
Abstract
Objective: This study aims to explore the effects of laryngopharyngeal reflux disease (LPRD) and proton pump inhibitor (PPI) treatment on Eustachian tube function in patients with obstructive sleep apnea (OSA). Methods: The Eustachian tube score-7 (ETS-7) was observed before and after PPI treatment in the control group, OSA only group, and OSA + LPRD group. Results: Age, sex, smoking history, and drinking history showed no differences among 3 groups (P > .05). The body mass index (BMI) in the control group was lower than that in other groups (P < .017). Before PPI treatment, the abnormality rate of ETS-7 in the OSA + LPRD group statistically differed from that in the control group and the OSA only group (P < .017). After PPI treatment, the abnormality rate of ETS-7 in the OSA + LPRD group exhibited no significant differences compared with that in the control group and the OSA only group (P > .017), and it declined remarkably compared with that before PPI treatment (75% vs 35%, χ2 = 13.334, P = .001). Moreover, the multivariate analysis revealed that only LPRD had an independent correlation with the abnormality of ETS-7 (OR = 1.245, 95% CI: 1.759–6.861, P = .000). Conclusion: In view of its high incidence in OSA patients, LPRD may be a considerable factor for the high incidence of abnormality rate of ETS-7 in OSA patients, and PPI therapy is of significant value in improving Eustachian tube function in OSA patients with LPRD.
Keywords
Introduction
Reflux diseases are classified into gastroesophageal reflux disease (GERD) and laryngopharyngeal reflux disease (LPRD). LPRD is defined as a variety of symptoms caused by a reflux of gastrointestinal contents into the upper esophageal sphincter. 1 With such common clinical symptoms as glob uspharyngeus, hoarseness, and cough, LPRD often threatens the quality of life of patients, showing an incidence rate of 3.8-56.88% in China. 2 Obstructive sleep apnea (OSA) is a type of sleep disorder caused by partial or complete obstruction of the upper airway, which can be evaluated by sleep apnea-hypopnea index (AHI), with an incidence rate of 6–17%. 3 Eustachian tube dysfunction (ETD) refers to the mechanical obstruction of the Eustachian tube or motile mucociliary impairment, which is the basis of many diseases of the middle ear.
Ahmed et al’s research confirmed that the negative pressure of the middle ear is related to the negative pressure of the nasopharynx in the pathophysiological process of OSA in both children and adults. 4 Magliulo’s study showed that Eustachian tube blockage or delayed opening being found in most adults with OSA, with the concurrence rate of 20%. 5 Meanwhile, since LPRD can lead to the pathophysiological changes of the Eustachian tube, the concurrence rate of ETD and LPRD is relatively high. 6 Moreover, it has been widely recognized and accepted that reflux diseases (including GERD and LRPD) display high incidence rates in OSA patients in recent years, and the concurrence rate of OSA and LPRD is 40.3–64.3%. 7
Studies have shown that OSA patients have an increased incidence rate of ETD. However, the role of LRPD, a secondary or concomitant disease of OSA, in the occurrence of ETD in patients with OSA has been rarely studied. In this study, therefore, the effects of LRPD and its PPI treatment on Eustachian tube function in OSA patients were probed into.
Patients and methods
Research subjects
OSA and LPRD patients admitted to the Department of Otorhinolaryngology Head and Neck Surgery and Sleep Medicine Center in Beijing Anzhen Hospital, from August 2019 to December 2020 were collected.
The inclusion criteria for inpatients and outpatients with OSA and/or LPRD involved: (1) patients aged > 18 years old and (2) those diagnosed with OSA and/or LPRD with a course of more than 3 months.
The exclusion criteria were set as follows: (1) patients with symptoms related to the upper airway infection and/or allergic diseases such as allergic rhinitis within 3 months of the examination; (2) those with history of head and neck surgery or radiotherapy, including OSA surgery; (3) those with history of ear disease surgery or tympanic membrane perforation; (4) those who had taken over-the-counter drugs, such as intranasal steroids, decongestants, or antihistamines; (5) those who had received continuous positive airway pressure (CPAP); or (6) those who with omeprazole allergy or contraindications.
Volunteers were enrolled from the Physical Examination Center of Anzhen Hospital in the same period as control group based on the following inclusion criteria: (1) people aged > 18 years old, (2) those with no history of reflux diseases (including GERD and LPRD), and (3) those with no history of OSA.
