
Abstract
Objectives:
To explore the effect of gastroesophageal reflux disease (GERD) on Eustachian tube function in patients with obstructive sleep apnea (OSA).
Methods:
This was a cross-sectional study. The patients were divided into 4 groups according to OSA and GERD: OSA+GERD group; OSA-only group; GERD-only group; and normal control group.
Results:
There were no differences among the 4 groups regarding age, sex, smoking history, and alcohol history (all P > .05). The patients in the OSA and OSA+GERD groups had a significantly larger body mass index than those in the control and GERD-only groups (all P < .05). The proportions of patients with abnormal ETS-7 and ETD-Q results were higher in the GERD and OSA+GERD groups compared to the control group (P < .008). There were no significant differences in ETS-7 and ETD-Q between the control and the OSA-only groups (P > .008). The multivariable analysis showed that only GERD was independently associated with abnormal ETS-7 results (odds ratio = 3.090, 95% CI: 1.332-7.169, P = .009).
Conclusion:
Given the high concomitance rate in patients with OSA, GERD might be an important association factor of Eustachian tube dysfunction in patients with OSA.
Keywords
Introduction
Obstructive sleep apnea (OSA) is a sleep disorder characterized by repetitive complete or partial (hypopnea) upper airway obstructions, despite associated respiratory effort causing repetitive arousals and sleep fragmentation. The prevalence of OSA, as defined as an apnea–hypopnea index (AHI)
Gastroesophageal reflux disease (GERD) is a condition that develops when the reflux of stomach contents into the esophagus causes troublesome symptoms and/or complications. The prevalence of GERD ranges from 2.5% to 7.8% in East Asia to 8.7% to 33.1% in the Middle East. 2 Gastroesophageal reflux disease increases the risk of esophageal cancer and is associated with reflux cough and apnea. 3 Eustachian tube dysfunction (ETD) is the inability of the Eustachian tube to protect the middle ear from pathogens, to ventilate the middle ear adequately, and to drain the secretions from the middle ear. 4
Regarding ETD, ETD is associated with a high occurrence of reflux events that may affect the pathogenesis of ETD (2.3 ± 1.6 vs 0.8 ± 1.2 events). 5 In addition, Eustachian tube blockage or delayed opening is found in most adults with OSA. 6
Both OSA and GERD are associated. In patients with GERD, the risk of OSA and poor sleep quality are higher than in controls. 3 After controlling for confounders, a Korean study showed that compared to the control group, OSA was more likely to be found in patients with GERD, and this association is independent of age, sex, ethnicity, sinonasal/laryngopharyngeal obstructive/inflammatory disorders, obesity, asthma, and lung diseases. 7 On the other hand, the association between GERD and OSA is controversial, but patients with OSA nevertheless have a high incidence of GERD as supported by a large-sample US study. 7 In terms of the causal relationship between GERD and OSA, conflicting results were reported by previous researches; currently, it is widely accepted that the mechanism by which the 2 diseases is associated could be the large negative intrathoracic pressure swings generated during obstructive apneas. 8 Patients with OSA have a high incidence of GERD, independent of known risk factors for GERD. 7
Importantly, there are no studies on Eustachian tube function in patients with OSA but without GERD. In particular, patients with OSA often have GERD, an important factor affecting the function of the Eustachian tube. Therefore, the aim of the present study was to explore the effect of GERD on Eustachian tube function in patients with OSA.
Patients and Methods
Study Design and Patients
Outpatient and hospitalized patients with OSA and/or GERD at the Hospital from November 2018 to June 2019 were enrolled. The study was approved by the ethics committee of the Hospital (2019050X). All patients provided written informed consent prior to any study procedure. The study was carried out in accordance with the principles of the Declaration of Helsinki.
Outpatient and hospitalized patients with OSA and/or GERD were consecutively selected. The inclusion criteria were (1) age
In addition, healthy controls were enrolled for comparison from the population of patients undergoing a routine physical examination. The inclusion criteria were (1) age
Diagnosis Criteria and Grouping
Obstructive sleep apnea was diagnosed at the sleep Center of the Hospital by polysomnography, showing AHI >5. Gastroesophageal reflux disease was diagnosed by gastroenterologists, based on endoscopic findings and clinical questionnaires,
10
without treatment or receiving treatment but with A or C
Data Collection and Examination Methods
Demographic information (sex, age, and body mass index [BMI]), history of present ETD (consecutively left or right and duration), symptoms of GERD, past history (hypertension, diabetes, and otitis), family history, smoking history, drinking history, drugs (nonsteroidal anti-inflammatory drugs, aspirin, proton pump inhibitor, etc), OSA grade, and AHI index were collected. The tympanic membrane examination included tympanic membrane invagination and range of tympanic membrane motion. Rhinomanometry included an acoustic rhinometer (model A1) and a nasal resistance meter (model NR6; GM Instruments) and was performed routinely.
