
Abstract
Objectives:
The objective of this pilot study was to report the feasibility and safety of a new 3-port supraclavicular approach in endoscopic submandibular sialoadenectomy.
Methods:
We reported the safety, surgical feasibility, and aesthetic features of the total endoscopic submandibular sialoadenectomy (submandibular gland excision) using a 3-port supraclavicular approach in our institute from December 2018 to January 2020.
Results:
Endoscopic submandibular sialoadenectomy using a 3-port supraclavicular approach was performed in 2 patients with intraglandular sialolithiasis. No major adverse events occurred in this study. The patient’s satisfaction score was high (more than 8; range: 0-10).
Conclusions:
The 3-port supraclavicular approach submandibular sialoadenectomy is a feasible method that permits a relatively good surgical scarring and minimal adverse effects.
Keywords
Introduction
Submandibular sialoadenectomy or submandibular gland excision is the procedure to remove the submandibular gland. This procedure can be done either by an open or endoscopic approach. Currently, the endoscopic approach has gained in popularity due to a smaller incision scar that is less noticeable.
There were 2 endoscopic submandibular sialoadenectomy techniques, including endoscopic-assisted and total endoscopic method. The endoscopic-assisted method included the lateral transcervical, submental, and transoral endoscopy-assisted approaches. 1
The total endoscopic method included the transoral robot-assisted approach 2 and chest wall approach. 3 To our knowledge, this is the first report on a total endoscopic supraclavicular approach.
The objective of this pilot study was to report the experience of using a 3-port supraclavicular approach for total endoscopic submandibular sialoadenectomy in intraglandular sialolithiasis patients.
Patients and Methods
Patients presenting with intraglandular submandibular sialolithiasis that were failed to remove through endoscopic sialoendoscopy from December 2018 to January 2020 at the Srinagarind Hospital, Khon Kaen University were included in this study.
The patients were allowed to choose whether they would undergo traditional transcervical or endoscopic submandibular sialoadenectomy using the supraclavicular approach after a discussion on the risks and benefits of each technique.
Technical Description
Patient selection
The eligibility criterion was intraglandular submandibular sialolithiasis that were failed to remove through sialoendoscopy. We excluded patients who had previously undergone neck surgery, had a history of cervical injury, with bleeding tendencies, and in whom malignancy was suspected.
There were 10 patients who matched our inclusion criteria during this period. Two patients agreed to participate in this study.
Patient position and operating room setting
The patient was placed in a supine position with the neck extended and rotated to the contralateral side to expose the operative field. The arms of the patient were adducted and placed by the sides of the body on the operating table. The patient was administered general anesthesia using oral intubation. The surgeon stood by the pathology side of the patient. The camera operator stood by the contralateral side of the patient. The scrub nurse was positioned around the head of the patient (Figure 1).

Overview of the operating room setting.
Operative technique
An incision was made at the ipsilateral supraclavicular area, around 2 fingerbreadths above the clavicle to avoid an injury to lungs and major vessels. The incision can be tailored to suit the patient’s needs. The incision that closer to the clavicle is easier to hide under the cloth. However, as the distance from incision to the target submandibular gland increased, the area of dissection was larger and there was a higher chance of accidentally enter into the mediastinum.
A 10-mm central incision and bilateral 5-mm incisions were made for the endoscope port and instrument port, respectively. The central incision should be situated at a midclavicular point, whereas the bilateral incisions should be approximately situated at the sternal end and acromial end of the clavicle. If the bilateral incisions are too close to the central incision, it will limit the dissection field and angle of maneuver (Figure 2). Furthermore, the incisions should be adjusted to avoid the external jugular vein to prevent bleeding-related complications and delay operating time.
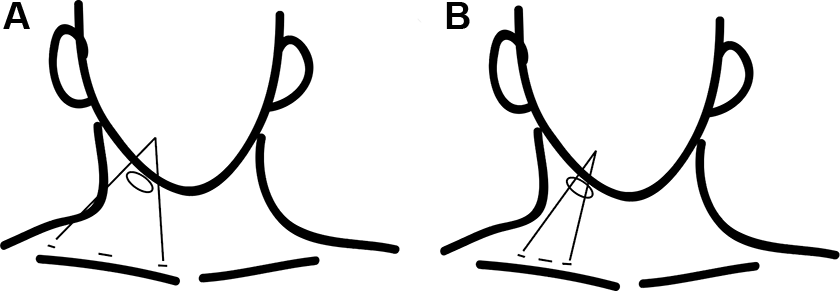
Supraclavicular incisions (A) preferable 3 incisions, (B) the incisions are too close to each other.
The acromial end incision can be adjusted to be higher than 2 fingerbreadths above the clavicle to decrease the dissection area. This incision was less noticeable in the anteroposterior view (Figure 3).

Position of the patient and placement of trocars.
The hydrodissection was performed using a Veress needle by infiltrating the subplatysmal space with a diluted epinephrine solution (0.1 mL of epinephrine [1:1000] in 200 mL of normal saline) in a fan-shaped manner.