All the participants to be observed signed the informed consent in line with the Declaration of Helsinki before observation. This study was approved by the Ethics Committee of the hospital (Approval No.: 2019052X).
Diagnostic criteria and grouping
According to the diagnostic criteria of AHI > 5, OSA was diagnosed by polysomnography (PSG), 8 Type III, in the Sleep Medicine Center of Anzhen Hospital. Diagnosis of LPRD accorded with the diagnostic criteria of our country (2015), 9 which including RSI (reflux symptom index, RSI) and/or RFS (reflux finding score, RFS). The RSI and RFS were examined by 2 experienced physicians at the same time. The RSI scale includes 9 symptoms such as hoarseness, throat clearing, excessive phlegm, or post-nasal drip, and it adopts a scoring of 0–5 points for conditions from no problem to severe problem, with a total score of 45 points. The RFS scale includes 8 laryngoscopic signs such as false vocal cords, laryngeal edema, erythema, or hyperemia, with a total score of 26 points. Those with RSI > 13 points, RFS > 7 points, and the course of disease > 3 months were included in the study.
In the OSA + LPRD group, the RSI and RFS were executed separately at the beginning of the study and at the ending of the PPI treatment, by the same physician.
The control group underwent PSG examination to rule out OSA.
In light of the incidence of OSA and LPRD, the subjects to be observed were divided into 3 groups, namely, the control group, OSA only group, and OSA + LPRD group.
PPI treatment: OSA patients with LPRD received PPI treatment twice a day for 12 weeks(omeprazole, 20 mg twice a day, half an hour before breakfast and dinner), and they were given advice for living under the condition of LPRD, 9 such as losing weight, quitting smoking, giving up alcohol, avoiding chocolate and carbonated beverages, and avoiding eating at midnight.
The research process is as shown in Figure 1. Study flow chart.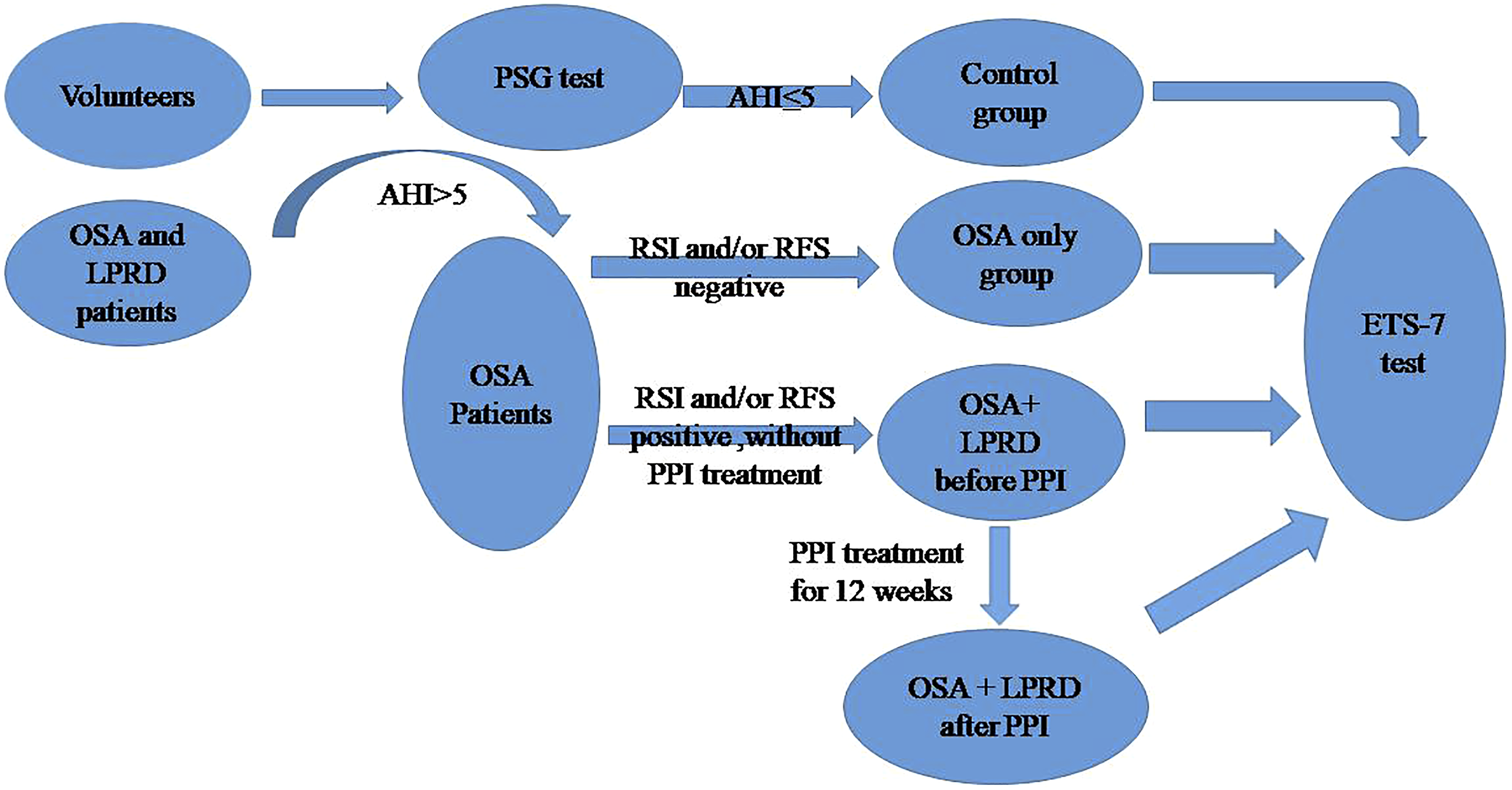
Routine otolaryngological examinations including upper airway and the ear, mainly performed by endoscopy, were carried out before study.
Abbreviations: LPRD, laryngopharyngeal reflux disease; OSA, obstructive sleep apnea; PPI, proton pump inhibitor; ETS-7, Eustachian tube score-7; PSG, polysomnography; RSI, reflux symptom index; RFS, reflux finding score; AHI, apnea-hypopnea index.
