
Abstract
Spontaneous cerebrospinal fluid (CSF) leak is a condition that commonly presents with unilateral watery drainage from the nose or ear, tinnitus, and stuffy ears or hearing loss. Spontaneous CSF rhinorrhea and otorrhea together are rare. A 64-year-old woman presented at our department with complaints of clear watery rhinorrhea and hearing loss on the right side persisting for 10 months. Imaging and surgery were used to diagnose the condition. Through surgical treatment, she was eventually cured. Review of the literature has shown that patients with both nasal and aural CSF leaks are rare. When a patient presents with both unilateral watery drainage from both the nose and ear, a diagnosis of CSF rhinorrhea and otorrhea should be considered. This case report will benefit clinicians by providing more information to assist with diagnosing the disease.
Introduction
Cerebrospinal fluid (CSF) leak results from direct communication between the CSF-containing subarachnoid space and the nasal cavity, nasal sinuses, or middle ear cavity. It is caused by bony defects, ruptures, or weaknesses of the dura mater or the bone of the lateral skull base.1–3 A CSF leak may be classified as secondary or spontaneous. Secondary CSF leaks are mainly caused by inflammation, trauma, tumors, surgery, etc. 1 However, the etiology of spontaneous CSF leaks is not clear. A spontaneous CSF leak might occur due to defects in the anterior, middle, or posterior cranial fossa bony plate, or when the overlying dura becomes fragile and breaks.3,4 Depending on whether the CSF flows into the middle ear cavity or the nasal cavity, a spontaneous CSF leak can be classified into spontaneous CSF otorrhea or rhinorrhea, which have different clinical presentations. The clinical presentations of spontaneous CSF otorrhea might be similar to serous otitis, with conductive hearing loss. 5 Clear, pulsatile otorrhea is often evident after myringotomy and grommet placement.4,6,7 The clinical manifestations of CSF rhinorrhea might be similar to allergic rhinitis, with continuous watery nasal discharge. 8 Both can present with tinnitus and headache. 9 Compared with secondary CSF, diagnosis of spontaneous CSF leakage is more difficult due to its atypical symptoms.