The working space was created by blunt dissection of the subplatysmal space using Kelly clamps, and a dilator until the submandibular space was reached. A 10-mm and two 5-mm short trocars were inserted with CO2 insufflation. A 30° endoscope was used to visualize the operating space. The remaining fibrous bands in the subplatysmal space were incised, and the lower part of submandibular gland was identified.
The fascia of the submandibular space from an inferior to superior direction that carries the marginal mandibular nerve was elevated superiorly away from the gland. The facial vein was ligated using 5-mm ultrasonic shears (Harmonic Scalpel; Ethicon Endo-Surgery; Cincinnati, OH) and elevated away from the gland. Then, superior and lateral side of the submandibular gland was dissected.
The facial artery may be found at the posterior part of the submandibular gland and can be ligated using ultrasonic shears. Then, the submandibular gland can be retracted anterolaterally to identify the lingual nerve and Wharton duct (WD).
The lingual nerve was separated away superiorly, and the duct was ligated using 5-mm ultrasonic shears. After the duct was ligated, the submandibular gland was mobile and able to be transferred out through the central incision. Meticulous hemostasis was attained. No drain was left in place, and the skin was sutured cosmetically (Figure 4).
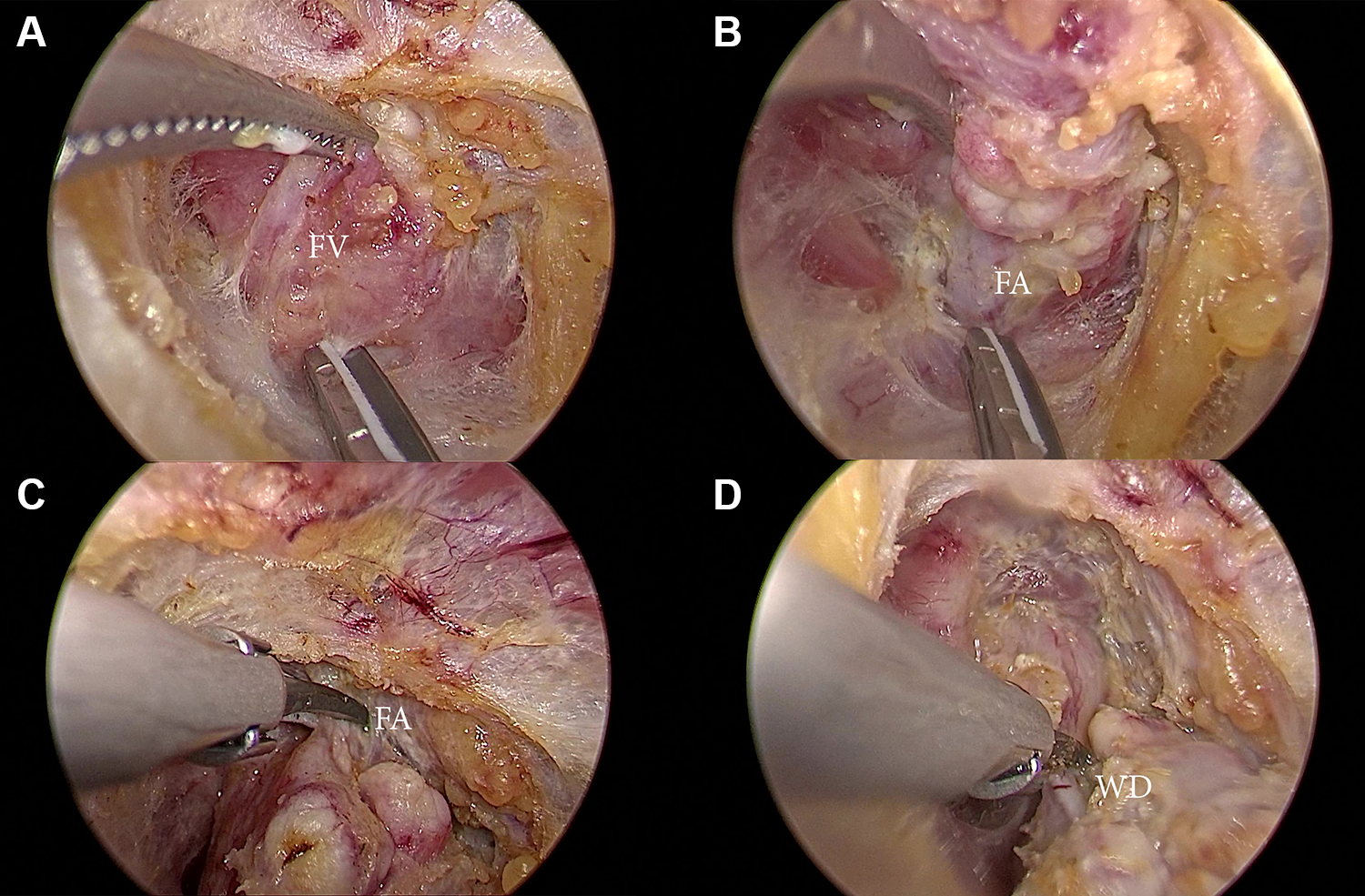
Endoscopic view during the dissection. A, The facial vein (FV) was ligated and elevated, (B) the facial artery (FA) was ligated below the gland, (C) the FA was ligated above the gland, (D) the Wharton duct (WD) was ligated before the gland was removed.
