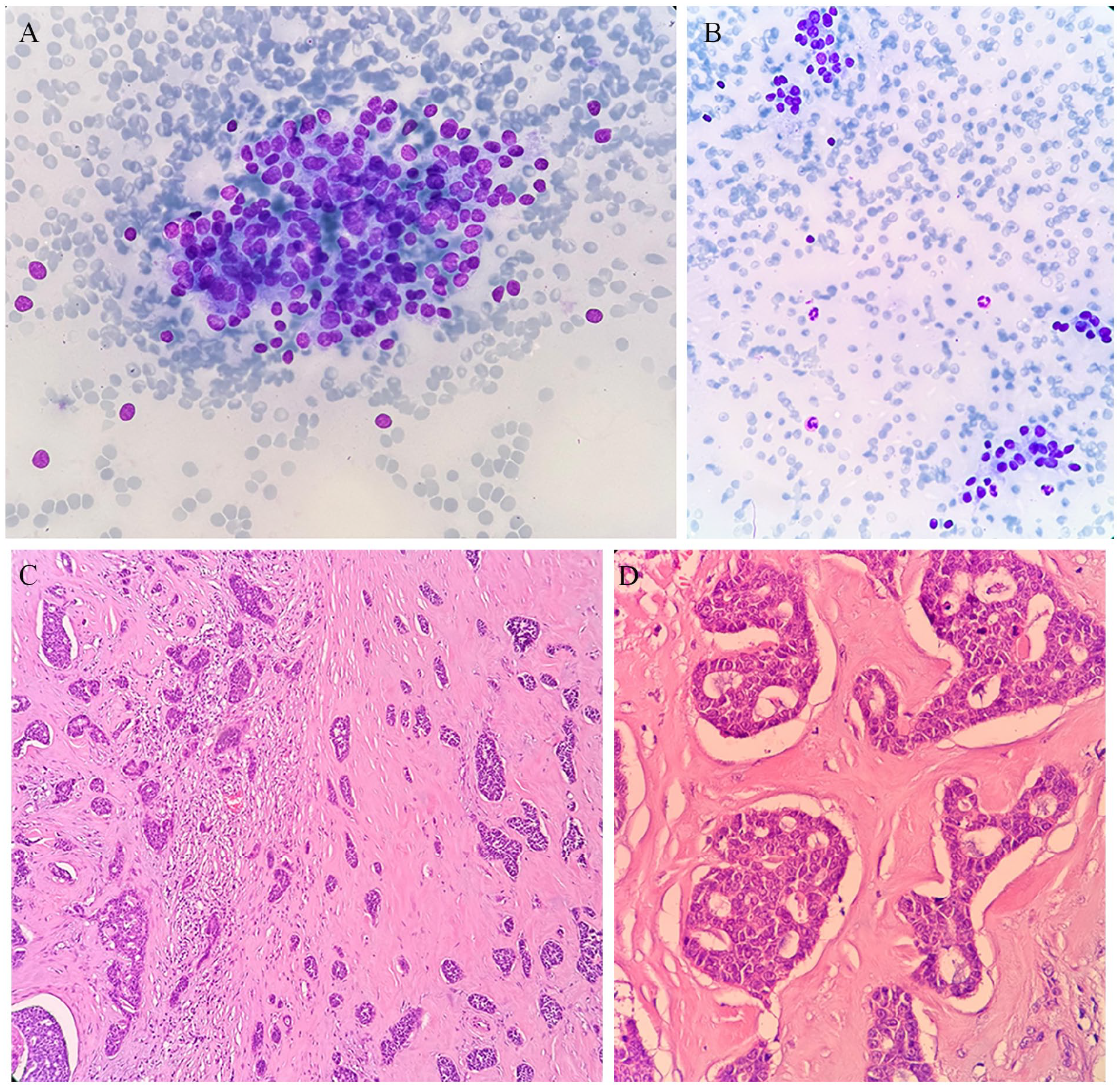
False negative result of adenoid cystic carcinoma as non-neoplastic in FNAC. (A) The smear shows benign-appearing epithelial cells among peripheral blood elements. These cells exhibit minimal atypia, suggesting a non-neoplastic or benign reactive process, consistent with benign epithelial proliferation (May Grünwald Giemsa ×40). (B) A more detailed view of benign-appearing epithelial cells, with no significant atypia noted, further supporting a benign process (May Grünwald Giemsa ×100). (C) In the histopathology material, tumor cells forming small solid groups and cribriform patterns are observed within a fibrous stroma. The tumor cells show features consistent with adenoid cystic carcinoma (H&E ×40). (D) At higher magnification, the cribriform pattern of adenoid cystic carcinoma becomes more apparent, with tumor cells surrounding spaces and forming intricate patterns (H&E ×100). FNAC, fine needle aspiration cytology; H&E, hematoxylin and eosin.