Simultaneous spontaneous CSF rhinorrhea and otorrhea are rare. In 2012, Schraven et al. 10 reported a case of spontaneous CSF leak from the nasal cavity and middle ear in a pregnant woman. We describe a case of a woman whom we diagnosed with spontaneous CSF rhinorrhea and otorrhea after reviewing her imaging and medical history. More attention should be paid to the role of medical history and imaging in the diagnosis of this disease. The different management options are reviewed.
Case report
A 65-year-old woman presented to our ENT clinic with a 10-month history of clear watery nasal drainage and hearing loss on the right side. No nasal obstruction, otorrhea, tinnitus, or psychological disturbance was described. She had a background of hypertension. There was no history of trauma, surgical operations, or tumor. Nasal endoscopy showed clear fluid discharge from the right middle meatus (Figure 1a). Coronal computed tomography (CT) revealed a defect in the right cribriform plate (Figure 1b). Axial CT showed tympanic effusion on the right side (Figure 1c). Sagittal magnetic resonance imaging (MRI) showed the presence of an empty sella (Figure 1d). The nasal secretions were proven to be CSF upon laboratory testing (with a glucose concentration of 4.79 mmol/L, and a chlorine concentration of 134.50 mmol/L). (a) Endoscopy showed clear fluid discharge in the right middle meatus. (b) Coronal CT revealed a defect in the right cribriform plate. (c) Axial CT showed tympanic effusion in the right side (arrows) as well as bony pneumatization in the mastoid region. (d) Sagittal MRI showed an empty sella.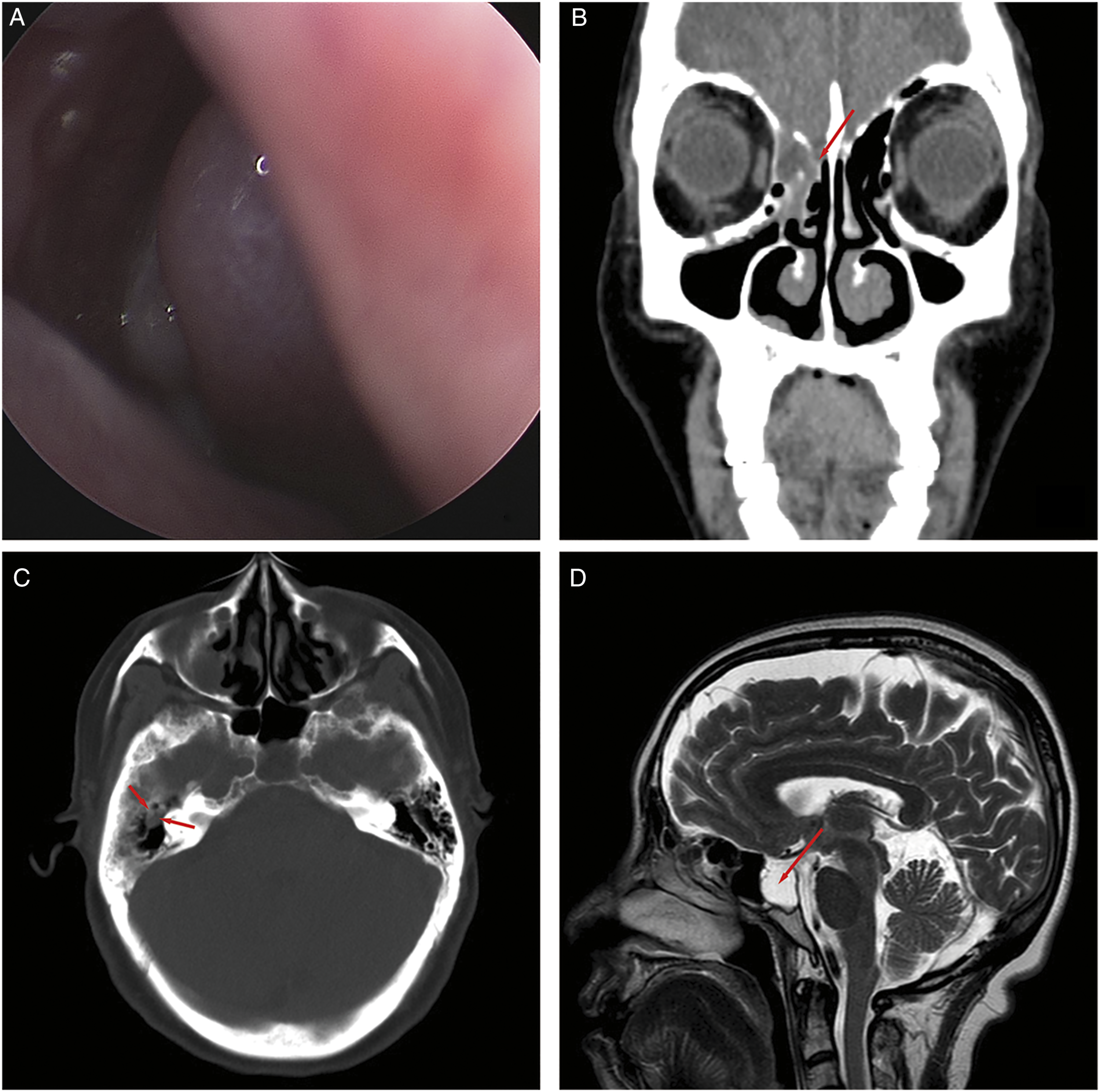
The patient was diagnosed with spontaneous CSF rhinorrhea and otitis media. She underwent a transnasal endoscopic sandwich procedure to treat her CSF rhinorrhea. Her postoperative response was highly favorable. She was discharged on postoperative day 5 in satisfactory condition, and no signs of recurrence were observed for 12 months postoperatively.