Data collection and examination methods
Firstly, characteristics of the observed, including sex, age, body mass index (BMI), smoking history, drinking history, Eustachian tube function, LPRD symptoms, and rhinomanometry, were collected. An acoustic rhinometer (model A1) and a nasal resistance meter (model NR6; GM Instruments) were employed to measure rhinomanometry; routine otolaryngological examinations including upper airway and the ear, mainly performed by endoscopy, were carried out.
Secondly, Eustachian tube function was evaluated by Eustachian tube score-7 (ETS-7). Based on Eustachian tube manometry, ETS-7 is a valid and quasiobjective method to investigate ETD, accounting for acoustic impedance and Valsalva’s and Toynbee’s clinical symptoms. 10 By ETS-7, Eustachian tube function is scored 0–14 points, and a score of ≤ 7 points meets the diagnostic criteria for ETD. The literature has shown that the sensitivity and specificity of ETS-7 in diagnosing ETD are 91% and 86%, respectively. 11 A tubomanometer from La Diffusion Technique Francaise was employed for TMM in our study, and the patients were divided into the normal group, the unilateral ETD group, and the bilateral ETD group according to the results of ETS-7.
All participants completed the ETS-7 score at the beginning of the experiment; the OSA +LPRD group completed it again after 12 weeks of PPI treatment.
Statistical analysis
SPSS 23.0 (IBM) was adopted for statistical analysis. Continuous variable data were expressed as mean ± standard deviation, and subjected to normal distribution test and LSD variance analysis. Besides, categorical data were expressed by n (%), and data analysis and/or paired data detection was performed using the χ2 test. Fisher’s exact probability method was utilized if the theoretical frequency was less than 5. Furthermore, ETD-related factors were analyzed via univariate and multivariate logistic regression methods (unilateral and bilateral ETD shown in ETS-7). Statistical significance was set at P < .05, and adjusted at P < .017 in comparisons among groups.
Results
Characteristics of the observed
Characteristics of the observed.
