
Abstract
Rosai–Dorfman disease (RDD) is characterized by sinus histiocytosis with massive lymphadenopathy, and the tissue exhibits positive results for S100 and CD68. This lesion typically affects the lymph nodes and rarely involves the nasal soft tissues. This report aims to present a case of RDD involving the nasal soft tissues, presenting with nasal congestion and rhinorrhea as the primary complaints. The patient underwent surgery navigated by nasal endoscope did not report recurrence after operation.
Keywords
Introduction
Rosai–Dorfman disease (RDD) is a rare benign type II histiocytosis, also known as sinus histiocytosis with massive lymphadenopathy. Its characteristic feature is that the histiocytes in the tissue are positive for both S100 and CD68.1 -3 According to the extent of lesion involvement, RDD can be classified into 3 subtypes: nodal, extranodal, and mixed, in which extranodal type accounts for only 5%. 4 Nodal subtype presents as painless bilateral cervical lymphadenopathy and may involve axillary and inguinal lymph nodes, as well as mediastinal lymph nodes. Extranodal subtype can be observed in the respiratory tract, skin, bone, orbit, genitourinary tract, central nervous system, bone marrow, visceral organs, and soft tissue. However, only a few cases of extranodal RDD occur in soft tissue.1,5 Although nodular RDD and soft tissue RDD share similarities, the features in soft tissue lesion are usually not distinct, making the identification and diagnosis of these lesions complicated.
Case Report
A 52-year-old female patient presented to our hospital with left-sided nasal congestion, rhinorrhea, occasional bloody nasal discharge, slight loss of smell, and occasional headaches. These symptoms had appeared 2 months prior without a discernible cause. The patient was previously diagnosed with allergic asthma due to coughing. She had improved after taking montelukast sodium tablets and inhaling budesonide formoterol powder. Nasal endoscopy examination (Figure 1A) revealed a well-defined, soft, smooth swelling measuring approximately 2 × 2 × 1.5 cm in the anterior upper portion of the left nasal septum. The base of the swelling was located on the left anterior part of the nasal septum, with no redness, discharge, or tenderness observed. Computed tomography (Figure 1B) indicated that the lesion partially protruded into the left anterior vestibule and was adjacent to the nasal septum and the left inferior nasal turbinate, while compressing nearby bone without any apparent absorption or destruction. Other tests did not reveal any significant abnormalities.
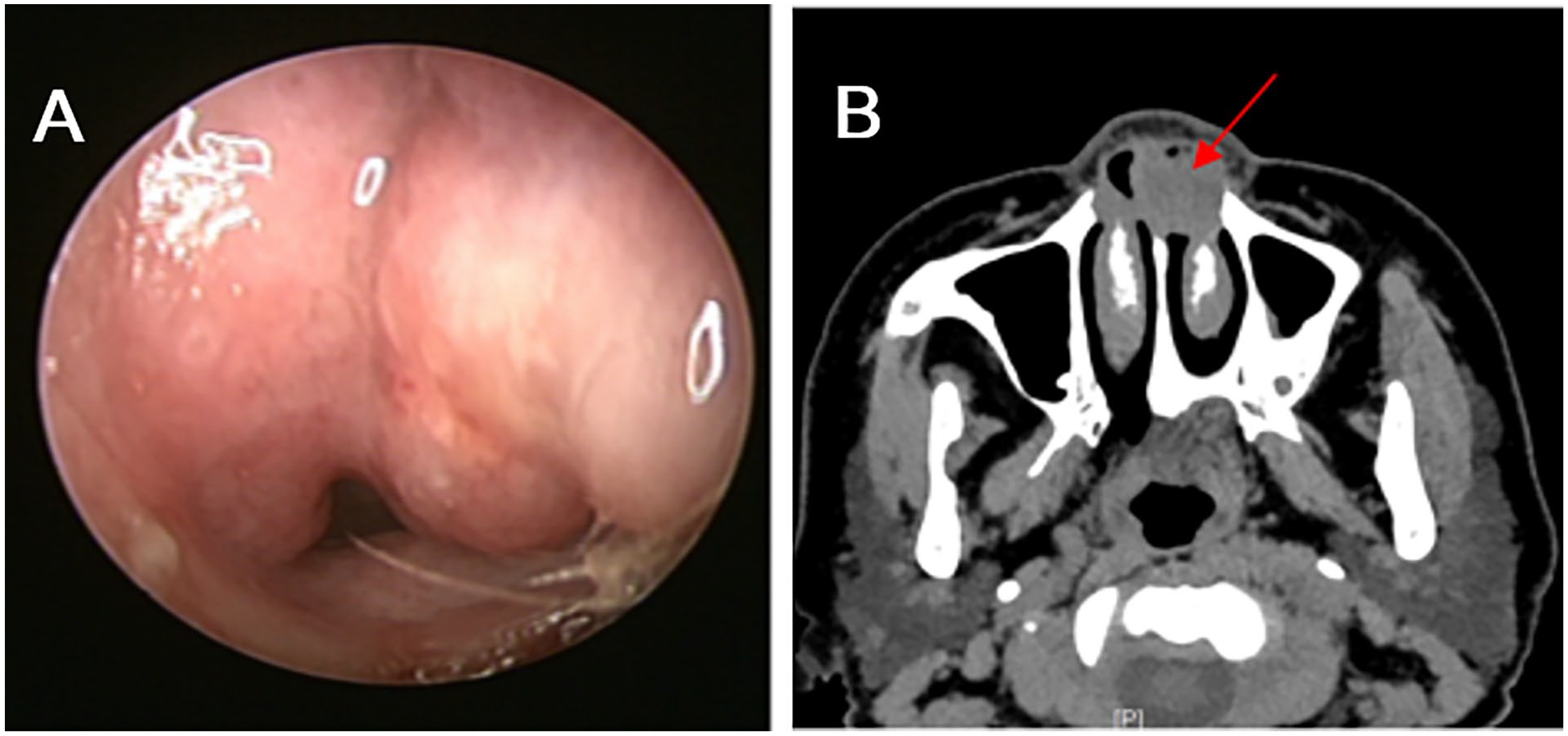
(A) Nasal endoscopy examination: A soft, smooth, well-defined swelling was observed in the anterior upper part of the left nasal septum and (B) enhanced computed tomography: A nodule was observed in the lower left nasal cavity, which partially protrudes into the left anterior vestibule.