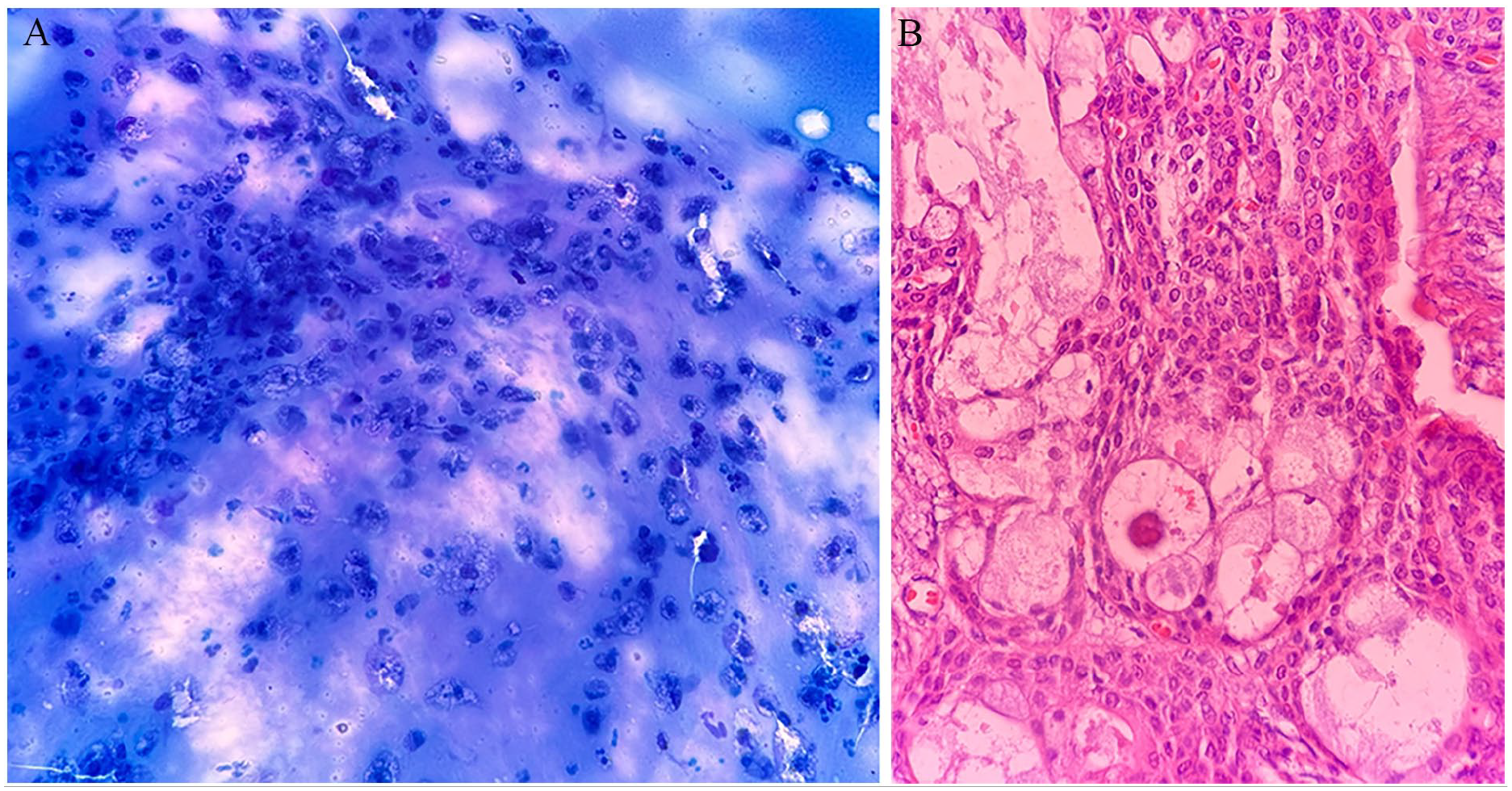
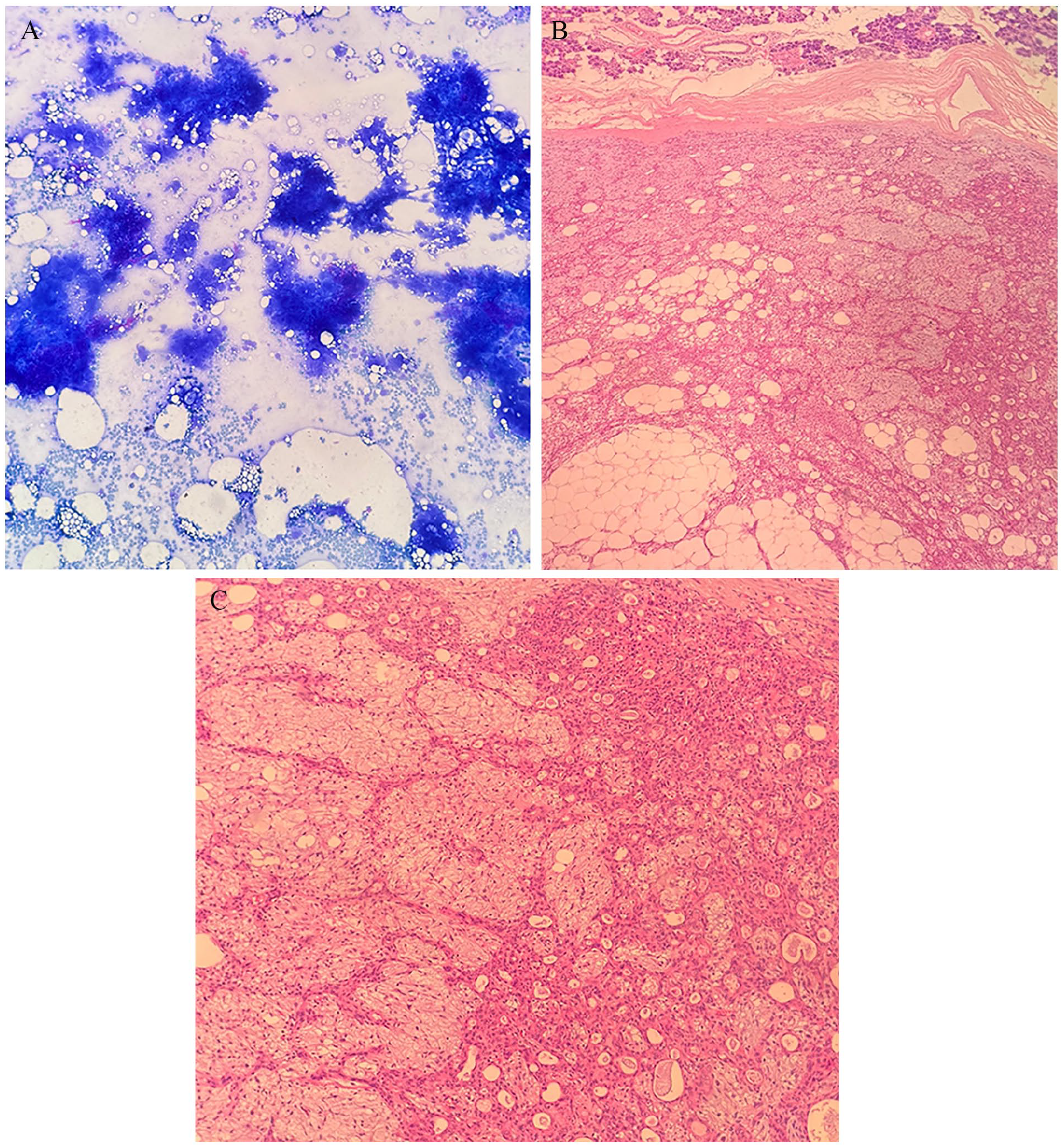
Mucoepidermoid carcinoma false negatively diagnosed as a non-specific cystic lesion in FNAC. (A) The smear shows numerous histiocytes representing a cystic lesion, with no significant atypia observed, suggesting a benign process (May Grünwald Giemsa ×200). (B) The presence of mucous and intermediate cells is observed, characteristic of mucoepidermoid carcinoma, forming glandular and solid patterns in the histopathology material (H&E ×200). FNAC, fine needle aspiration cytology; H&E, hematoxylin and eosin.
