
Abstract
Introduction
Chronic rhinosinusitis (CRS) has a high prevalence, symptom burden, and financial costs. 1 CRS in children aged 0 to 20 years results in 7.5 million visits per year in the United States with the majority of visits in children aged 6 years and older. 2 Therefore, optimization of treatment options for this patient population is critical.
Pediatric CRS (PCRS) is defined as signs and symptoms of nasal congestion, colored nasal discharge, facial pressure or pain, or cough that have been present for 12 or more weeks. Two or more symptoms are required to diagnose PCRS along with evidence of sinonasal inflammation using either nasal endoscopy or computed tomography (CT) scan.3-5 CT imaging with Lund-Mackay (LM) score of ≥5 have high positive predictive value for PCRS, whereas scores of 3 to 4 may be equivocal depending on clinical context. 6
Treatment consists of medical management followed by adenoidectomy in medically refractory cases. 7 The adenoid has been implicated in pediatric sinus disease although the exact mechanism remains unclear. Research indicates that bacteria harbored within adenoid biofilms contribute to PCRS. 8 Adenoidectomy is the most commonly performed surgical intervention.9,10 The American Academy of Otolaryngology considers adenoidectomy as a first-line surgical therapy for PCRS in children up to age 12 years. However, there was a stronger consensus regarding the effectiveness of adenoidectomy for patients aged up to 6 years compared to patients aged 6 to 12 years. 4
Given the high prevalence and symptom burden of PCRS, 1 it is important to identify the effectiveness of adenoidectomy for children aged 6 years and older. The aim of this clinical research study is to further delineate the effectiveness of adenoidectomy in the treatment of PCRS based on patient age. The present study is the first to investigate whether age is associated with adenoidectomy success in the treatment of PCRS.
Patients and Methods