The patient underwent surgery after excluding surgical contraindications. The tumor at the base of the left nasal cavity was separated and removed using a small round knife under nasal endoscope. During the surgery, it was observed that the base of the tumor was located at the anterior and upper part of the left nasal septum, deeply reaching the nasal septal cartilage. After completely separating and exposing the border of peripheral tissues, tumor was removed in a whole block. Following thorough hemostasis, artificial repair of the biological film was used to repair the exposed cartilage with a size of about 2.5 × 2.5 cm, and absorbable hemostatic cotton was used to pack the wound. Intraoperative frozen pathology (Figure 2A and B) indicated the infiltration of lymphocytes in the cytoplasm of tissues; postoperative immunohistochemistry (Figure 2C and D) confirmed the diagnosis of soft tissue RDD with positive expression of CD68 and S100. After the operation, the patient received symptomatic treatment such as anti-infection, hemostasis, and nasal cavity irrigation. On the sixth day-post surgery, the surgical area recovered well, and the patient was discharged with the advice to continue taking chlorpheniramine maleate tablets, nasal inflammation tablets, and luohuazizhu tablets, as well as nasal cavity irrigation. The patient was followed up in the outpatient clinic, and at the 3-month postoperative visit, no tumor recurrence was observed during nasal endoscopy, and the healing of the nasal septal mucosa was satisfactory. It was originally planned to have re-examination imaging half a year after the operation, but due to external factors such as the patient residing in another province and the ongoing epidemic situation, the patient has not yet completed the re-examination imaging.
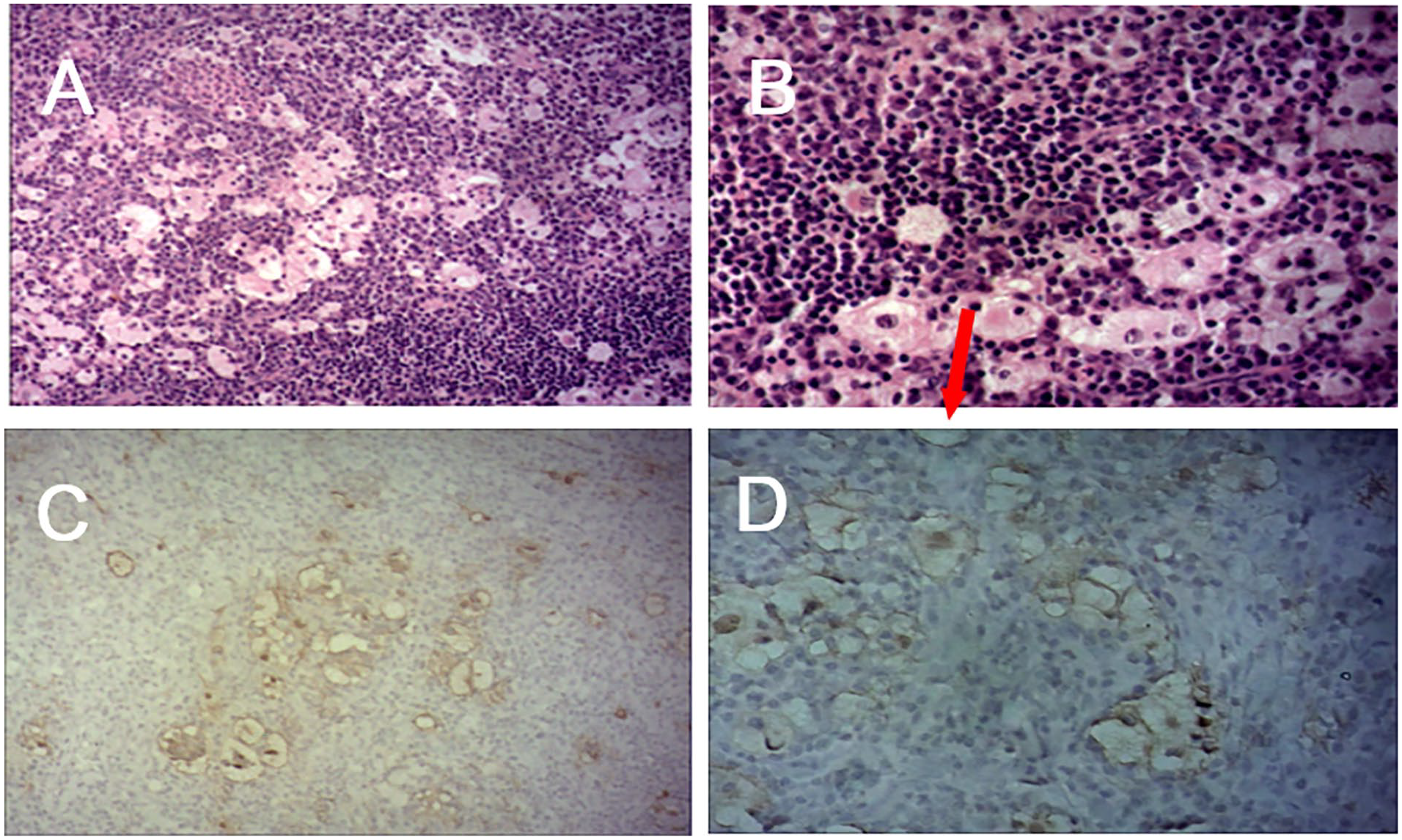
(A) 200× and (B) 400× Hematoxylin–eosin staining revealed that in the proliferated fibrocollagen tissue, there was diffuse infiltration of lymphocytes and plasma cells, multiple light staining areas, and lymphocyte migration in the cytoplasm of tissue cells. Immunohistochemical staining of (C) CD68 expression and (D) S100 protein expression in the cytoplasm of tissue cells.
Discussion
Typical RDD is mainly characterized by bilateral, painless cervical lymphadenopathy, accompanied by fever, weight loss, and night sweats. 6 It primarily occurs in children and young adults, with an average onset age of 20.6 years and is mostly reported in Africa. Males are slightly more likely to be affected, with a male-to-female ratio of 1.4:1. 7 On the other hand, RDD without nodal involvement generally occurs in elderly patients.8,9 This case is an extremely rare occurrence of isolated RDD in soft tissue, which is one of the diagnostic challenges in this disease. In 1990, Foucar et al 7 reported that among 423 RDD patients, only 13 cases (3%) had RDD without lymph node involvement in soft tissue.
