
Abstract
Rosai–Dorfman disease (RDD) is a rare non-malignant disorder, characterized by painless multiple cervical lymphadenopathy, fever, and elevated inflammatory markers. Its diagnosis is difficult due to its rare incidence and various clinical presentations, especially in extranodal involvement. In this report, we demonstrate a patient with RDD who presented with a nasal septum and laryngeal tumor that caused dyspnea. We achieved a successful treatment outcome with combined surgical resection of the laryngeal mass and corticosteroid medication. The symptoms and tumors were resolved within 3 weeks after treatment. We reported our experiences with review of literatures.
Introduction
Rosai–Dorfman disease (RDD) is a non-malignant tumorous histiocytosis involving lymph nodes or extranodal organs. 1 It usually involves cervical and other lymph nodes, but 30–40% of cases demonstrated extranodal organs such as the skin, upper respiratory tract, sinuses, thyroid gland, and brain.2,3
Because of the rarity of RDD, the clinical spectrum and treatment outcomes are not defined well. The disease can cause various clinical symptoms including palpable mass and pain, as well as involve various organ including skin, lymph node, lung, and liver. 4 Extranodal involvement by RDD was thought to be uncommon in the past, but some reports suggest that it is present in up to 40% of cases.5,6
Imaging features of RDD are not well established due to its rarity and heterogeneous involved structures. 7 Thus, biopsy should be performed to obtain adequate diagnosis by morphological and immunohistochemical evaluation.1,8,9 However, in extranodal RDD locations such as the larynx and trachea, it can be difficult to collect a tissue sample, which could delay diagnosis.
Asymptomatic RDD patients do not need treatment, 10 while steroids are a first-line treatment for symptomatic RDD despite unpredictable effectivity and durability.11,12 In the presence of life-threatening manifestations by vital organ compression and airway obstruction, surgery and radiation are treatment options.13,14
In this case report, the authors describe a patient with RDD who had delayed diagnosis because of extranodal involvement with unusual clinical presentation including airway obstruction. In addition, we report the combined medical and surgical treatment to achieve a successful outcome.
Case Report
A 68-year-old male visited another hospital for aggravating stridor and dyspnea, and endoscopic examination revealed a nasal septum and subglottic mass. Upon suspicion of malignancy, a biopsy was performed from both nasal cavity and subglottis under general anesthesia, and tracheostomy was performed due to the aggravated dyspnea. The patient was transferred to our hospital due to unclear pathologic diagnosis.
