
Abstract
Rosai-Dorfman disease (RDD), also known as sinus histiocytosis with massive lymphadenopathy, is an uncommon histiocytic disease with idiopathic etiology and unique pathology. Extra-nodal RDD that occurs in the nasal cavity is extremely unusual and the characteristic clinical features are unknown. Herein, we report a case of nasal septum RDD, with intermittent epistaxis from the left nasal cavity, which led to collapse of the nasal bridge. The patient underwent surgical biopsy, and a diagnosis of nasal septum RDD was established. No further treatment was performed. An enlarged mass was found in the second postoperative year which was treated by surgical excision in the third postoperative year. To improve the current diagnostic and therapeutic approach of extra-nodal RDD, we incorporate previous reports from the literature to discuss the pathological characteristics, pathogenesis, clinical manifestations, diagnosis, and therapy for this rare disease.
Introduction
Rosai-Dorfman disease (RDD), also known as sinus histiocytosis with massive lymphadenopathy, is an agnogenic rare benign histiocytic proliferative disease. 1 According to the extent of involvement, RDD can be classified as lymph node, extra-nodal, or mixed (ie, for the latter, simultaneous involvement of lymph nodes and extra-nodal organs). Patients with RDD often present with painless bilateral enlarged cervical lymph nodes, which are often fused. In 43% of cases, other external tissues are involved, 2 such as bone, skin, central nervous system, and head and neck. However, RDD in the nasal septum has rarely been documented.
Herein, we report a case of nasal septum RDD characterized by nasal dorsum collapse. The clinical manifestations, pathological features, diagnosis, and treatment of this patient population are summarized from the literature. A detailed search of the PubMed and CNKI (China Academic Journals) databases was performed for articles published between 1990 and 2021. The search terms included “nasal cavity,” or “paranasal sinus,” or “nasal septal,” and “Rosai–Dorfman disease,” or “sinus histiocytosis with massive lymphadenopathy.”
Case report