She was hospitalized again for hypertension one year later. During her hospitalization, she had a repeating sinus CT and MRI for her CSF rhinorrhea. Axial CT showed no CSF rhinorrhea, but there was a significant defect in the right tegmen tympani, and increased tympanic effusion (Figure 2a) compared with the previous CT scan of the temporal bone. In addition, her MRI revealed a water signal in the right mastoid (Figure 2b). (a) Axial CT showed a defect in the right tegmen tympani (arrow) and increased tympanic effusion. (b) Axial MRI revealed a water signal in the right mastoid (arrow).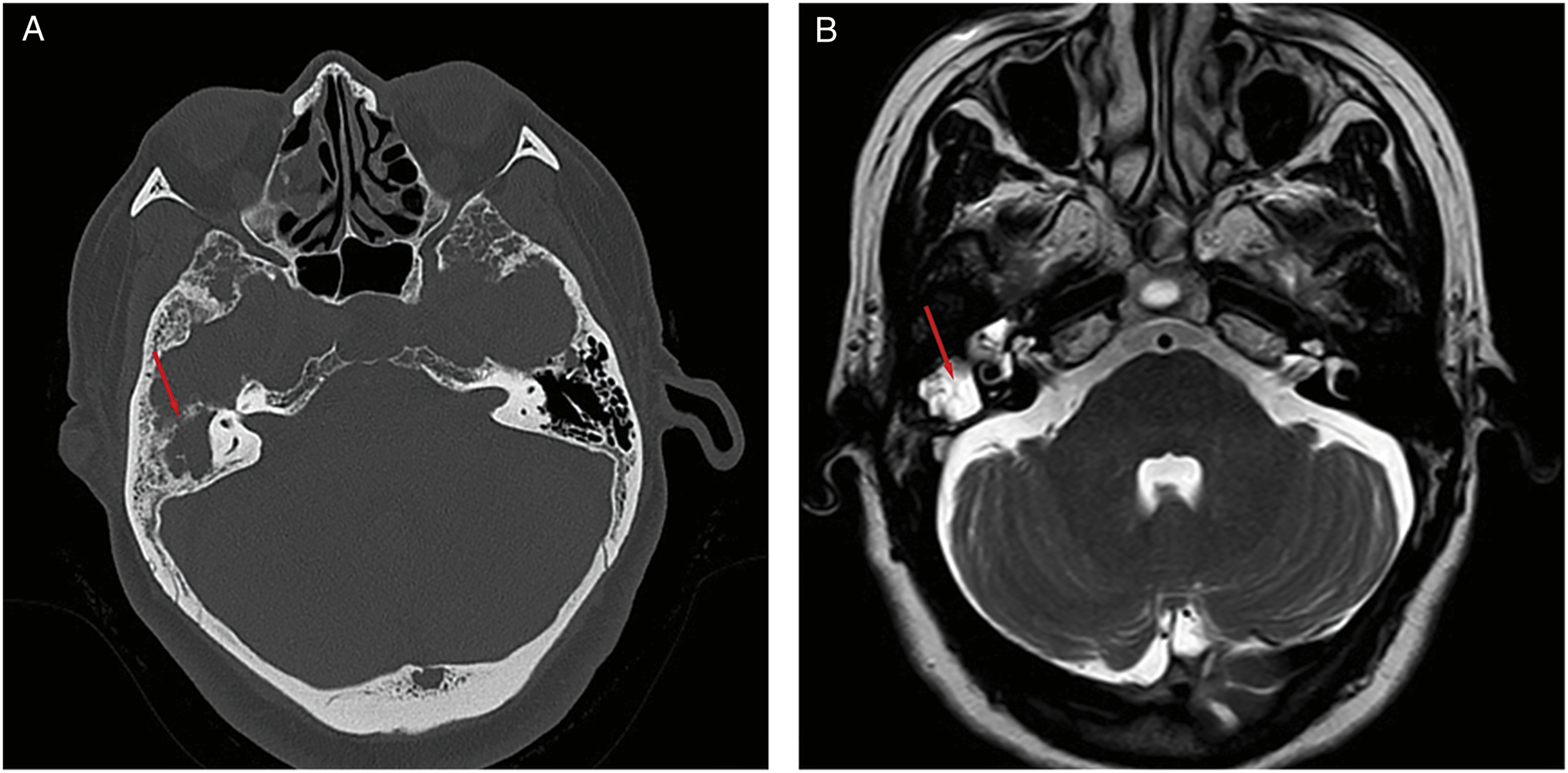
After the patient was discharged from the hospital, the cardiologist advised her to visit the ENT clinic. She presented to the ENT department with her CT and MRI findings. She stated that there was no significant change in her hearing, and she only occasionally felt stuffiness in her right ear. There was no new history of trauma, surgical operations, or tumor during the previous year. Initial examination