A well-marginated left subglottic mass obstructing the laryngeal airway and septal mass pushing against sinus and turbinate structures of both nasal cavities were shown in our endoscopic exam (Figure 1A-C). Neck enhanced computed tomography (CT) demonstrated a 3.5 cm nasal septum mass destructing adjacent sinus structures and a 3.3 cm enhancing mass at the left subglottis (Figure 2A and D). Endoscopic images of a case with Rosai–Dorfman disease. Preoperative endoscopic findings of larynx (A), right nasal cavity (B), and left nasal cavity (C). Postoperative endoscopic findings of larynx (D), right nasal cavity (E), and left nasal cavity (F). Enhanced CT imaging of larynx (A) and nasal cavity (D) shows a space-occupying lesion with equivocal enhancement. H & E staining of the larynx (B) and nasal cavity (E) masses showed histiocytes and positive S100 staining in both the larynx (C) and nasal cavity (F).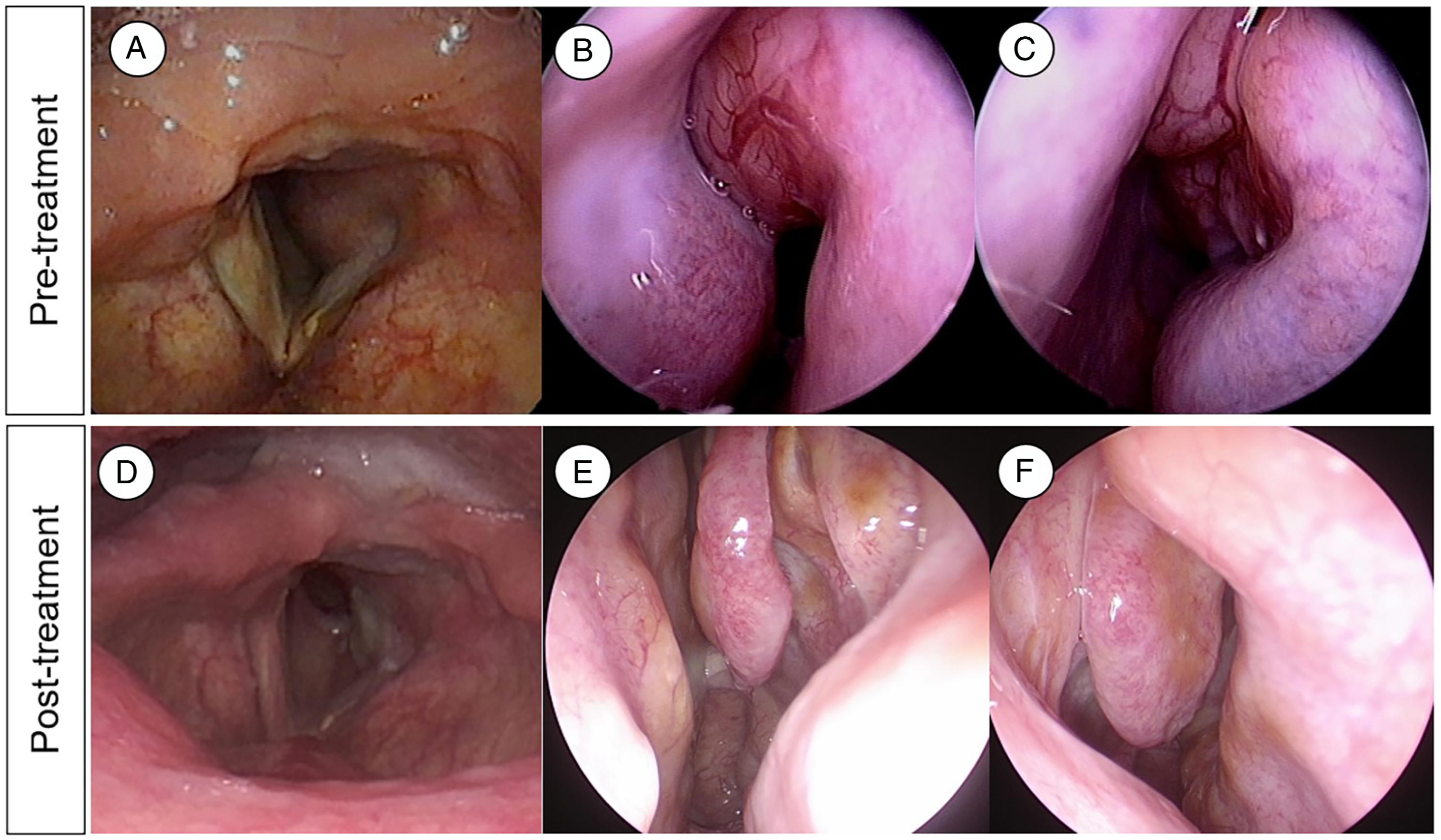
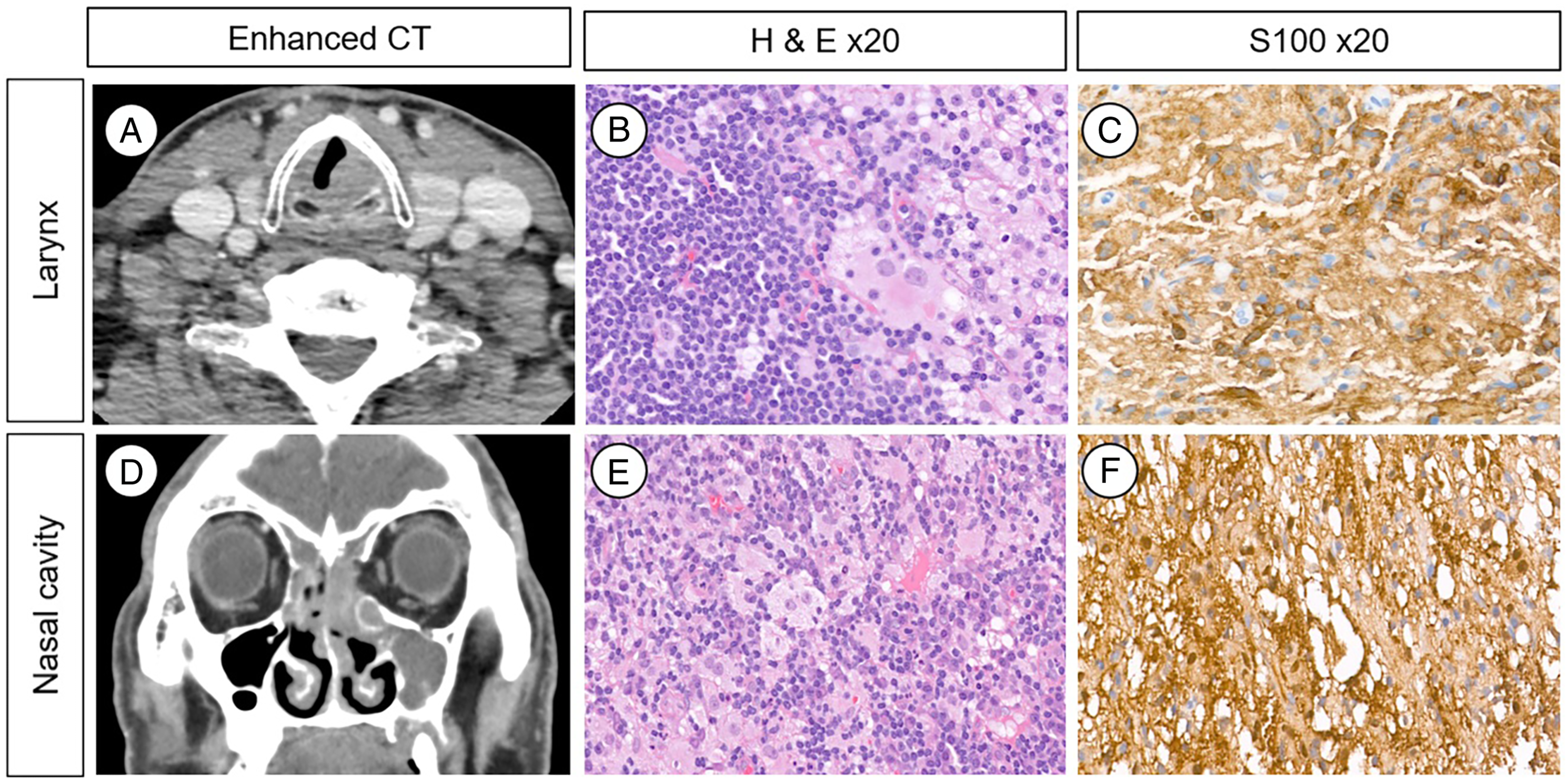
We performed re-biopsy of the nasal septal and subglottic mass under local anesthesia; pathology of the nasal septum and subglottic tumor was diffuse histiocytic, lymphocytic, and plasmocytic infiltration with positivity for S100 stain (Figure 2C and F). The final pathologic diagnosis was extranodal Rosai–Dorfman disease of the nasal cavity and subglottis.
After pathologic diagnosis, the patient received intravenous steroid therapy (dexamethasone 5 mg, three times a day) for 1 week, after which both masses had decreased in size.
However, the subglottic mass was not small enough for decannulation, so laser excision with laryngeal microscopic surgery was performed under general anesthesia. The patient was decannulated without respiratory symptom and discharged. He received 2 weeks of additional intraoral steroid medication (methylprednisolone 8 mg).
In an outpatient clinic at 1 month and 3 months after discharge, the patient had no respiratory symptom, and the nasal cavity mass was non-visible. The subglottic mass was decreased markedly, and the patient underwent pinpoint tracheostoma at the last visit (Figure 1D and F).
Discussion