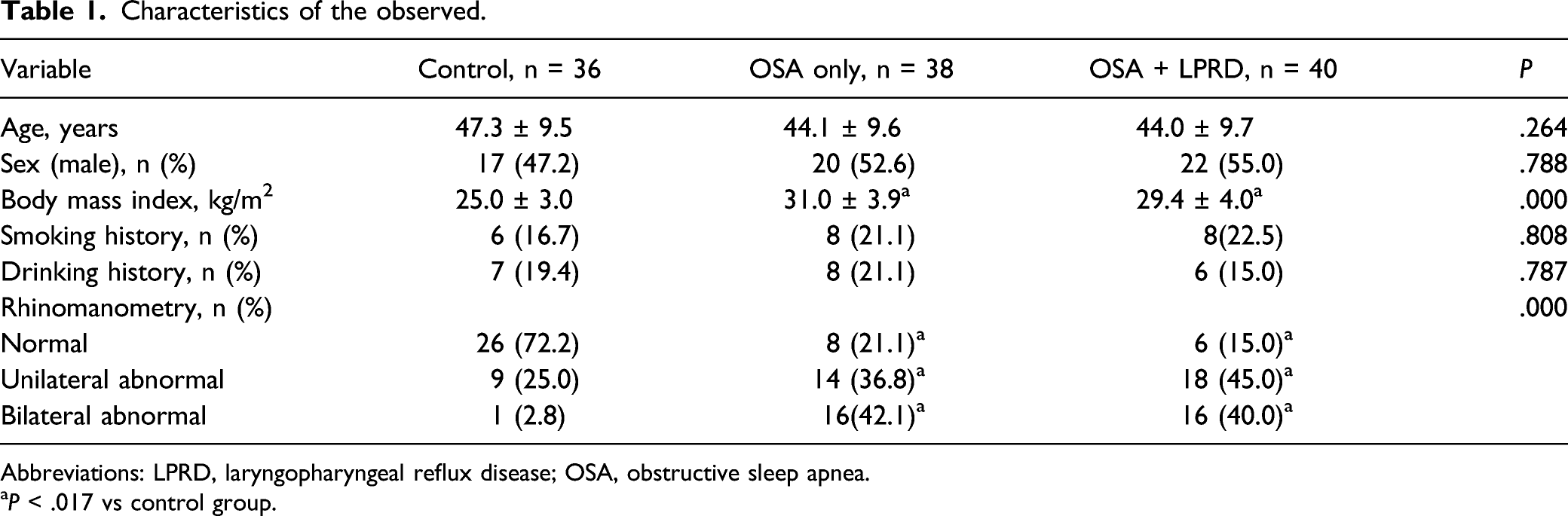
Abbreviations: LPRD, laryngopharyngeal reflux disease; OSA, obstructive sleep apnea.
aP < .017 vs control group.
Laryngopharyngeal reflux disease and Eustachian tube function
In our study, after 12 weeks of PPI treatment twice a day in the OSA with LPRD group, with RSI > 13 points and/or RFS > 7 points as the diagnostic criteria, 25 of 40 patients were relieved, showing an effective rate of 62.5%.
ETS-7 results before treatment in each group.
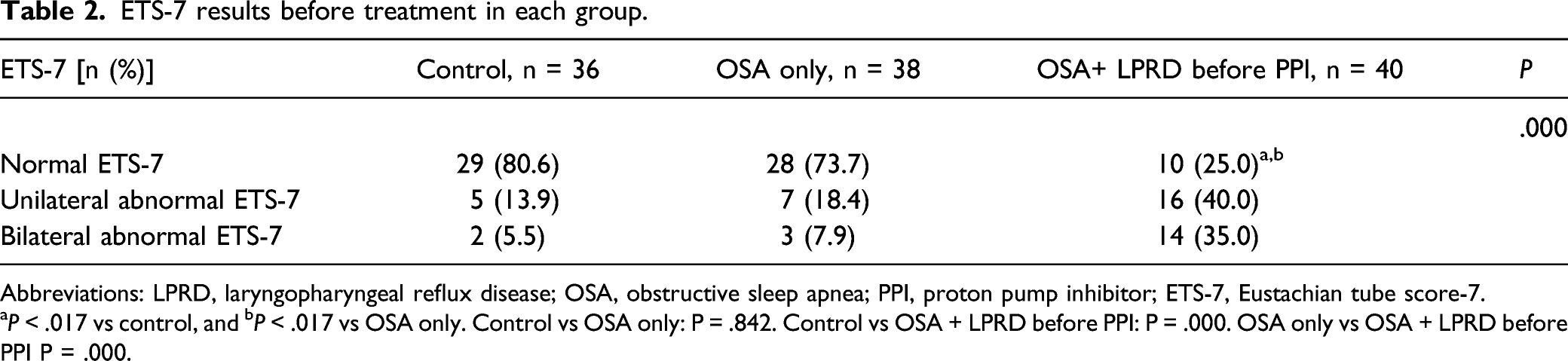
Abbreviations: LPRD, laryngopharyngeal reflux disease; OSA, obstructive sleep apnea; PPI, proton pump inhibitor; ETS-7, Eustachian tube score-7.
