
Abstract
Pneumocephalus refers to air inside the cranium; however, otogenic pneumocephalus is rarely reported in the literature. The neurological presentations of pneumocephalus include headache, lethargy, confusion, disorientation, and seizure. Here, we have reported a case of a 42-year-old woman with extensive pneumocephalus and cerebrospinal fluid leak secondary to petrous bone cholesteatoma. She presented to the emergency department with sudden headache and left ear discharge. Physical examination revealed watery otorrhea through a hole in the tympanic membrane. Radiological studies demonstrated extensive soft tissue in the left middle ear and mastoid extending to the internal auditory canal. Free intracranial air was observed, and bony destruction was seen in the cochlea, vestibule, and semicircular canals. The patient was managed surgically via the transotic approach and fully recovered. Although otogenic pneumocephalus is rarely encountered in clinical practice, early diagnosis and urgent management are important to prevent fatal complications.
Introduction
Petrous bone cholesteatoma (PBC) is a rare pathological entity that comprises 4%‐9% of all petrous pyramid lesions. 1 PBC gradually involves the petrous apex, otic capsule, and skull base. It may also invade the internal auditory canal (IAC) and vital neurovascular components in the temporal bone and intracranial structures, resulting in serious complications. 1,2
Intracranial complications related to PBC occur in 2%‐6% cases. Among the complications, pneumocephalus is extremely rare and associated with significant mortality. 1 Pneumocephalus is defined as air inside the cranium and classified into benign and tension variants. 3 The causes of otogenic pneumocephalus include trauma, middle ear infection, surgical intervention, neoplastic processes, congenital defects, and idiopathic causes. 4
Here, we have presented an unusual case of extensive pneumocephalus and cerebrospinal fluid (CSF) leak secondary to PBC.
Case Report
A 42-year-old woman presented to the emergency department complaining of sudden headache, nausea, and vomiting that had lasted 1 day. In addition, she had left ear watery discharge, deafness, ear fullness, and dizziness. The ear discharge had started 1 week before, but the amount of discharge had significantly increased compared to that on the previous day. There were no other neurological symptoms. The patient had a history of tympanoplasty and mastoidectomy on the left ear 10 years ago, and she had experienced left facial paralysis for >3 years. Her vital signs were within the normal range. Physical examination revealed clear watery pulsatile discharge in the left external auditory canal draining from a 1-mm perforation of the tympanic membrane. Left facial palsy was categorized as grade 6 paralysis based on the House–Brackmann grading system.