The ETDQ-7 11 and ETS-7 9 were used to assess the Eustachian tubes. ETDQ-7 questionnaire is the most commonly used Eustachian tube symptom score scale, divided into 7 questions, scored according to the subjective situation of the patient (none–mildly–severe degree). The ETDQ evaluates the presence of symptoms such as ear pressure, ear pain, clogged feeling, and ear symptoms when having a cold or sinusitis, popping sounds, ringing, and muffling feeling (each score from 1 to 7, with high scores indicating worst symptoms) and more than 14.5 points were defined as ETDQ abnormal. 11 Because there is no objective data, ETDQ-7 lacks objectivity. Based on Eustachian tube manometry, ETS-7 is a valid and quasiobjective method to investigate ETD, accounting for acoustic impedance and Valsalva’s and Toynbee’s clinical symptoms (from 0 to 14 points), and the cutoff value is 7 points. 9 Eustachian tube manometry was evaluated using a tubomanometer (La Diffusion Technique Française). 6 The patients were divided into normal, unilateral abnormal, and bilateral abnormal ETD, according to ETS-7. 12
Statistical Analysis
Statistical analysis was performed using SPSS version 23.0 (IBM). Continuous data with normal distribution confirmed by the Kolmogorov-Smirnov test are displayed as means ± standard deviation and were analyzed using analysis of variance and the LSD post hoc test. Categorical data are displayed as n (%) and were analyzed using the χ2 test. Univariable and multivariable logistic regression were used to analyze the factors associated with ETD (ETS-7 unilateral abnormal and bilateral abnormal). Statistical significance was set at P < .05; multiple comparisons among groups were adjusted at P < .008.
Results
Characteristics of the Patients
Table 1 presents the characteristics of the patients in 4 groups. There were no differences among the 4 groups regarding age, sex, smoking history, and drinking history (all P > .05). The patients in the OSA and OSA+GERD groups had a significantly larger BMI than those in the control and GERD-only groups (all P < .05). The proportions of patients with abnormal rhinomanometry were higher in the OSA, and OSA+GERD groups had a significantly larger BMI than those in the control and GERD-only groups (all P < .05).
Characteristics of the Patients.
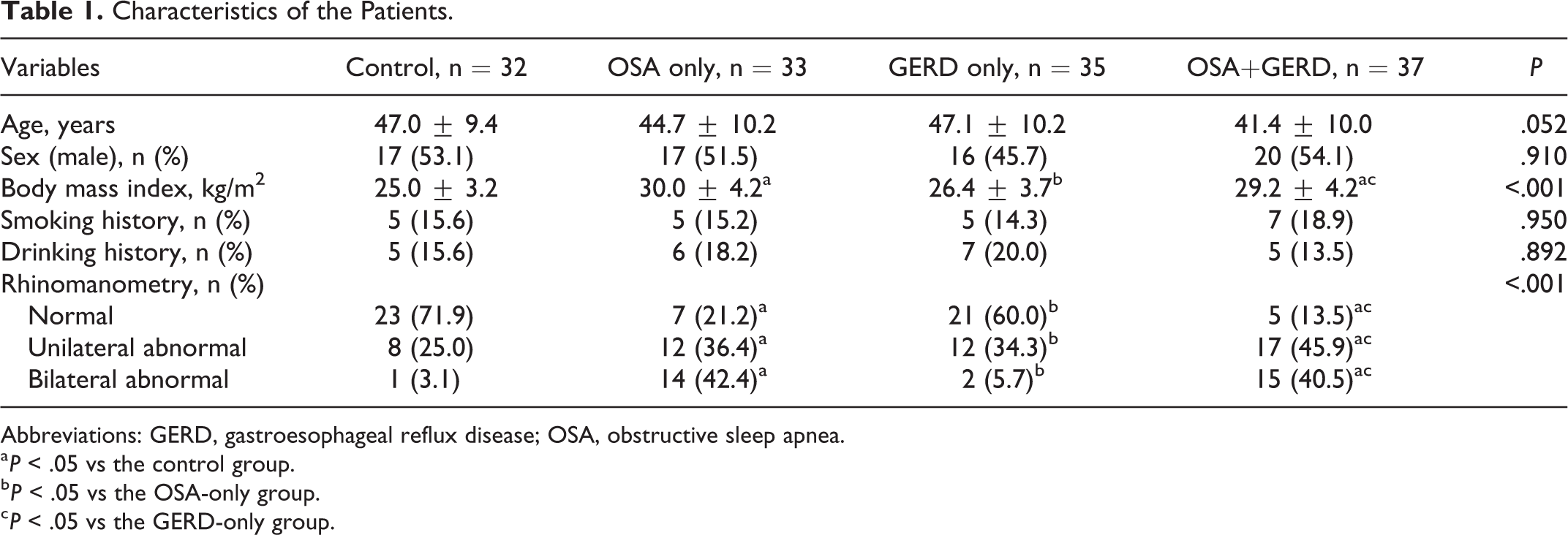
Abbreviations: GERD, gastroesophageal reflux disease; OSA, obstructive sleep apnea.