The pathogenesis of RDD is not yet clear, and it may be related to viral infections, autoimmune, or genetic mutations.10,11 Diagnosis mainly relies on histopathological and immunohistochemical examinations rather than clinical and imaging manifestations. 12 As shown in the figures, nasal endoscopy and imaging examinations of the patient can be easily misdiagnosed as nasal tumors. The histopathological characteristics of RDD are lymphocytes that can be seen in the cytoplasm of tissue cells, appearing typical streaming or phagocytosis of lymphocytes. The immunohistochemical phenotype shows positive for CD68 and S100, and negative for CD1a.
RDD is usually self-limited and has a good prognosis, with approximately 50% of cases reported to be in spontaneous remission. 13 There is an almost 10% mortality rate is due to complications, infection, and amyloidosis. According to the consensus of experts on the diagnosis and clinical management of RDD in 2018, 14 solitary extranodal RDD or lesions with respiratory symptoms, skull, spine, or paranasal sinuses can be surgically removed. In this case, considering the patient’s specific condition, surgical treatment was chosen with complete excision of the affected tissue, resulting in good recovery at the operated site with no recurrence observed after 3 months. For patients with multifocal extranodal lesions that cannot be surgically resected, systemic treatment may be necessary. Currently, there is no standard treatment regimen for systemic therapy, which may include corticosteroids, sirolimus, radiation therapy, chemotherapy, and immune-modulating therapy. 14 For now, only scattered evidence was shown to support the exact relationship between prognosis and potential molecular changes. The prognosis of RDD also varies. Based on previous research, among 14 patients with extranodal RDD in the head and neck region, 2 (14.3%) died, and 6 (4.8%) of 126 patients with nasal RDD died from the disease.15,16 Therefore, targeted next-generation sequencing of the mitogen-activated protein kinase mutations can be considered in severe or refractory cases. If a driver gene mutation is detected, targeted therapy should be considered. 14
Footnotes
Authors’ Note
This article has not been published or submitted to any journal or meeting. Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Data Availability
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Project funds (Municipal Schools (Institutes) and Enterprises Joint Funding Theme, Guangzhou Municipal Health Commission Basic and Applied Basic Research Project in 2023 (2023A03J0488)).