revealed effusion in the right-side tympanic cavity. Pure tone audiometry showed mild conductive hearing loss with 12 dB air-bone gap in her right ear (Figure 3a), and a tympanogram revealed a type B pattern on the right side (Figure 3d). (a) Pre-operative pure tone audiometry showed mild conductive hearing loss with air-bone gap 12 dB in the right ear. (b) The first post-operative pure tone audiometry showed mild conductive hearing loss with air-bone gap 16 dB in the right ear. (c) The second post-operative pure tone audiometry showed no conductive hearing loss in the right ear. (d) A pre-operative tympanogram revealed a type B pattern on the right side. (e) The first post-operative tympanogram revealed a type B pattern on the right side. (f) The second post-operative tympanogram revealed a type A pattern on the right side.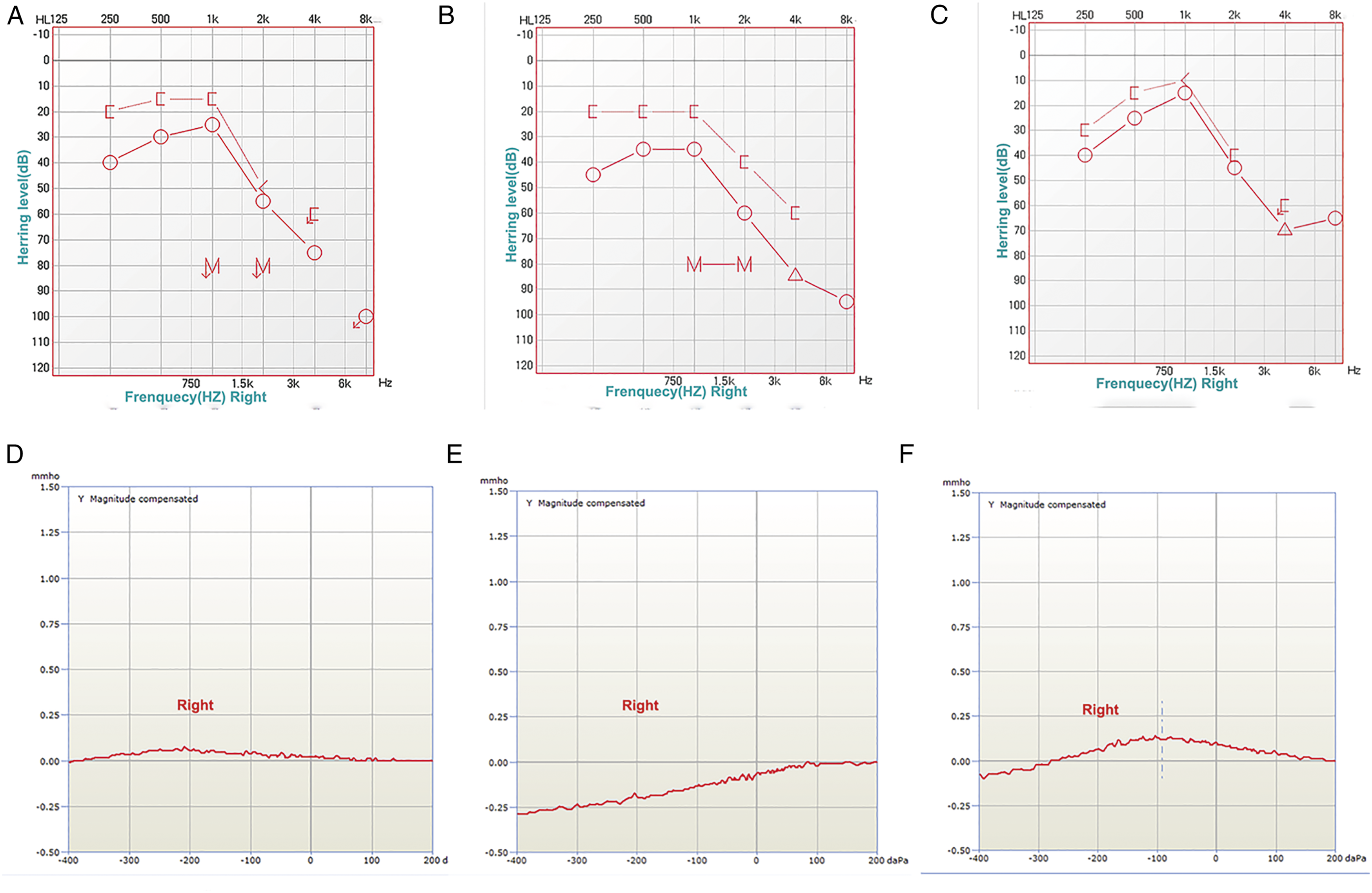
She was diagnosed with right-side secretory otitis media (SOM) and underwent myringotomy with grommet insertion in her right ear. Clear fluid was noted in the tube.