P < .017 vs control, and bP < .017 vs OSA only. Control vs OSA only: P = .842. Control vs OSA + LPRD before PPI: P = .000. OSA only vs OSA + LPRD before PPI P = .000.
ETS results after PPI treatment in each group.
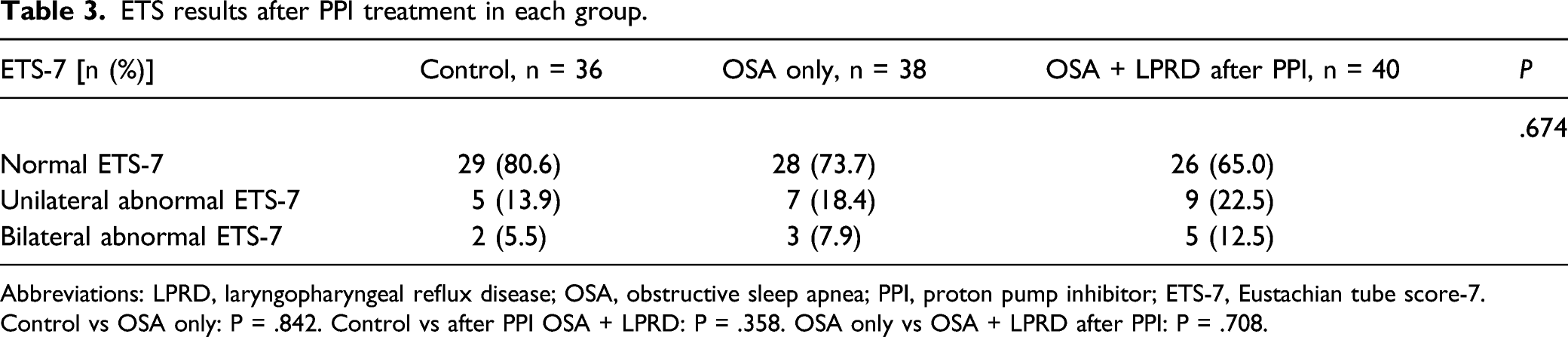
Abbreviations: LPRD, laryngopharyngeal reflux disease; OSA, obstructive sleep apnea; PPI, proton pump inhibitor; ETS-7, Eustachian tube score-7.
Control vs OSA only: P = .842. Control vs after PPI OSA + LPRD: P = .358. OSA only vs OSA + LPRD after PPI: P = .708.
ETS-7 results before and after PPI treatment in the OSA + LPRD group.

Abbreviations: LPRD, laryngopharyngeal reflux disease; OSA, obstructive sleep apnea; PPI, proton pump inhibitor before vs after PPI treatment: P = .001.
Logistic regression analysis
Univariate and multivariate analyses of factors related to ETD.