When we examine the false-positive cases, there is an initial diagnosis of low-grade adenocarcinoma (LGA) based on FNAC, but it was later found to be pleomorphic adenoma (Figure 4). LGA typically consists of a uniform cell population with a regular glandular structure, but it may display mildly invasive growth patterns and significant nuclear atypia. However, the permanent histopathology of the resected gland confirmed the diagnosis of pleomorphic adenoma with a myxoid stroma predominantly composed of myoepithelial cells. Also, there is another pleomorphic adenoma case misdiagnosed as salivary gland neoplasm of uncertain malignant potential in FNAC (Figure 5).
False-positive result of pleomorphic adenoma as low-grade adenocarcinoma in FNAC. (A) Among peripheral blood elements, large clusters of mildly atypical-looking cells (May Grünwald Giemsa ×200). (B) In the parotidectomy material of the same case, well-circumscribed tumoral tissue with a myxoid stroma, predominantly composed of myoepithelial cells, surrounded by normal salivary gland tissue diagnosed as pleomorphic adenoma (H&E ×100). FNAC, fine needle aspiration cytology; H&E, hematoxylin and eosin.
Pleomorphic adenoma false positively diagnosed as salivary gland neoplasm of uncertain malignant potential in FNAC. (A) The smear reveals large groups of epithelial cells forming papillary-like structures with unclear cellular details, indicating a dense cellular arrangement (May Grünwald Giemsa ×100). (B) Histopathology sections presented a cellularly rich pleomorphic adenoma, separated from the surrounding salivary gland tissue by a fibrous capsule (H&E ×100). (C) A closer view of the cellular component of the pleomorphic adenoma highlights its high cellularity and pleomorphic features (H&E ×200). FNAC, fine needle aspiration cytology; H&E, hematoxylin and eosin.
FS not only provides rapid diagnosis during surgery and helps decide the continuation and extent of the operation, but it also does not add any extra complications for the patient. In literature studies investigating the success of FS, sensitivity and specificity were calculated by Carvalho et al 24 at 61.5% and 98%, respectively, while Seethala et al 16 reported 77% and 100%. Similarly, Zbären et al 13 found a sensitivity of 93% and a specificity of 95%, which is close to our study results. Given that nearly half of the patients we examined with FS were malignant, we believe that we have achieved results similar to those in the Zbären et al study, where 62% of the cohort had malignant tumors. Records of some patients from our study that may exemplify the potential contributions of FS to FNAC analysis are presented in Table 6.
Comparison of FNAC, FS, and Histopathology Results Across Different MSRSGC Categories.
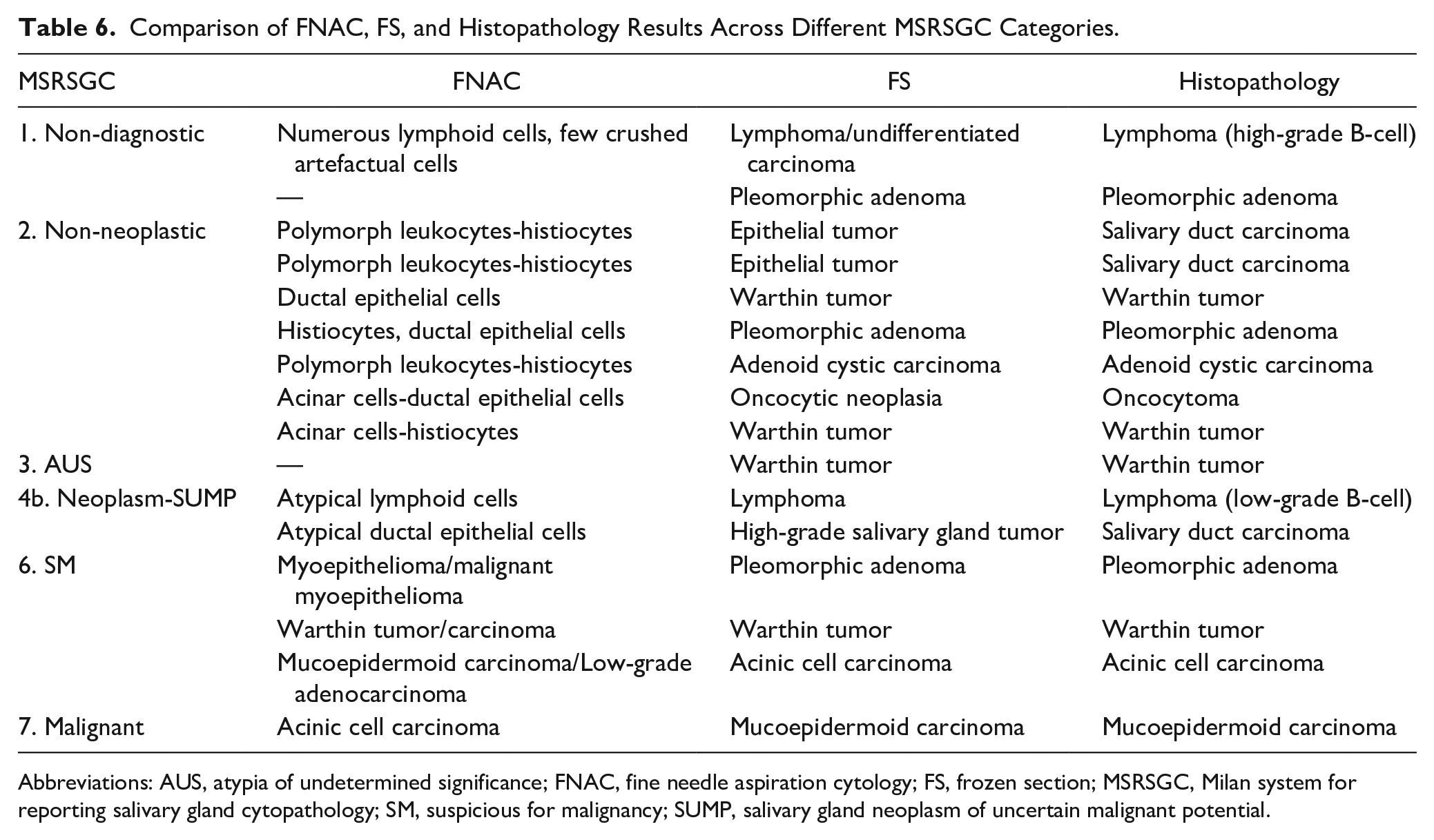
Abbreviations: AUS, atypia of undetermined significance; FNAC, fine needle aspiration cytology; FS, frozen section; MSRSGC, Milan system for reporting salivary gland cytopathology; SM, suspicious for malignancy; SUMP, salivary gland neoplasm of uncertain malignant potential.