Outcomes
The patient demographics, size of the submandibular stone, conversion to open surgery, blood loss, operation time, injury to the nerves, paresthesia, and patient satisfaction data were collected.
Ethical Considerations
This study was approved by the Khon Kaen University Ethics Committee in Human Research (HE621542). Written informed consent to participate in this study was provided by all patients enrolled. All authors abided by the Declaration of Helsinki.
Results
Two patients elected to undergo supraclavicular approach endoscopic submandibular sialoadenectomy, all of whom were diagnosed with intraglandular sialolithiasis who failed to remove through sialoendoscopy. The data of the patients are shown in Table 1. The operative time ranged from 90 to 120 minutes. The estimated volume of intraoperative blood loss ranged from 5 to 20 mL.
Individual Patients’ Data.

No patients underwent conversion to open submandibular sialoadenectomy, and none experienced marginal mandibular nerve injury, lingual nerve injury, hypoglossal nerve injury, or hematoma. One patient experienced paresthesia at the left neck that was resolved in 3 months. The average length of stay was 3 days. After 1 month, the scar was hidden in the supraclavicular creases in the supraclavicular creases and was barely noticeable. The patient’s satisfaction score was high (more than 8; range: 0-10; Figure 5).

Surgical scar at 1 month after endoscopic submandibular sialoadenectomy using a 3-port supraclavicular approach.
Discussion
The open submandibular sialoadenectomy can be performed using various incision such as lateral transcervical, retroauricular, and submental incision. However, the lateral transcervical incision was an incision of choice for most surgeons. 1
The video-assisted and total endoscopic approaches were developed after the success in endoscopic head and neck surgery such as thyroidectomy and parathyroidectomy.4-7 The objective of these approaches was to hide or decrease the neck scar that was easily noticeable.
In 2002, the feasibility of a total endoscopic sialoadenectomy was examined in a porcine model. Twelve endoscopic submandibular gland resections were performed on 7 Yorkshire adult pigs using a combination of balloon dissection and low-pressure CO2 insufflation. Three incisions were made. The central 14-mm incision accepts the 12-mm trocar which houses the endoscope, while the 2 lateral incisions (6-7 mm) were used to place the 5-mm operative trocars. All 12 submandibular gland resections were successfully performed endoscopically, and no conversions to open resection were necessary. 8
Terris et al study the feasibility of endo-robotic submandibular gland sialoadenectomy in a cadaver model in 2005. 9 Eleven endo-robotic submandibular gland resections were successfully performed in 6 cadavers. No conversions to open resection were necessary.
Since the success in the cadaver model, the endoscopic technique in the head and neck region has been refined. In 2018, endoscopic submandibular sialoadenectomy through a chest wall approach without the creation of any neck incisions was reported in human. Four patients with benign submandibular gland lesions underwent a total endoscopic submandibular sialoadenectomy through a chest wall approach using 3 ports (one 10-mm port for the camera and two 5-mm ports for the working instruments). Conversion to the open technique was only necessary in one case. 3 In 2019, a transoral robotic submandibular sialoadenectomy with preservation of sublingual gland and WD was successfully performed in 32-year-old female. 2
We successfully performed the total endoscopic submandibular sialoadenectomy using a 3-port supraclavicular approach in 2 patients. There were no major adverse events, such as hematoma or major major nerve injury in this study. One patient in this study had the paresthesia at the surgical area (left neck) that was resolved in 3 months.
The operating room setting could be adjusted according to surgeon’s preference. Alternatively, the camera operator can stand on the same side of the surgeon instead of standing on the contralateral side. The monitor can be moved to the opposite side of the lesion, and the ventilator can be in the usual position at the head of the operative bed.
In these 2 cases, we decided to make the acromial end incision a little higher than 2 fingerbreadths above the clavicle to decrease the dissection area. Because this is a new approach, we expected that it might take more time to dissect than the conventional case. Although this incision was less noticeable in the anteroposterior view, the surgeon needed to talk to the patient whether this incision is acceptable by the patient.
The 3-port supraclavicular approach resection steps resembling the conventional open transcervical submandibular resection. Therefore, the learning curve to perform the 3-port supraclavicular approach for most surgeons should be steeper than the transoral approach. Furthermore, a 3-port supraclavicular approach has a smaller resection area compare to chest wall approach leading to faster recovery time.
This approach is not a scarless technique. Three small scars at the supraclavicular area are acceptable in our patients. In our opinion, the 3 small scars can blend better with a natural neck crease compared to the conventional submandibular incision. However, some patients may prefer scarless or no neck scar. In this instance, the transoral or chest wall approach would be a better option.
Conclusions
We reported the feasibility and safety of the total endoscopic submandibular sialoadenectomy using a 3-port supraclavicular approach. The surgical scar was minor and hidden in the supraclavicular creases.
Footnotes
Acknowledgments
The authors would like to thank all of the patients who participated in this study.
Authors’ Note
This study was approved by the Khon Kaen University Ethics Committee in Human Research (HE621542). Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.