At the one-month follow-up after surgery, the hearing loss in her right ear was more severe than it was before surgery, and there was a continuous discharge of clear fluid through the right ear tube. A new symptom of pulsatile tinnitus had also appeared in the right ear. However, she had no vertigo, headache, or fever. Further pure tone audiometry showed mild conductive hearing loss with 16 dB air-bone gap in her right ear (Figure 3b), and a tympanogram still revealed a type B pattern on the right side (Figure 3e). Reviewing MRI still showed water signal in the right mastoid.
A review of her imaging and symptoms raised the suspicion of an ongoing CSF leak. She underwent a canal wall-up mastoidectomy. During the operation, a CSF leak in the tegmen tympani was found and repaired. The patient was discharged on postoperative day 5.
At one month postoperatively, pure tone audiometry showed no conductive hearing loss in the right ear (Figure 3c), and a tympanogram revealed a type A pattern on the right side (Figure 3e). She had not experienced CSF leak for the past 8 months following surgery.
Discussion
Spontaneous CSF leak represents a clinical condition in which CSF rhinorrhea or otorrhea occurs without any history of trauma, tumor, or surgery.11–13 The diagnosis of spontaneous CSF leak is difficult because its pathogenesis is unclear and its clinical symptoms are atypical. Although the mechanism of symptom production remains controversial, several causes of this condition have been identified. Spontaneous CSF leaks may be related to factors such as obesity, sex, or idiopathic intracranial hypertension (IIH).2,14,15 Symptoms of spontaneous CSF leak may be intermittent and asymptomatic, during which patients may complain of clear fluid leaking from their nose or ear, or present with headaches, hearing loss, and a sense of ear fullness and/or pulsatile tinnitus.10,12,15,16
Here, we report a rare case of ipsilateral spontaneous CSF rhinorrhea and otorrhea, presenting in an elderly woman, with no obvious cause for her symptoms. Previous reports of CSF leaks in the ear and nose have been documented in the literature, one published case was retrieved regarding simultaneous CSF rhinorrhea and otorrhea, in which the patient was pregnant. Schraven reported that a pregnant woman with CSF rhinorrhea and otorrhea presented typical with nasal and aural symptoms, her nasal and middle ear secretions proved to be CSF, and MRI findings suggested an empty sella. 10 Excessive vaporization of the skull and empty sella are common clinical manifestations of spontaneous CSF leaks and IIH. 17
The patient reported in this paper was an elderly woman who also showed an empty sella in her MRI (Figure 1d), as well as the presence of bony pneumatization in the mastoid region (Figure 1c). We identified the nasal discharge as CSF by glucose testing, and when combined with the patient's imaging and history, we diagnosed her with spontaneous CSF rhinorrhea. We performed endoscopic CSF rhinorrhea repair and found no further symptoms of CSF rhinorrhea at her 2-year postoperative follow-up.
The diagnosis of spontaneous CSF otorrhea is more challenging than that of spontaneous CSF rhinorrhea, and the patient experienced atypical symptoms in the affected ear. The patient's first visit was due to typical symptoms of CSF rhinorrhea, and her symptoms of mild hearing loss were overlooked. We also ignored the middle ear effusion and possible tegmen tympani defect mentioned in the patient's first CT. When she had her routine check for CSF rhinorrhea repair a year later, the examination revealed fluid in the right middle ear, and we diagnosed her with SOM and performed myringotomy and ventilation tube insertion. Her symptoms, however, worsened rather than lessened. It has been reported in the literature that a patient who had SOM for 3 years was eventually diagnosed with CSF otorrhea in combination with imaging findings. 16 Thus, it is not uncommon in clinical practice for CSF otorrhea to be misdiagnosed as SOM. When patients have tegmen tympani defects and mastoid effusion, but no history of trauma of the ear or skull, the diagnosis of spontaneous CSF otorrhea should be taken into consideration with the aid of MRI. 18 Evidently, imaging is highly beneficial in detecting CSF otorrhea because both middle ear effusion and bone defects can be identified.