a P < .05 vs the control group.
b P < .05 vs the OSA-only group.
c P < .05 vs the GERD-only group.
Eustachian Tube Conditions
Tables 2 and 3 present the results of the ETS-7 and ETD-Q, and the pairwise comparisons are presented in the footnotes. The proportions of patients with abnormal ETS-7 results were higher in the GERD and OSA+GERD groups compared to the control group (both P < .008) but not higher than in the OSA-only group (P = .499, P > .008; Table 2). The proportions of patients with abnormal ETD-Q results were higher in the GERD and OSA+GERD groups compared to the control (both P < .008) but not higher than in the OSA-only group (P = .741, P > .008; Table 3). There were no statistically significant differences in ETS-7 and ETD-Q between the control and the OSA-only groups or between the GERD and the OSA+GERD groups (all P > .008).
Results of the ETS-7.a
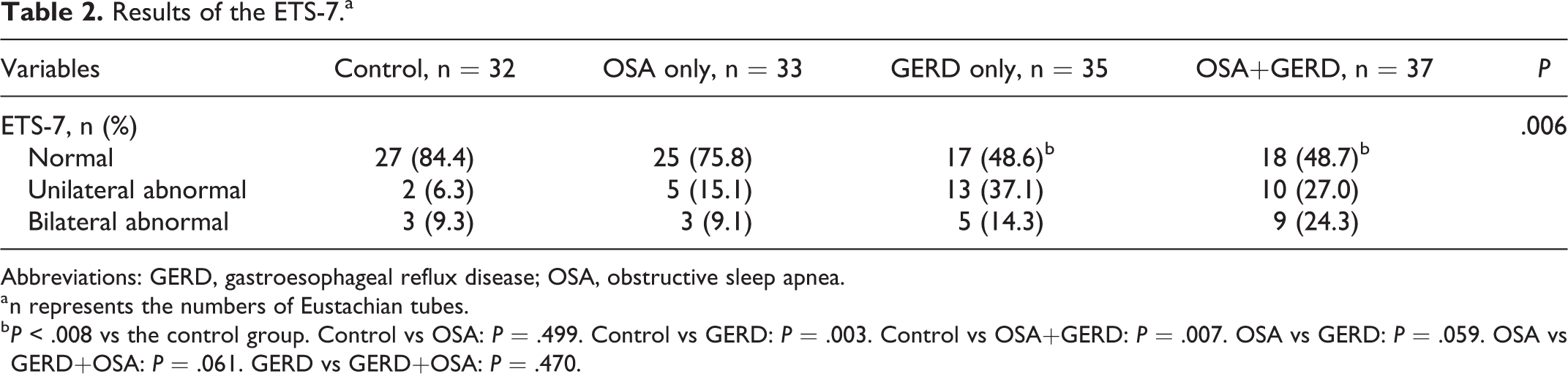
Abbreviations: GERD, gastroesophageal reflux disease; OSA, obstructive sleep apnea.
a n represents the numbers of Eustachian tubes.
b P < .008 vs the control group. Control vs OSA: P = .499. Control vs GERD: P = .003. Control vs OSA+GERD: P = .007. OSA vs GERD: P = .059. OSA vs GERD+OSA: P = .061. GERD vs GERD+OSA: P = .470.
Results of the ETD-Q.a

Abbreviations: GERD, gastroesophageal reflux disease; OSA, obstructive sleep apnea.
a N represents numbers of patients.
b P < .008 vs the control group; Control vs OSA: P = .741. Control vs GERD: P = .004. Control vs OSA+GERD: P = .002. OSA vs GERD: P = .022. OSA vs GERD+OSA: P = .010. GERD vs GERD+OSA: P = .780.