Brain computed tomography (CT) showed extensive pneumocephalus in the basal cistern and cortical sulci (Figure 1A), while temporal bone CT demonstrated extensive soft tissue opacification in the left middle ear and mastoid, with erosion of the ossicles, scutum, and tegmen tympani. Moreover, bony destruction was noticed in the cochlea, vestibule, and semicircular canals (Figures 1B and 1C). There were no other lesions, such as parenchymal mass or abscess. Brain magnetic resonance imaging (MRI) revealed a high-signal intensity on T2- and diffusion-weighted imaging, a characteristic of cholesteatoma (Figures 1D and 1E). Preoperative photographs. Brain CT scan showing extensive pneumocephalus (A). Temporal bone CT images displaying a lesion filling the left middle ear and mastoid, with extension to the vestibule, cochlea, and IAC, with air in the inner ear and IAC (arrows; B, C). T2-weighted magnetic resonance imaging showing soft tissue opacification with a high-intensity signal in the middle ear and mastoid (D). Diffusion-weighted imaging showing a high-intensity area in the middle ear and mastoid, indicating cholesteatoma (arrow; E). IAC, internal auditory canal; CT, computed tomography.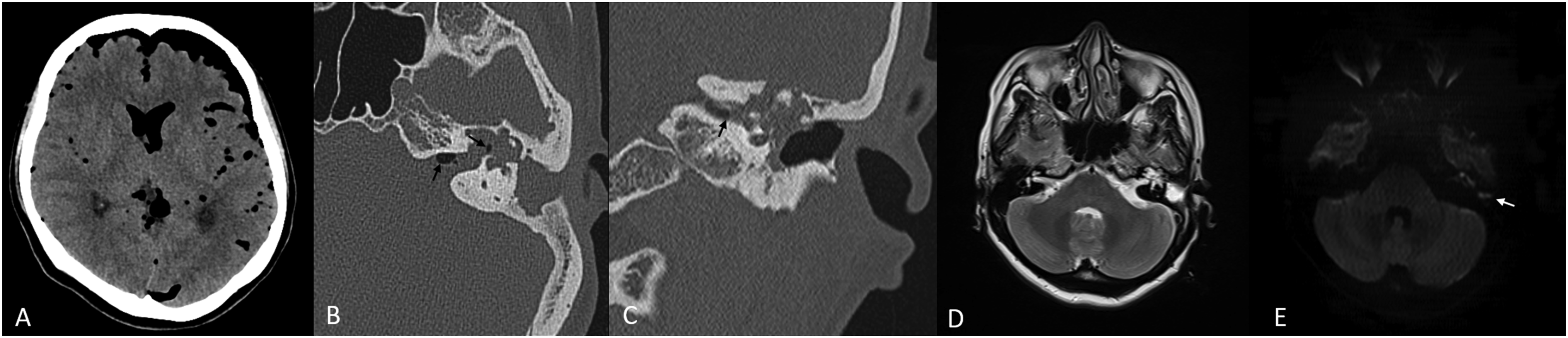
The patient was kept in a supine position with her head elevated at 30°. She was administered normobaric oxygen. Further, a lumbar drain was inserted, and an antibiotic (ceftriaxone) was administered. She underwent surgery via the transotic approach. The surgery showed that the cholesteatoma extended to the cochlea, vestibule, lateral and superior semicircular canals, as well as the IAC (Figures 2A-2C). A CSF leak was noted from the IAC. The labyrinthine segment of the facial nerve was missed. After complete removal of the cholesteatoma, the eustachian tube was closed using periosteum and bone wax. The IAC and mastoid cavity were closed using abdominal fat and fibrin sealant patch (TachoComb®). Three days after surgery, the lumbar drain was removed. Repeat brain and temporal bone CT 6 days after surgery revealed complete disappearance of the pneumocephalus (Figures 2D and 2E). Repeat MRI 3 months after surgery demonstrated no pneumocephalus or residual lesion (Figure 2F). Intraoperative microscopic views showing cholesteatoma in the internal auditory canal (arrow) and middle ear (arrowhead) (A-C). Postoperative photographs; brain CT scan showing complete disappearance of pneumocephalus (D). Temporal bone CT showing fully resolved pneumocephalus (E). T1-weighted magnetic resonance imaging showing a high-intensity signal for the fat used in obliteration (F). CT, computed tomography.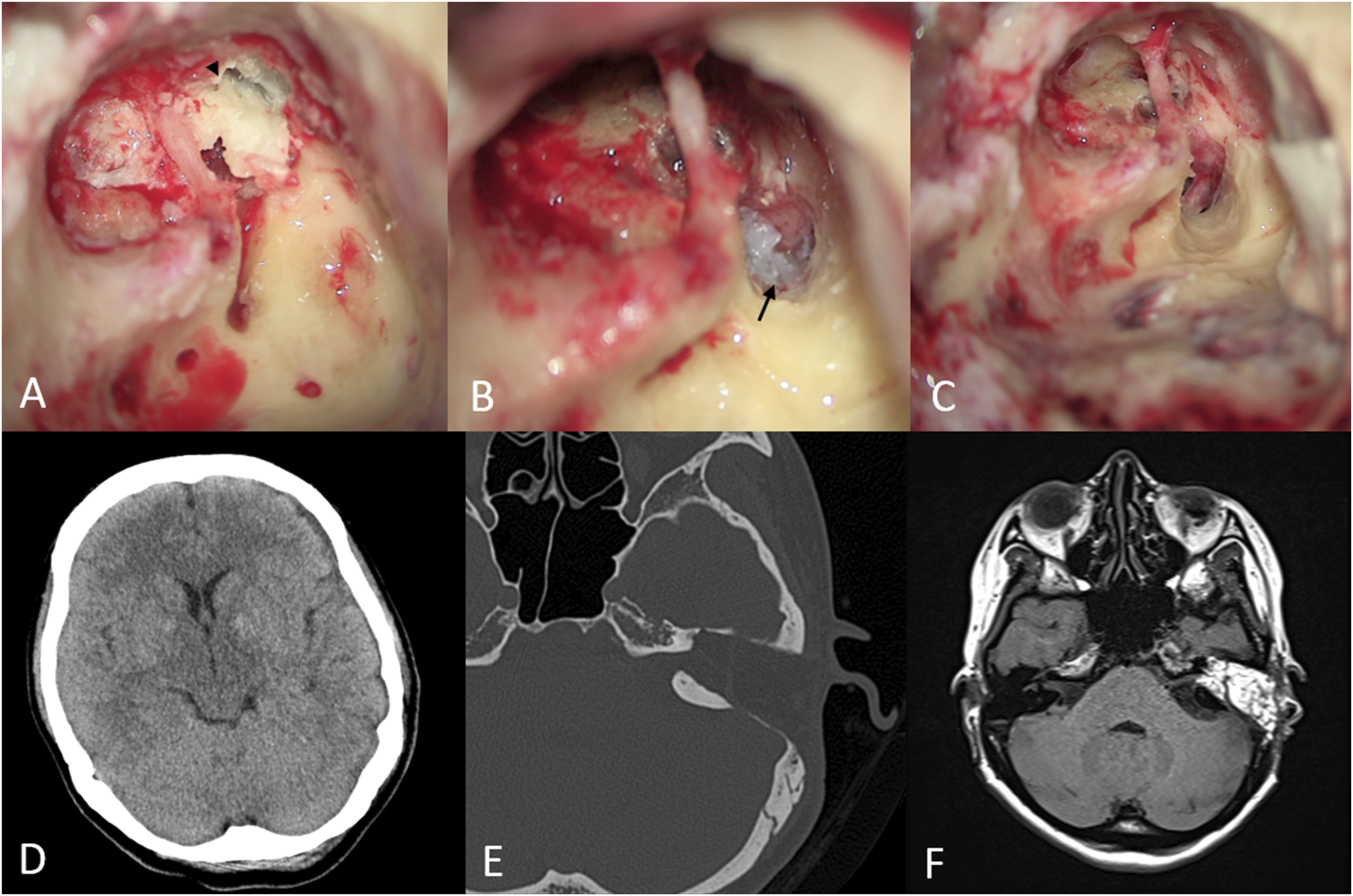
Discussion
The presentation of otogenic pneumocephalus is relatively variable. In benign pneumocephalus, patients can present with headache, lethargy, confusion, and disorientation, while in tension pneumocephalus, patients can present with nausea, vomiting, papilledema, seizures, and cardiac or respiratory arrest. 3,4 Patients with otogenic pneumocephalus present with ear symptoms, including otalgia, ear discharge, aural fullness, tinnitus, and hearing loss. 5
Although the most common symptoms are hearing loss, followed by facial palsy in patients with PBC, the most common symptom is headache in patients with pneumocephalus. 1 -3 In the present case, the patient presented sudden onset headache, CSF leak, deafness, and facial palsy. The site of the bony defect resulting in pneumocephalus was the IAC, which has not been reported thus far.