A 55-year-old woman presented to our hospital with nasal dorsum collapse while wearing her glasses. She had experienced occasional epistaxis, but no hyposmia, nasal obstruction, diplopia, headache, fever, or other discomforts. She had a past medical history of 6 years that was significant for glaucoma and uveitis. She had smoked tobacco, but had quit 4 years previously.
Nasal endoscopy showed an anterior septal deviation to the left and a mass with a friable surface on the left side of the nasal septum (Figure 1A). No enlarged lymph nodes were detected upon either physical examination or ultrasonography. Her white blood count was 11.49 × 109/L. Her erythrocyte sedimentation rate (ESR) was not measured. Computed tomography (CT) and magnetic resonance imaging (MRI) of the nasal sinuses (Figures 1B-1D) showed a solid enhanced mass (∼1.4 × 1.1 × 1.9 cm) on the left side of the septum, with suspected nasal bone erosion. Imaging findings on the first admission. (A) Nasal endoscopic findings. NS: nasal septum, LA: the medial side of the left alar. (B) Coronal CT showed a soft tissue lesion. (C) Sagittal CT showed nasal dorsum collapse (red arrow). (D) Axial MRI showed that the lesion was located on the left side of the nasal septum. (E) Hematoxylin-eosin staining revealed fibrous tissue hyperplasia with infiltration of plasma cells and lymphocytes and a diffuse infiltrate of histiocytes (200×). The histiocytes presented with large vesiculated nuclei, and emperipolesis was observed (yellow arrow). (F) S-100 protein was strongly positive in the nucleus and cytoplasm of tissue cells (200×). (G) CD68 was positive in the cytoplasm of tissue cells (200×). (H) CD1a was negative in tissue cells (200×).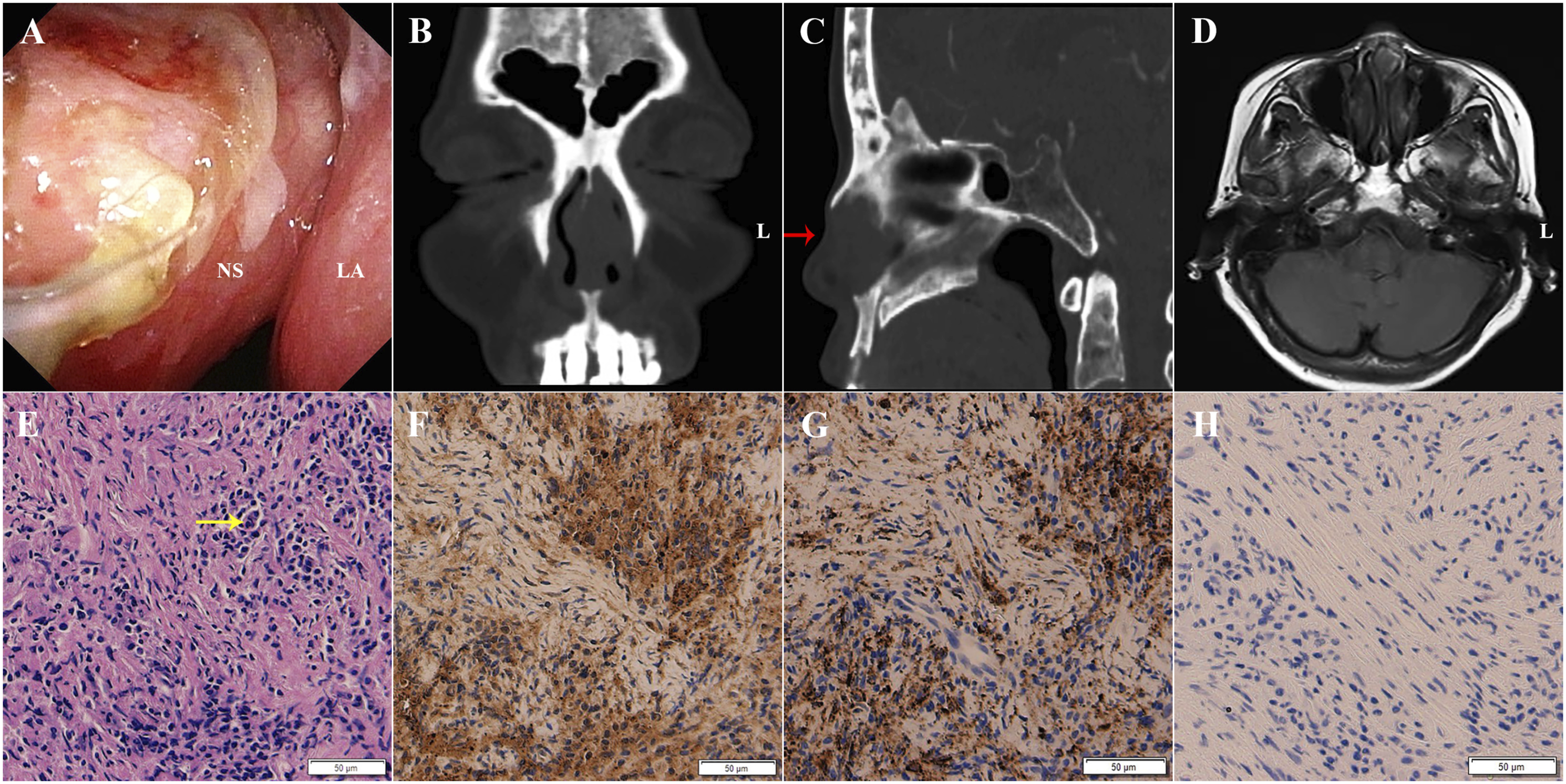
A transnasal endoscopic surgical biopsy was performed under general anesthesia, and most of the diseased tissue was excised for pathological examination. The histopathological analysis showed fibrous tissue hyperplasia with significant infiltration of plasma cells, lymphocytes, and histiocytes, with large and vesiculated nuclei (Figure 1E). Immunohistochemistry for S100 (Figure 1F) and CD68 (Figure 1G) were positive, but CD1a protein was negative (Figure 1H). The final diagnosis was RDD of the nasal septum. The patient was discharged 1 week after surgery. No further treatment was performed, for the patient’s personal reasons.