Multivariable Analysis
Table 4 presents the results of the univariable and multivariable analyses. Among age, sex, BMI, OSA, GERD, smoking, drinking, and rhinomanometry, only GERD was independently associated with abnormal ETS-7 results (odds ratio = 3.090, 95% CI: 1.332-7.169, P = .009).
Univariable and Multivariable Analyses of Factors Associated With ETD.
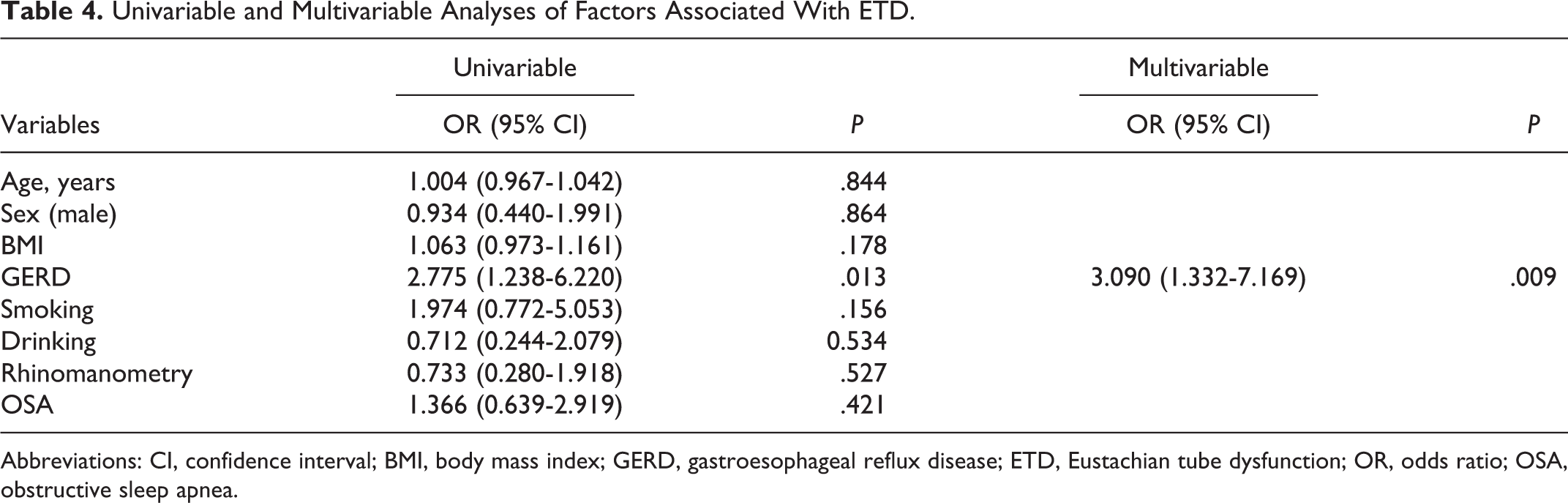
Abbreviations: CI, confidence interval; BMI, body mass index; GERD, gastroesophageal reflux disease; ETD, Eustachian tube dysfunction; OR, odds ratio; OSA, obstructive sleep apnea.
Discussion
This study aimed to explore the effect of GERD on Eustachian tube function in patients with OSA. The results suggest an association between GERD and ETD. The abnormal function of the Eustachian tube in OSA without GERD was not significantly higher than that of the controls as well as between the OSA+ GERD and GERD-only groups, based on ETDQ or ETS-7. Gastroesophageal reflux disease concomitant may be an important factor of ETD in patients with OSA.
Since the Eustachian tubes open in the nasopharynx, it is highly possible that GERD and OSA affect them. Indeed, Kim 5 showed that GERD is associated with ETD. Studies using subjective questionnaires associated symptoms of GERD with the symptoms of ETD. 13 The present study shows that the frequency of ETD was higher in the GERD-only group than that of the controls, which is consistent with the previous studies. Refluxing stomach content can directly block the Eustachian tubes or cause tube inflammation and adhesion and lead to an increased risk of otitis media. 14 Antireflux therapy can relieve refractory pressure feeling in the ears. 14 These are all possible reasons for the association between GERD and ETD.