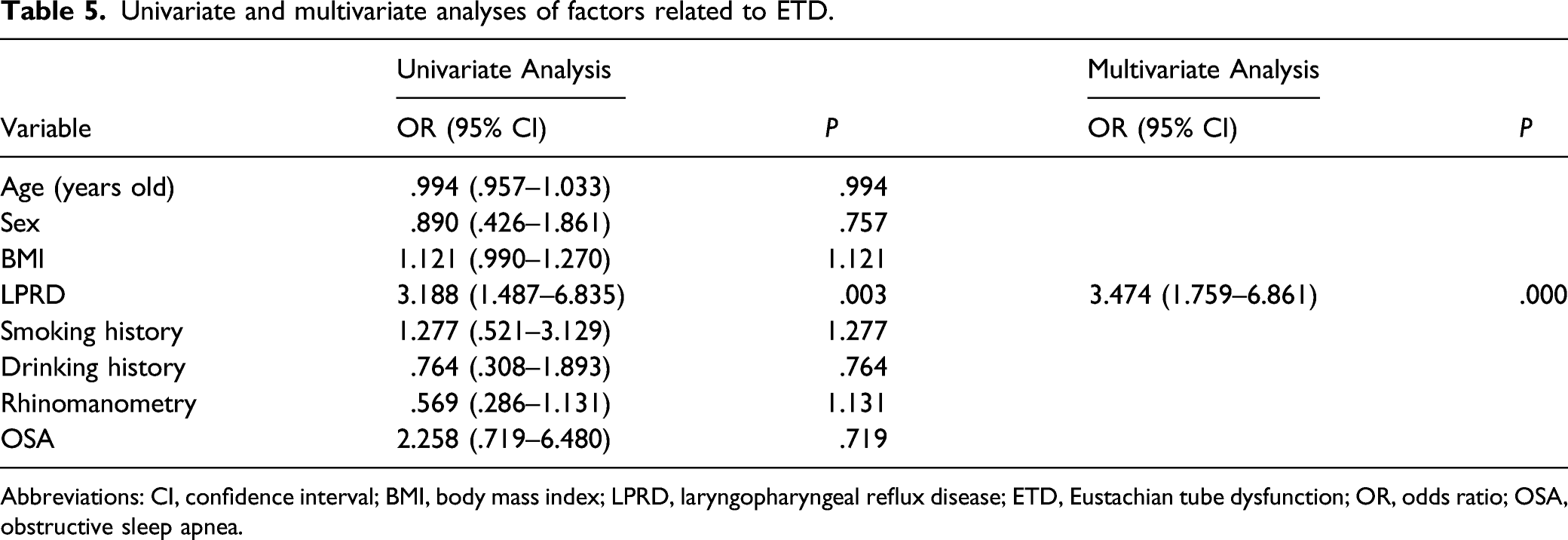
Abbreviations: CI, confidence interval; BMI, body mass index; LPRD, laryngopharyngeal reflux disease; ETD, Eustachian tube dysfunction; OR, odds ratio; OSA, obstructive sleep apnea.
Discussion
The purpose of this study is to investigate the effects of LPRD and PPI treatment on Eustachian tube function in OSA patients.
The results showed that the difference in the incidence rate of ETD between the OSA only and control group was not statistically significant (P = .842, Table 2). With ETS-7 as a diagnosis method, it was found that before PPI treatment, the incidence rate of ETD in the OSA + LPRD group was higher than that in the OSA only group and the control group, showing statistically significant differences (control vs OSA + LPRD group: P = .000, OSA only vs OSA + LPRD group: P = .000, Table 2). The above results indicated that LPRD may be a crucial factor for the high incidence rate of ETD in OSA patients.
The association between LPRD and OSA has been recognized by the academic circles.12,13The meta-analysis of Magliulo et al. denoted that the incidence rate of LPRD in OSA patients was very high (about 45.2%), 14 and the occurrence of LPRD was not related to the severity of OSA. After the control of the confounding factors such as obesity, age, sex, race, nasal sinus, asthma, lung diseases, and inflammatory diseases,14,15 OSA patients exhibit a higher incidence rate of reflux diseases still. Similar to the mechanism of high GERD in OSA patients, the changes of the circulatory system and airway dynamics in the pathophysiological process of OSA, especially the huge pressure difference inside and outside the thoracic cavity at the end of inspiration, result in the relaxation of the lower esophageal sphincter and laryngeal sensory dysfunction, thereby leading to the reflux of gastric contents including liquid, gas, and acid and non-acid contents. As LPRD involves a chronic process, its long-term cough, hoarseness, and globus pharyngeus trigger chronic edema and hyperplasia of the throat mucosa, which in turn may aggravate OSA.
The research of Magliulo et al. 14 demonstrated OSA was closely associated with ETD. In theory, the aerodynamic changes of nasal cavity and nasopharynx and the impairment of mucosal function induced by hypoxia and inflammation may induce or aggravate ETD. Rare reports have revealed the correlation between OSA and ETD, and in these existing reports, the high incidence rate of LPRD in OSA patients, a considerable factor for Eustachian tube mucosa injury, has not been studied.