In the second postoperative year, the patient began to experience bilateral nasal obstruction and hyposmia. Laboratory results indicated leukocytosis and a normal ESR. The CT and contrast-enhanced MRI showed a large mass (3.8 × 2.5 cm) which involved the nasal septum and the left ethmoid sinus, with significant bone erosion (Figures 2A-2D). Imaging findings before the second surgery resection. 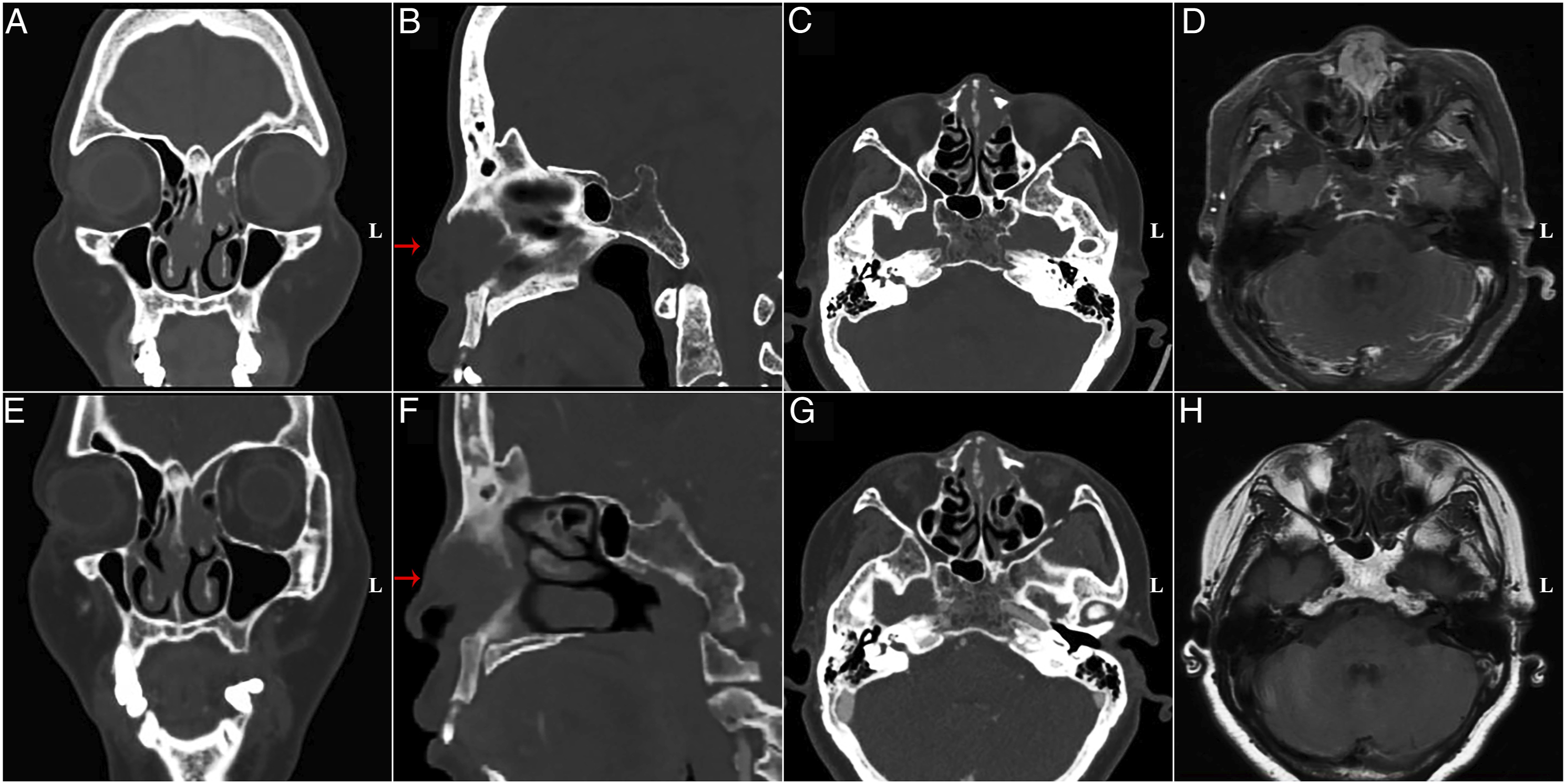
The patient was advised to undergo surgical resection of the tumor, but due to greater exigencies in hospitals during the COVID-19 epidemic, this was forestalled. For 1 year, the patient self-medicated with traditional Chinese medicine (including Poria cocos, Panax ginseng, Ligusticum chuanxiong Hort, Laminaria, and Salvia miltiorrhiza Bunge). A repeat CT performed in the third postoperative year showed that the mass was significantly reduced, to ∼1.7 × 1.6 cm (Figures 2E-2H). Subsequently, the patient underwent transnasal endoscopic surgery at another hospital for the complete removal of the tumor. Postoperative pathological results were consistent with RDD. There has been no recurrence after a follow-up of more than 10 months.
