
Abstract
Immunoglobulin G4-related disease (IgG4-RD) is a novel clinical disease entity characterized by elevated serum IgG4 concentration and tumefaction or tissue infiltration by IgG4+ plasma cells. 1 We report the case of a 56-year-old man who presented with nasal obstruction for 5 years. Rhinoscopy revealed hypertrophy and sclerosis of the inferior turbinate, whereas computed tomography revealed inflammation of the anterior ethmoid sinus and frontal sinuses. An endoscopic inferior turbinectomy was performed, and IgG4-RD was definitively diagnosed based on the histopathological features of the turbinate tissue. Prednisolone was administered postoperatively. IgG4-RD presenting with hypertrophy and sclerosis of the inferior turbinate is rare. Awareness of IgG4-RD originating in the sinonasal cavity is essential to avoid delayed diagnosis.
Introduction
IgG4-related disease (IgG4-RD) was first described in 2001 by a Japanese scholar as “sclerosing pancreatitis”. 2 IgG4-RD has been described in nearly every organ system, including the salivary glands, periorbital tissues, lymph nodes, lungs, kidneys, breast, prostate, thyroid, and biliary tree. 3 IgG4-RD is typically found in the head and neck region, particularly the sub-mandibular and parotid glands, orbit, and thyroid. 4 Chronic rhinosinusitis (CRS) is common in patients with IgG4-RD and is closely associated with IgG4-related ophthalmic and allergic manifestations. 5 However, IgG4-RD mediated sinonasal disease is rarely reported. Here, we report a case of IgG4-RD presenting with hypertrophy and sclerosis of the inferior turbinate.
Case report
Here, we report the case of a 54-year-old male presenting with nasal obstruction for 5 years. In the last year, nasal obstruction symptoms gradually worsened, accompanied by sleep snoring, frequent sneezing, and a runny nose. He used the intranasal spray, but his symptoms worsened. Therefore, he came to our hospital for surgery. Rhinoscopy revealed hypertrophy of the inferior turbinate, slightly swollen nasal mucosa, and a very restricted nasal cavity (Figure 1A and 1B). Computed tomography (CT) showed hypertrophy of the inferior turbinate, as well as thickening of the anterior ethmoidal and frontal sinuses, but with no bone destruction (Figure 1E and 1F). There was no significant increase in the percentage of eosinophils in the peripheral blood. The allergic reaction test came back negative. Rhinoscopy revealed hypertrophy of the inferior turbinate and swollen nasal mucosa. A: right nasal cavity B: left nasal cavity. E-F: Computed tomography (CT) showed hypertrophy of the inferior turbinate, with thickening of the anterior ethmoidal and frontal sinuses, but no bone destruction. C: incision of the anterior attachment of the inferior turbinate D: excision partial inferior turbinate, the fibrosis, and sclerosis of the inferior turbinate tissue.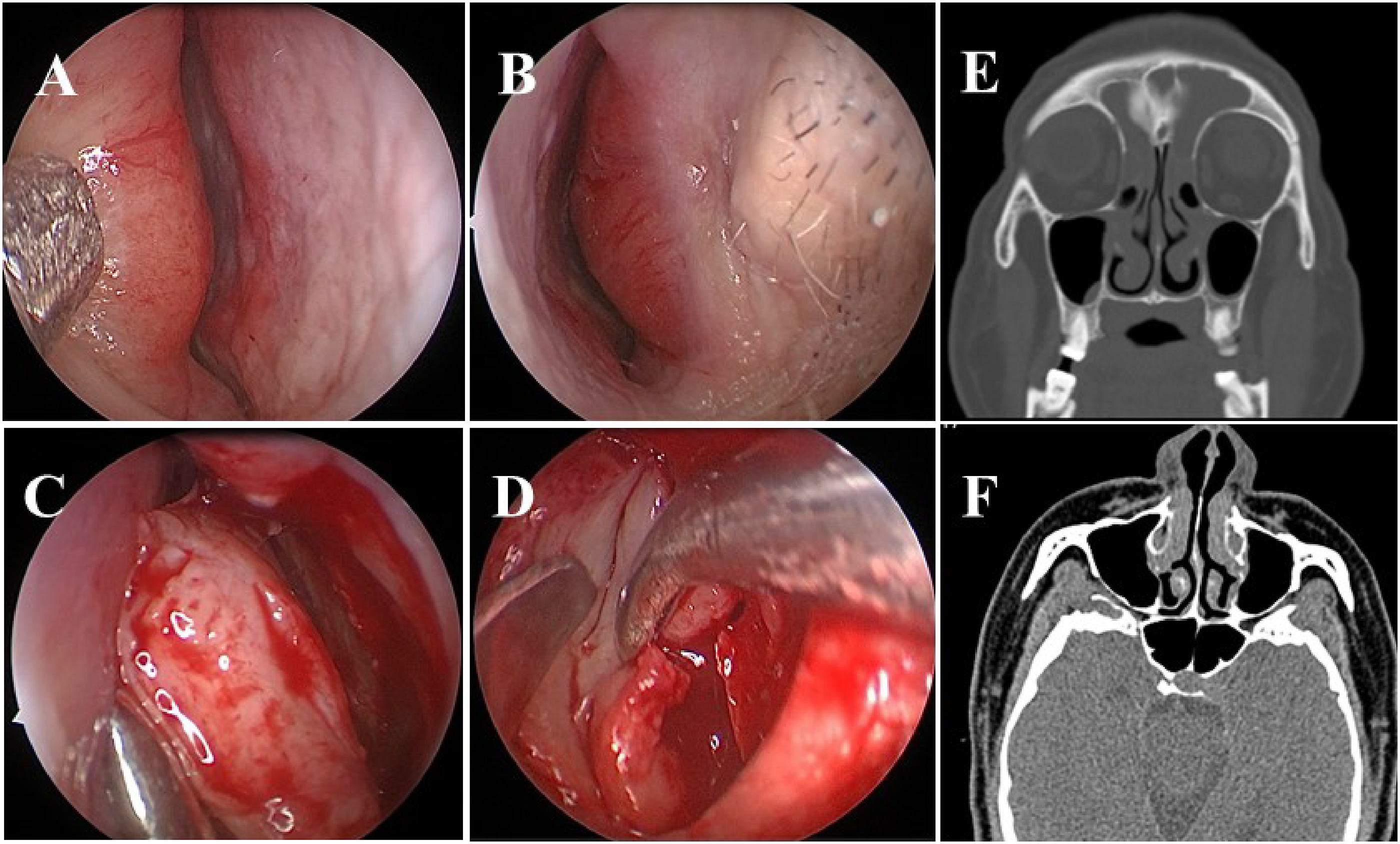