In addition to imaging, the diagnosis can be strengthened by the detection of β2-transferrin in secretions from nasal or tympanic cavities.19,20 According to report, the specificity of β2-transferrin detection in diagnosing CSF leaks ranges from 71% to 94%, and the sensitivity ranges from 87% to 100%, which is the gold standard for the diagnosis of CSF leaks. 20 While the β2-transferrin test is more accurate for CSF leaks, it is expensive and time-consuming. 21 The traditional glucose test is relatively faster and more convenient. The glucose test is also useful for ruling out patients with meningitis and diabetes. 22 Our patient had no history of diabetes and no manifestations of meningitis, so we opted for a glucose test for a quicker diagnosis. Combined with the patient's chloride concentration test result of >110 mmol/L (she had a chlorine concentration of 134.50 mmol/L), this strengthened the diagnostic evidence for CSF leakage. 23
Quiney et al. 24 believed that a defect of the tegmen tympani was a congenital defect caused by abnormal embryonic development. Long-term high intracranial pressure caused damage to the dura mater and resulted in CSF otorrhea. Gacek et al. 25 believed that a defect at the tegmen tympani was due to the abnormal retention of arachnoid granules in the local skull, where the bone was weak, and the pressure of the CSF acted directly on the weak part, resulting in CSF otorrhea. However, it is also possible that the patient did not have CSF otorrhea at that time, but only had mastoid inflammation of the middle ear. After surgical repair of CSF rhinorrhea, the intracranial pressure increased, and the consequent long-term raised pressure of the CSF eroded the weak bone of the temporal bone, causing dura mater rupture, and resulting in the occurrence of CSF otorrhea.
CSF otorrhea can occur in both children and adults, however, the clinical manifestations of spontaneous CSF otorrhea differ between the two. Children with spontaneous CSF otorrhea often have inner ear deformities or unexplained repeated episodes of meningitis, making spontaneous CSF otorrhea relatively easy to identify. 26 Adults with spontaneous CSF otorrhea may present with secretory otitis media, watery discharge from the ear, persistent headache, hearing loss, and infrequent meningitis symptoms. In this case, based on her ear symptoms, medical history, and imaging data, we initially considered the diagnosis of SOM and performed myringotomy and ventilation tube insertion on our patient's second visit, At the one-month postoperative follow-up, a clear, watery discharge from the ventilation tube was seen in the patient's right external ear canal. After reviewing her medical history, CT, and MRI images again, we promptly confirmed the diagnosis of CSF otorrhea and finally performed a successful repair operation. When the diagnosis of CSF otorrhea is clear, we should follow-up closely after providing health education about intracranial infection. Because of atypical symptoms of spontaneous CSF otorrhea in adults, careful analysis of the patient’s clinical presentation is needed to clarify the diagnosis as early as possible.27,28
In summary, this case highlights the fact that spontaneous CSF rhinorrhea and otorrhea can develop simultaneously. If a patient with CSF rhinorrhea presents with conductive or mixed hearing loss, imaging evaluation including CT and MRI should be investigated for diagnosis and surgical planning.
Footnotes
Authors’ Contribution
LSJ proposed the idea and performed the literature search, LSJ and LT analyzed the case and wrote the paper. WY, GM, and MYR provided support and participated patient information collection. LSL and RB revised the manuscript. All authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the funding from 2022 Yunnan Science and Technology Department - Kunming Medical University Joint Fund for Applied and Basic Research (No. 202201AY070001-078), Doctoral Scientific Research Fund of the First Affiliated Hospital of Kunming Medical University (No. 2019BS004).
Informed consent
A legally authorized representative of the patient gave written consent for the publication of this case report.