Rosai–Dorfman disease is a non-Langerhans cell histiocytosis characterized by positive CD68 and S100 histiocytes.1,15 It is difficult to achieve early diagnosis of RDD because of its rarity, heterogeneous symptoms, and involved organs. Rosai–Dorfman disease has various clinical presentations including subcutaneous masses, fever, leukocytosis, and nonpainful cervical lymphadenopathy. 4 A previous study reported that duration from symptom onset to diagnosis of RDD ranged from 0 to 128 months. 4 In our case report, we experienced delayed diagnosis despite performing 2 biopsies under general anesthesia.
The histopathological diagnosis of RDD can be challenging due to non-specific histologic findings, especially in extranodal RDD. Rosai–Dorfman disease cells usually exhibit emperipolesis, the nondestructive phagocytosis of lymphocytes or erythrocytes. However, these pathognomonic findings can be obscured by inflammatory cells or fibrosis, especially in extranodal RDD. 4 Prominent inflammatory background with plasma cells or lymphoid follicle formation and neutrophilic infiltrates in the extranodal RDD can be mistaken as non-specific chronic inflammation. 16 In addition, RDD is characterized by positive CD163 and S100 staining but negative CD1a in immunohistochemistry. 17 In our case report, we observed positive S100 staining in the larynx and nasal cavity RDD lesions.
There is no consensus about RDD treatment, and about 20–50% of cases show spontaneous resolution without treatment.18,19 In symptomatic RDD, the treatment of choice has been corticosteroid, the response rate of which was reported to be 56%.4,10 Surgery has been an appropriate option in cases of resectable and localized disease. 14 In addition, surgery could be used in patients with airway obstruction to secure airway patency, as in our case. We observed fair response to corticosteroid treatment for the nasal cavity lesion, but the laryngeal lesion was not reduced enough to remove the tracheostoma. Therefore, we performed combined surgical and medical treatment, which resulted in successful reduction of the remaining tumor and improvement of symptoms.
In this case, we experienced a rare clinical presentation, by which dyspnea was caused by multiple airway involvement of RDD of the larynx and nasal cavity, and we achieved a successful treatment outcome using a combined medical and surgical approach.
Footnotes
Author Contributions
First two authors were equally contributed to this work. Conceptualization: C.L., N.C., Y.L., J.H.P., and Y.I.S. Data curation: C.L., N.C., Y.L., J.H.P., and Y.I.S. Formal analysis: C.L., Y.L., and N.C. Methodology: C.L., N.C., Y.L., J.H.P., and Y.I.S. Project administration: C.L., N.C., and Y.I.S. Visualization: C.L., N.C., and Y.L., Writing—original draft: C.L., N.C. Writing—review and editing: N.C., Y.I.S.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.