Discussion
Rosai-Dorfman disease is a histiocytic proliferative disorder that primarily affects cervical lymph nodes. Adults younger than 20 years, especially males, are reportedly more susceptible. A study that included 423 cases of RDD reported extra-nodal involvement in 43%, commonly the skin, eyes, bone, parotid gland, and respiratory, gastrointestinal, and central nervous systems. 2 The most common extra-nodal lesions were in the head and neck.
The classic presentation of RDD consists of bilateral, massive, and painless cervical lymphadenopathy with or without intermittent fevers, night sweats, and weight loss. 3 The nasal cavity and sinuses are usual sites of extra-nodal invasion, commonly leading to symptoms such as nasal obstruction and epistaxis. The nasal septum is rarely invaded. Laboratory results are usually characterized by leukocytosis and an accelerated ESR. During clinical practice, nasal RDD is often misdiagnosed due to the paucity of pathognomonic clinical features.
The diagnosis for our patient was complicated by the lack of typical RDD features at presentation. Her body temperature and ESR were normal, and there was no other organ involvement; although laboratory findings also showed leukocytosis. The patient had a collapsed nasal bridge and minimal damage to the bone structure, which could not be explained. We could not initially rule out that a viral or bacterial infection might have caused the saddle nose deformity.
Notwithstanding that the clinical characteristics of RDD have been widely explored, little is known of its etiology or pathogenesis. RDD is a heterogeneous entity that can occur as an isolated disorder, or may be associated with immune, hereditary, or neoplasia disease. 4 In the past, RDD was thought to result from immune dysfunction and viral infections. There is increasing evidence that RDD coexists or is associated with autoimmune hemolytic anemia,5,6 RAS-associated autoimmune leukoproliferative disease, 7 and autoimmune atrophic gastritis. 8 Interestingly, the presence of several viruses has been documented during respective pathological examinations of RDD tissues: human immunodeficiency virus (HIV), 9 human herpesvirus 6, 10 Epstein-Barr, 11 parvovirus B19 (B19), 12 and cytomegalovirus. 13 Nonetheless, the causal link between viral infections and RDD has not been proven.
In addition, germline mutations in SLC29A3 (solute carrier family 29 member 3) have been reported in patients with familial RDD.14,15 In contrast, recent molecular studies have identified specific mutations in the MAPK/ERK signaling pathway, including KRAS,16-18 MAP2K1,18,19 NRAS, 20 and BRAF.21-23 The above findings suggest that genome instability may be a factor causing RDD. Garces et al 18 documented that in RDD, mutations were more commonly associated with head and neck lesions. In our case, it is regrettable that the lesion was too small during the second surgery to perform next-generation sequencing.
Extra-nodal RDD, originating from the nasal cavity, exhibits non-specific imaging findings, with only mucosal thickening or a soft-tissue mass filling the nasal cavity and sinus. However, osteosclerosis and bone erosion have been documented in some cases.24,25 Importantly, the enhancement pattern of the RDD mass can be similar to tumor lesions, leading to misdiagnosis. In our present case, the first preoperative imaging raised the suspicion of localized nasal bone involvement. Before performing the second surgery, a repeat CT showed that the lesion had invaded the nasal bone and the underlying subcutaneous tissue.
Unlike malignancies, RDD is a benign disorder that runs an indolent and self-limiting course. Typical histopathological and immunohistochemical patterns are diagnostic of RDD. Studies have shown that in patients with RDD, the lymphatic sinus is invaded by plasma cells and histiocytes, which leads to partial or complete destruction of the structure of the lymphatic sinus. 26 The histopathology of RDD often displays emperipolesis, that is, phagocytized lymphocytes and plasma cells in the cytoplasm of the histiocytes. 27 However, emperipolesis is not a requirement for the diagnosis, since extra-nodal RDD can be inconspicuous 4 ; extra-nodal lesions are usually associated with more fibrosis, fewer RDD histiocytes, and less emperipolesis.