The association between GERD and OSA is well-known, 3 although some conflicting results have been reported. 15 Including a meta-analysis, many studies7,16 showed that patients with OSA have a higher incidence of GERD, from 38.9% to 78.9%. Gastroesophageal reflux disease is known to induce throat symptoms such as cough, hoarseness, and apnea, and could, therefore, participate in the development of OSA. 3 On the other hand, OSA is known to induce changes in circulatory and airway dynamics. Mechanisms by which the 2 diseases are associated include large negative intrathoracic pressure swings generated during obstructive apneas and respiratory-related arousals that appear to be associated with lower esophageal sphincter relaxation and laryngeal sensory dysfunction. 17 Shepherd and Orr 18 suggested that obesity was, in fact, the common cause of GERD and OSA. Notwithstanding whether one can participate in the development of the other, or if they simply share common risk factors 18 is a matter of a little more debate, the occurrence of GERD in OSA is becoming more and more accepted.
Regarding OSA and ETD, Magliulo et al 6 showed that OSA was associated with ETD. Studies suggested that any factor impairing adequate air circulation in the nasal cavity and nasopharynx can cause symptoms of ETD. 19 Since OSA is associated with chronic sinusitis, poor nasal mucociliary clearance, and nasopharyngeal secretion stagnation, that is, conditions associated with nasopharyngeal obstruction and inflammation, 20 OSA could lead to ETD. As for GERD-induced inflammation, OSA-induced airway inflammation can cause ETD. 19 Nevertheless, these studies did not take into account the higher incidence of GERD in patients with OSA, as described earlier, and GERD alone might be an important causative factor for ETD. Hence, the present study observed patients with OSA with and without GERD. The results showed that the frequency of ETD in patients with OSA and GERD was higher than in the control group (ETS-7: 51.3% vs 15.6%; ETDQ: 43.2% vs 9.4%), but the frequency of ETD in patients with OSA but without GERD was not higher than that of the control group (ETS-7: 24.2% vs 15.6%; ETDQ: 15.2% vs 9.4%). The frequency of ETD in the GERD group was also higher than in the control group but not higher than the OSA-only group, and there was no difference between the OSA-only and control groups. Those results suggest that the occurrence of ETD has a more obvious relationship with GERD than with OSA. In addition, the multivariable analysis showed that only GERD was associated with the ETS-7 score. These results are indeed supported by the obstructive and inflammatory hypothesis of GERD on the Eustachian tubes. 14 These results could be due to the fact the stomach content in GERD causes an actual chemical injury to the nasopharynx and Eustachian tubes, and this injury could be more important than that caused by OSA, which is supported by Kim 5 and Magliulo et al. 6
Gastroesophageal reflux disease was associated with the ETS-7 and ETD-Q abnormal scores, and OSA had a higher incidence of GERD. The higher rate of ETD in patients with OSA may be a result of the high incidence of GERD in OSA. The results of the present study do not mean that OSA is not related to ETD. On the contrary, the proportions of patients with abnormal ETS-7 results were higher in the GERD and OSA+GERD groups compared to the control group but not higher than in the OSA only group, indicating that OSA is also a factor that cannot be ignored in ETD, but its influence might be indirect. Obstructive sleep apnea is not a silencing factor in ETD. We suggest that OSA is merely strengthening or indirectly participating in the occurrence of ETD and that OSA may not be an indirect factor for GERD. The patients were from a single center, and the sample size was relatively small. In addition, the cross-sectional design prevents any conclusion about causality.
A longitudinal study might be necessary to address this question properly. Additional studies are necessary. Besides GERD, patient characteristics, comorbidities, ethnicity, and age should be included in future studies, but these studies will have to be adequately powered to take into account those factors all at once.
Conclusion
This study suggests that GERD is an important factor causing abnormal ETS-7 and ETD-Q scores in patients with OSA. The higher rate of ETD in patients with OSA may be the result of the high incidence of GERD in OSA. Obstructive sleep apnea is also a factor that cannot be ignored in ETD. Nevertheless, this study could not establish causality, and studies are still necessary to examine this point. Nevertheless, the clinical significance of this study is that for patients with OSA, paying attention to their GERD symptoms and their Eustachian tube function and corresponding ear symptoms is of clinical importance, especially for those with GERD.
Methodological Considerations/Limitations
A longitudinal study might be necessary to address this question properly. Besides GERD, patient characteristics, comorbidities, ethnicity, and age should be included in future studies.
Footnotes
Authors’ Note
Informed consent was obtained from all individual participants included in the study. The study was approved by the ethics committee of Peking Anzhen Hospital (2019050X). The study was carried out in accordance with the principles of the Declaration of Helsinki.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Beijing Municipal Administration of Hospitals Ascent Plan [DFL20150602].