
Abstract
We present a case of a 12-year-old male who presented with complaints of nasal congestion, intermittent throat pain, and odynophagia. He was taken to the operating room for inferior turbinate reduction and adenoidectomy and found to have stones within adenoid crypts. Adenoidectomy resulted in resolution of the patient’s throat pain and pain with swallowing. Not previously described in the literature, adenoid stones may represent an unrecognized etiology of odynophagia and throat pain in the pediatric population. Adenoidectomy should be considered for patients symptomatic from adenoid stones.
Introduction
Tonsil stones are a common indication for tonsillectomy. These tonsilloliths represent localized concentrations of aerobic and anaerobic bacteria that calcify overtime initially into soft gel and eventually to hard stone. They form within tonsillar crypts and may release sulfur compounds related to the metabolism of anaerobic bacteria. 1 These irritating concretions can be a great source of discomfort for patients, causing chronic sore throat, cough, dysphagia, otalgia, halitosis, and even globus sensation. Alternatively, many patients with tonsilloliths are asymptomatic. 2 While tonsilloliths are quite common in the palatine tonsil, estimated to affect 10% of the general population, 3 more rare sites of stone formation have been reported in the oral cavity. Primarily, these sites have been within Waldeyer’s ring, a circle of lymphoid tissue including the palatine tonsil, nasopharyngeal tonsil (adenoid), lingual tonsil, and tubal tonsillar tissue located adjacent to the opening of the Eustachian tube. 4 At least one incident of tonsilloliths within the lingual tonsillar tissue has been reported in an asymptomatic adult. 4 Stone formation has been reported rarely in adenoid tissue including one case report of a 30-year-old woman with nasal congestion and recurrent respiratory infections. 5 In this article, we highlight a rare case of adenoid stones in a pediatric patient.
Case Report
We report a common presentation of a 12-year-old male complaining primarily of snoring and nasal congestion as well as intermittent throat pain and odynophagia over the course of a year. The patient and parents were unable to identify alleviating or exacerbating factors. On exam, the patient was noted to have inferior turbinate hypertrophy and decreased nasal airflow. For his nasal obstruction, medical therapy with topical steroids was trialed but resulted