Unlike other reported cases of nasal RDD, in our current case typical emperipolesis was observed (Figure 1E). In addition, the immunohistochemistry showed strong positive staining for S-100 proteins and CD68, variable CD163 and CD14 positivity in histiocytes, and absence of staining for CD1a and CD207. 4 The heterogeneous clinical manifestations of RDD, and its variable pathological features, may significantly challenge differentiating extra-nodal disease from histiocytic proliferative diseases, lymphoma, tuberculosis, sarcoidosis, and reactive sinus hyperplasia. 26 In our case, given that in the diseased tissue samples there was positive staining for both CD68 and S-100 in histiocytes and CD1a was negative, RDD could be differentiated from Erdheim-Chester disease and Langerhans cell histiocytosis. 28 Accordingly, a diagnosis of intranasal RDD was determined.
The consensus published in 2018 is that there is no gold-standard optimal treatment for RDD, but treatment should be tailored to the individual’s clinical profile. 4 First- and second-line treatments are not applicable. Importantly, most patients without complicated lymphadenopathy or organ dysfunction do not require treatment. Surgical resection is usually recommended to rapidly relieve symptoms for patients with extra-nodal or vital organ invasion, or who present with significant local symptoms. 29 Hormones, antibiotics, immunomodulatory therapy, and local low-dose radiotherapy or chemotherapy can also be used to treat RDD. 4 Based on the 2018 consensus recommendations for the diagnosis and management of RDD, targeted next-generation sequencing for MAPK mutations should be considered in severe or refractory cases, and targeted therapy is indicated if driver mutations are identified. 4
A phase 2 trial for the use of cobimetinib in patients with wild-type histiocytosis, including RDD, is ongoing (NCT02649972) and the early results are promising. 30 However, the broad applicability of tumor sequencing and targeted treatments has not been established. Combining several methods has become the mainstream strategy to cure the disease; however, the effectiveness remains uncertain. The overall survival of patients with RDD remains inconclusive, although most scholars believe that the disease is benign and self-limited. Large lesions that invade multiple organs have been associated with poor postoperative outcomes. 31 For sinonasal sites, follow-up periods have ranged from 1 month to 18 years, with a mean of 35 months. 32 In addition, some RDD cases exhibit invasive biological phenotypes, and these lesions are prone to recur. In such cases, treatment with radiotherapy, 33 or chemotherapy and oral hormone therapy 34 can be considered.
In this study, in the second postoperative year an enlarged nasal mass was found with no other organ involvement. During the following year, the patient took traditional Chinese medicine (as far as known, Poria cocos, Panax ginseng, Ligusticum chuanxiong Hort, Laminaria, and Salvia miltiorrhiza Bunge). The size of the mass significantly declined. Traditional Chinese medicine has been demonstrated to exert immunomodulatory effects.35,36 It may be that the patient benefited from these medicines, and they may be important for treating RDD.
The patient subsequently underwent transnasal endoscopic surgery to remove the tumor completely, with no recurrence as of this writing. Although many RDD treatment approaches have been documented, none of them were effective in all cases. Interestingly, tumor sequencing and targeted therapies, such as MEK inhibitors, have been increasingly used in recent years and could have potential clinical value in RDD diagnosis and management. Further studies are warranted. In addition, given that it is widely acknowledged that the clinical course of most cases of RDD is indolent, the follow-up period should be sufficiently long to assess the outcomes of RDD more accurately.
Conclusion
Rosai-Dorfman disease is a rare, self-limited histiocytic proliferative disorder of unknown etiology. Comprehensive RDD evaluation involves a careful medical history, physical examination, imaging studies, and laboratory evaluations to determine the extent of the disease and comorbidities. Unexplained nasal dorsum collapse should be considered an extra-nodal sign of RDD, although it is rare. Characteristic lesional histiocytes are positive for S100 and CD68, and negative for CD1a. There is no consensus concerning the optimal management of RDD. For nasal RDD, endoscopic sinus surgery may be a good option for short-term symptomatic control and restoration of function.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The Ethics Committee of Yantai Yuhuangding Hospital (Yantai, China) approved this study (approval number 2022-007).
Informed consent
The patient granted permission through written informed consent for the publication of their anonymized information.