To dilate the nasal cavity, we chose to perform an endoscopic endonasal surgery with inferior turbinectomy. We briefed the patient about the type of surgery, the risks involved, and any potential complications, and he gave his informed consent. During surgery, we used cotton with adrenaline to constrict the nasal cavity for 10 minutes with, and there was no change in the inferior turbinate at all. Following surgical incision of the anterior attachment of the inferior turbinate and separation from the bone, fibrosis and sclerosis of the inferior turbinate tissue were visible (Figure 1C and 1D). We performed a partial inferior turbinate excision and carried out a pathological examination. Histopathological sections revealed a dense lymphoplasmacytic infiltrate, a storiform pattern of fibrosis, obliterative phlebitis, and IgG4 + plasma cells > 100 cells per high-power field, with a ratio of IgG4 + /IgG plasma cells > 40% (Figure 2). The serum IgG4 concentration was 2624.4 mg/L and was above the reference range (39.2–864.0) mg/L. Histopathological sections showed a dense lymphoplasmacytic infiltrate, a storiform pattern of fibrosis, obliterative phlebitis, and IgG4 + plasma cells > 100 cells per high-power field, with a ratio of IgG4 + /IgG plasma cells > 40% original magnification×200.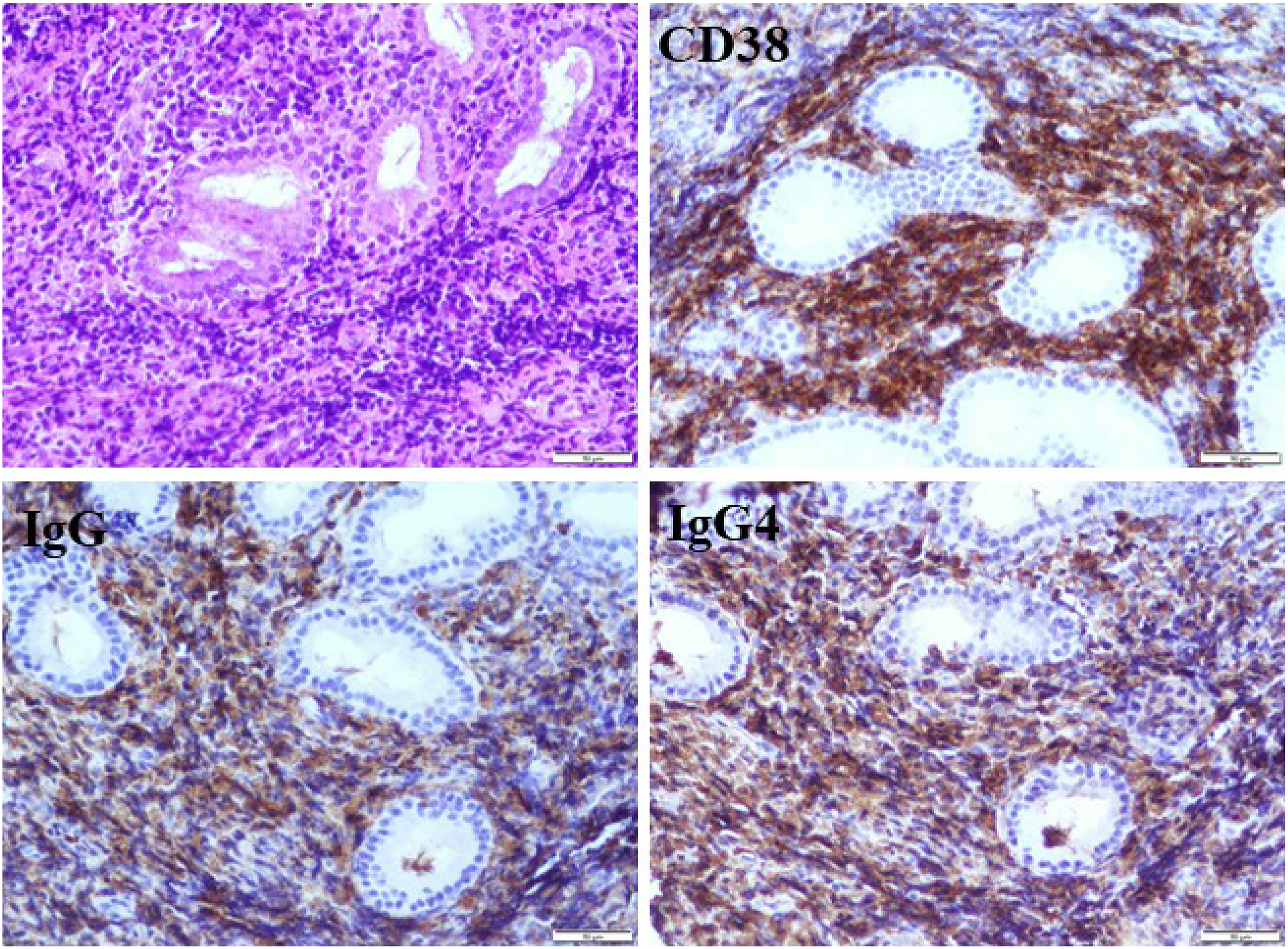
The patient was referred to a rheumatologist to be evaluated for rheumatologic autoimmune disorders. No other abnormal findings were observed. A series of tests, including chest CT, abdominal Color Doppler, parotid and submandibular gland Color Doppler, and serum biochemistry, were performed, and no further other organ manifestation of IgG4-RD was discovered. Furthermore, the patient had no other clinical symptoms. Therefore, a definitive diagnosis of IgG4-RD was established.1,6
Postoperatively, we prescribed a starting prednisolone dose of 30 mg daily. After 2 weeks, the inferior turbinate shrank and all clinical symptoms were completely resolved. After 4 weeks, serum IgG4 concentration returned to normal, the dose was reduced, and maintained at a low level based on clinical response.
Discussion