in no change in his symptoms. After discussion of the risks and benefits with his parents, the patient was taken to the operating room for further intervention. He underwent nasal endoscopy with inferior turbinate reduction as well as transoral adenoidectomy. After the Coblator wand was used to address the turbinates, a Crowe-Davis mouth gag was advanced into the patient’s oral cavity, and a laryngeal mirror was used to carefully examine the adenoid bed. Within the lymphatic crypts, multiple stones were visualized and removed (figure 1). Afterward, the adenoid tissue was fulgurated with suction Bovie cautery. On subsequent follow-up appointments, the patient reported improvement in nasal breathing and resolution of his throat pain and odynophagia. The adenoid bed is examined using a laryngeal mirror with a stone visualized adjacent to the suction Bovie.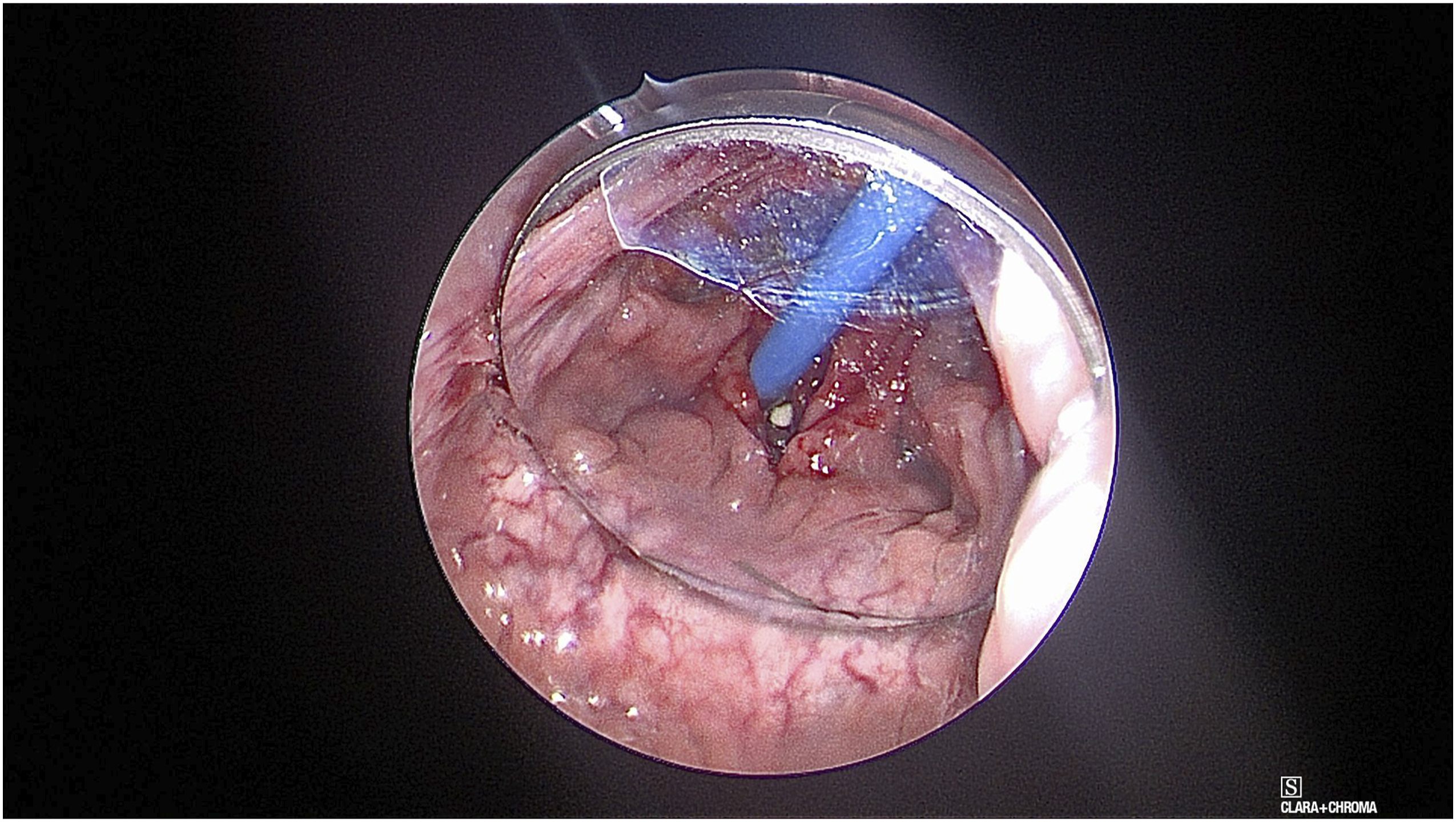
Discussion
Surgical excision of the adenoid bed is the third most common pediatric procedure performed in the ambulatory setting in the U.S. 6 Most commonly, the procedure is performed to address conditions such as obstructive sleep apnea, nasal obstruction, chronic otitis media, and chronic adenitis. 6 Many providers will perform adenoidectomy for recurrent sinonasal disease prior to consideration of functional endoscopic sinus surgery. 7 Of note, the procedure is also commonly performed as a combined procedure with tonsillectomy or ventilating tube placement. 8 Surgical techniques used for the procedure include electrocautery, coblation, and microdebrider. 6 No significant differences have been shown in complication rate or surgical time between the different techniques for adenoidectomy. 6 Of note, electrocautery adenoidectomy iss significantly less expensive than microdebrider or Coblator adenoidectomy. 6 Tonsillectomy for palatine tonsils for chronic sore throat has been described in the literature. 9 Observational studies have shown that tonsillectomy in these children resulted in fewer infections and improved disease-specific and global quality of life measures. 9
Conclusion
This unique case demonstrates a likely underreported phenomenon of stone formation in the nasopharyngeal tonsillar tissue leading to chronic throat pain and odynophagia. Adenoidectomy allowed for symptom resolution in this child. Adenoidectomy should be considered for pediatric patients symptomatic from adenoid stones.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.