The results of our study have important clinical implications. It is essential to fully understand the diagnostic accuracy of both FNAC and FS when choosing between them, particularly in cases where accurately distinguishing between benign and malignant tumors can impact surgical plans and patient outcomes. Our data indicates that FNAC can be a preferred initial diagnostic tool, but its limitations require careful interpretation, particularly in ambiguous cases where FS may offer more definitive guidance. In our department, FNAC is used as the initial diagnostic procedure. When FNAC results indicate neoplasia with uncertain malignant potential or are suspicious of malignancy, we request an intraoperative FS to eliminate the risk of false positives during surgery. Similarly, for cases where FNAC reports are non-neoplastic or show atypia of uncertain significance, we plan an intraoperative FS to prevent false negatives and potentially proceed with neck dissection. Furthermore, as observed in our studies, when FNAC presents a lesion as benign neoplasia, but the permanent histopathology results are malignant, we routinely request FS for patients whose clinical features or radiological imaging raise suspicions.
In the future, advancements in diagnostic technologies can potentially improve accuracy and reliability. Further research on advanced imaging techniques or molecular diagnostics could provide valuable insights and transform the diagnostic landscape for parotid gland tumors.
Conclusion
FNAC is highly successful in accurately detecting non-malignant lesions, but it requires support due to its suboptimal sensitivity and positive predictive values. Our study highlights the complementary role of FS to the FNAC in diagnosing parotid gland tumors. While FNAC provides a practical and patient-friendly initial assessment, it has its limitations, particularly in challenging cases where higher accuracy of FS can be decisive. FS can be requested in parotid tumors when FNAC yields non-diagnostic or non-neoplastic results to detect the presence of neoplasia, in cases of atypia of undetermined significance or benign neoplasms to confirm and characterize the lesion, and in suspected or confirmed malignancies where tumor differentiation may influence the extent of surgery. Therefore, our findings suggest a balanced use of these diagnostic tools, guided by clinical judgment, patient factors, and resource availability, to optimize patient outcomes in managing parotid gland tumors.
Footnotes
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
The Ethics Committee of the Bursa Uludag University Hospital waived the need for ethics approval and patient consent for the collection, analysis, and publication of the retrospectively obtained and anonymized data for this noninterventional study.