IgG4-RD originating in the sinonasal cavity is rare. Takano K et al 7 described the clinical features of patients with IgG4-RD complicated with CRS in Japan. Only 4 out of seventy nine cases underwent nasal sinus membrane biopsy, and a definitive diagnosis was made in the majority of the cases by involved organs biopsy from the extra-nasal cavity. Gao Y et al 5 identified a total of thirty patients (65.2%) who had IgG4-RD complicated with CRS, demonstrating a close association between ocular lesions with IgG4-RD and CRS. The orbital lesion may be contiguous as a result of inflammation lesion spreading from the nasal passages or paranasal sinuses due to the orbit’s close anatomical proximity. There are currently no documented definite diagnostic criteria for IgG4-RD affecting the sinonasal cavity.
Chronic rhinitis and CRS are highly prevalent in China, and it is extremely difficult and critical to distinguish patients who have systemic disorders from those who do not. The primary issue with this patient was nasal congestion, a common symptom of chronic rhinitis, leading to misdiagnosis and missed diagnosis.
In this case, the patient complained of perennial sneezing and a runny nose, and anterior rhinoscopy revealed a slight swelling of the nasal mucosa. The peripheral blood eosinophil count did not increase, and the allergy test was negative. Perhaps systemic and autoimmune disorders should have been considered at that time. Additionally, endoscopic examination provided critical information. Rhinoscopy revealed hypertrophy of the inferior turbinate, which remained unchanged following adrenaline cotton. The diagnosis was confirmed by surgery and pathology, and we also discovered fibrosis and sclerosis during surgery through the morphology of the turbinate. This will also help our rhinologists in future consideration of IgG4-RD.
Previously published research indicated that individuals with IgG4-RD had a higher risk of developing CRS and that some patients experienced multiple episodes of sinusitis. Furthermore, previous research indicated that CRS was committed as a component of the patient’s implicated organs. Although we did not discover any other significant organ symptoms, the patient had a 5-year history of rhinitis. Perhaps rhinitis or CRS are the initial manifestations of IgG4-RD.
Therefore, this case may enable rhinologists to diagnose IgG4-RD earlier and has prompted calls for the development of precise diagnostic criteria for IgG4-RD affecting the sinonasal cavity.
Conclusion
IgG4-RD can originate in the sinonasal cavity. Although the symptoms are common symptoms of chronic nasal illnesses, there are certain unique clinical features.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.