Pneumocephalus is caused by a bone defect in the cranium that allows air to move inside. 6 It can occur via 2 mechanisms. The first mechanism is the ball valve mechanism, in which air moves into the intracranial cavity through a defect secondary to nose blowing or straining. The air flow is unidirectional; therefore, air that enters cannot escape because of plugging by bone fragments, dural flap, mucosa, or granulation tissue. This form of pneumocephalus develops over a period of time. 7,8 The second mechanism is known as the inverted bottle effect. It is associated with CSF leak, which leads to negative intracranial pressure and causes air to enter the cranium to equalize the pressure. 9 In the present case, pneumocephalus developed via the inverted bottle effect; the patient had a history of CSF otorrhea for 1 week, which had forced air to move inside the cranial cavity to compensate the negative intracranial pressure.
Otogenic pneumocephalus should be suspected if a patient has CSF otorrhea, a history of ear surgery, or temporal bone trauma. 3 Radiological study plays a major role in the diagnosis of pneumocephalus, with high-resolution CT and MRI being the main modalities as they have good sensitivity and specificity. 10 CT is usually performed first; it can detect small amounts (.5 mL) of air inside the cranial cavity as well as the location and size of the bony defect. MRI helps to diagnose and localize the defect and identify herniated brain in the ear cavity. 11
There are multiple factors that affect the management of pneumocephalus, including type and etiology of pneumocephalus and whether the patient is symptomatic. 6 Conservative management includes bed rest; head elevation; avoidance of the Valsalva maneuver (nose blowing and coughing); and administration of antibiotics, antipyretics, analgesia, osmotic diuretics, and normobaric and hyperbaric oxygen. In the case of benign pneumocephalus associated with small bony defects, conservative management usually resolves the problem. 12 In otogenic pneumocephalus, surgery is indicated when conservative management fails to achieve remission of pneumocephalus and when patients have impaired consciousness and tension pneumocephalus. 12 The pressure of the trapped air in tension pneumocephalus results in herniation of the brainstem, compression of the brain parenchyma, and cerebral edema. 10,13 To save patients’ lives, emergency decompression is necessary to alleviate pressure on the brain parenchyma. The treatment options include the drilling of burr holes, air aspiration, ventriculostomy, craniotomy, and closure of the defect. 14
The materials used for defect repair in otogenic pneumocephalus include free fascia, temporalis muscle, cartilage, cortical bone, bone cement, and fibrin gel. The repair is performed in multiple combination and multiple layers to ensure the best defect sealing. 15
Long-term follow-up is mandatory after PBC surgery—at least once a year for 5 years. Once the cavity is obliterated, follow-up involves radiological assessment, including high-resolution CT, and T1- and T2-weighted MRI with fat suppression. 1,2
In conclusion, otogenic pneumocephalus is rarely encountered in clinical practice. Nonetheless, it should be suspected when patients present with otological and non-specific neurological symptoms. Early diagnosis and urgent management are important to prevent further complications and decrease mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by research funds from Chosun University Hospital, 2021.