Studies of Kim et al.16,17 showed that LPRD had a close correlation with ETD; Karyanta et al. reported that the prevalence of otitis media with effusion in the LPRD group was 4.5 times that in the non-LPRD group. 17 The results of this study displayed that the incidence rate of ETD in the OSA + LPRD group was higher than that in the control group and the OSA only group before PPI treatment. After PPI treatment, LPRD was alleviated in the OSA + LPRD group, showing an effective rate of 62.5% (25 of 40 patients), and the ETS-7 results were remarkably elevated (before vs after PPI: 75% vs 35%, P = .001, Table 4) too. Simultaneously, after PPI treatment, the incidence rate of ETD in the OSA + LPRD group was not statistically significantly different from that in the control group and the OSA only group (control vs OSA + LPRD group after PPI: P > .017, OSA only vs OSA + LPRD group after PPI: P > .017, Table 3), which are consistent with the above research results. All the above studies suggested that LPRD is likely to be a considerable factor for the high incidence rate of ETD in OSA patients and that PPI treatment is able to relieve ETD in OSA patients with LPRD.
The tissue structure of the laryngeal mucosa differs from that of the esophagus mucosa, and the 2 dramatically differ from each other in the defense mechanism. The esophageal mucosa can tolerate acid reflux at least 50 times a day, while the dysfunction of the laryngeal mucosal epithelium will occur after acid exposure 3 times a week. 18 When reflux diseases, especially LPRD, occur, the reflux of gastric contents, dominated by the stimulation of pepsin on the mucosal epithelium, can directly trigger the inflammation and adhesion of the Eustachian tube mucosa, thus increasing the risk of ETD. 17
The clinical treatment of LPRD is still inconclusive due to the lack of diagnostic gold standard/difficulty in clinical application and the existence of factors such as non-acid reflux. However, PPI treatment is a common clinical treatment method. Research by Park et al. 19 showed that the effective rate of PPI treatment twice a day is 50% at 2 months, and 72% at 4 months. The effective rate at 3 months in our study is 62.5%, which is similar to this.
The PPI treatment for the elderly can last for 2 years.18,20 In the existing studies, the effect of PPI on refractory ETD or secretory otitis media has been widely explored. Brunworth 21 observed and compared the nasopharyngeal pH values between patients with ETD and normal people, and found that although no difference in the nasopharyngeal pH was detected between the 2 groups of patients (pH = 6.90 in ETD patients vs 7.07 in the control group, P = .30), there were more nasopharyngeal reflux events in the ETD group (2.3 ± 1.6 vs .8 ± 1.2, P = .002). 21 In spite of the fact that the nasopharyngeal pH value was not changed by these refluxes, these refluxes probably exert effects on the pathogenesis of ETD. It can be concluded that ETD is more likely to be associated with a higher incidence rate of nasopharyngeal reflux events. In the present study, the difference in the abnormality rate of ETS-7, namely, ETD, in the OSA + LPRD group before and after PPI treatment was statistically significant (75% vs 35%, P = .001, Table 4), accompanied by 62.5% improvement rate of LPRD; this confirmed the close relationship between LPRD and ETD from the therapeutic view.
At the end of the statistical process, the multivariate analysis was carried out, which demonstrated that LPRD was an independent risk factor for the ETD (OR = 1.245, 95% CI: 1.759–6.861, P = .000, Table 5). The reason may be that the actual chemical damage to the structure of nasopharynx and Eustachian tube, especially the structure of the mucosa, caused by the stomach contents in LPRD further exacerbates the existing OSA-induced motile cilia impairment or mechanical obstruction. 18
Conclusion
It was demonstrated by this study that LPRD may be a bridge factor for the high incidence of ETD in OSA patients, considering its high incidence in OSA. PPI treatment is of significant value in improving Eustachian tube function in OSA patients with LPRD.
Methodological considerations/limitations
The diagnosis of LPRD was made only with clinical tests in the absence of an esophageal PH impedance test, which was a limitation of this study. Although there is no consensus regarding standardization of the diagnostic criteria, an increasing number of authors used multichannel intraluminal impedance–pH monitoring, and new tests such as the salivary pepsin dosage for the diagnosis of LPRD are continuously applied.22-24 Another limitation is that being a preliminary exploration, the present study could not establish causality. It is still necessary to conduct further prospective research with a large sample size and multi-center data to examine this point.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ Note
Informed consent was obtained from all individual participants included in the study. The study was approved by the ethics committee Of Peking Anzhen Hospital. The study was carried out in accordance with the principles of the Declaration of Helsinki.