This retrospective cohort study was approved by West Virginia University institutional review board (Protocol Number: 2004956868). Given the retrospective nature of the study, the study was exempt from requiring informed consent from the patients. Patients seen in the pediatric rhinology clinic over a 10 year period were reviewed and included if they met PCRS definition and underwent adenoidectomy only after failed medical management. PCRS was defined as 2 or more symptoms of nasal congestion, colored nasal discharge, facial pressure or pain, or cough that have been present for 12 or more weeks, as assessed by the PCRS symptoms screening questionnaire in Figure 1; with evidence of sinonasal inflammation using either nasal endoscopy or CT imaging.3,5 To be included in the study, patients must have been experiencing congestion, discharge, pressure/pain, and/or cough prior to and after medical management thus necessitating an adenoidectomy procedure. Patients were excluded if following medical management, they had undergone endoscopic sinus surgery (ESS) as an initial surgical intervention prior to adenoidectomy. Figure 2 shows a scan of the sinuses with persistent signs of CRS after maximal medical management. Patients were excluded if they had cystic fibrosis, primary ciliary dyskinesia, complicated acute sinusitis, immune deficiency disorders, prior functional ESS intervention, allergic fungal sinusitis, or a LM CT score of 2 or lower.
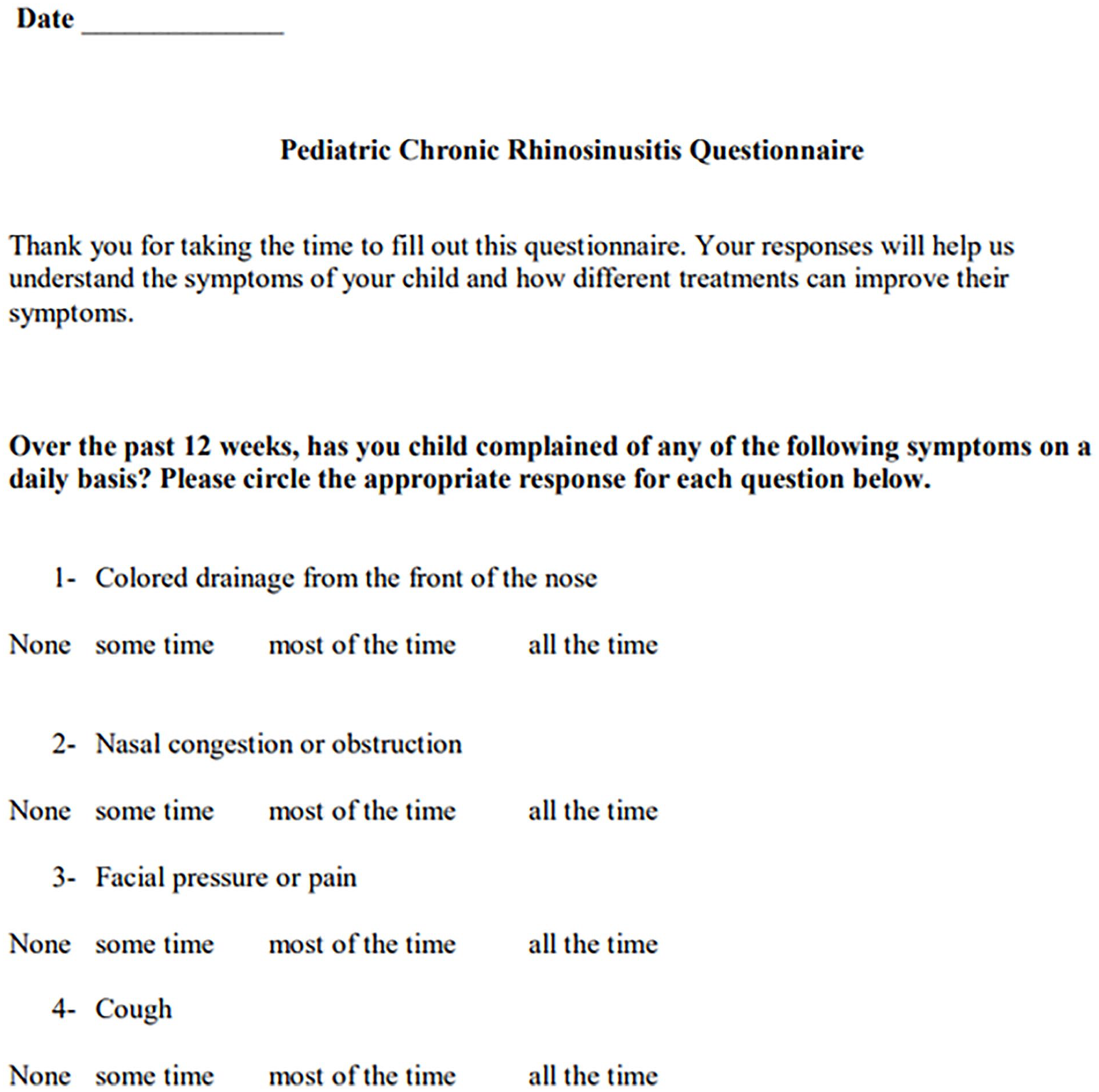
PCRS symptoms screening questionnaire. PCRS, pediatric chronic rhinosinusitis.
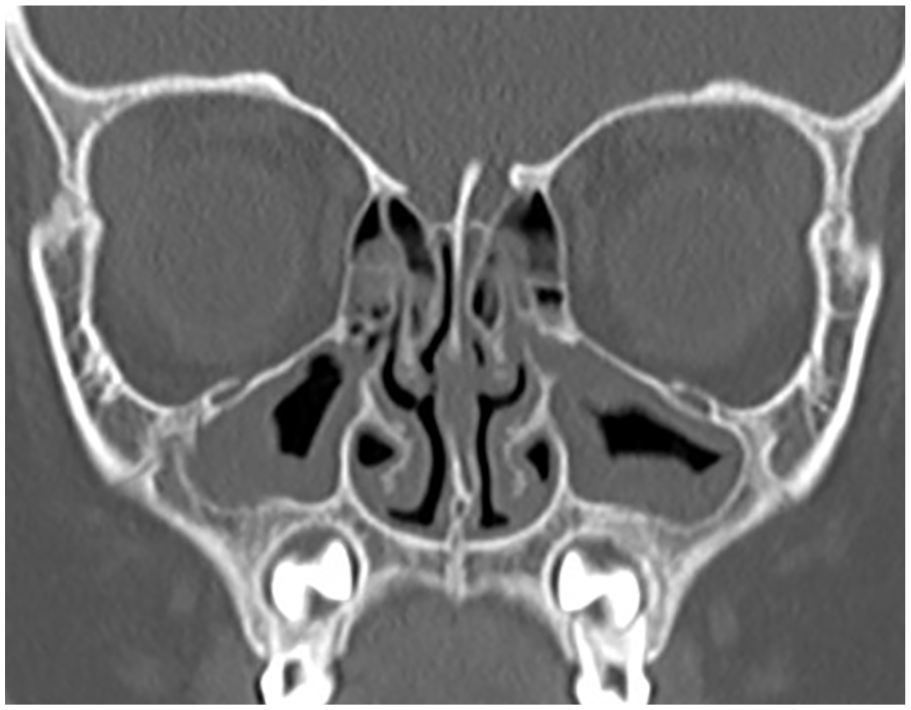
Coronal CT scan of sinuses after maximal medical therapy showing opacification of both maxillary sinuses as well as anterior ethmoid sinuses. CT, computed tomography.
All patients received standard maximal medical therapy prior to adenoidectomy, which included a course of antibiotic therapy, topical nasal and/or systemic corticosteroids, and nasal saline irrigation. 3 Medical management was usually 8 weeks long before patients were reevaluated. However, the time from medical management failure, determined at the 8 week follow-up, to adenoidectomy varied. ESS was performed only after failure of both standard medical treatment and adenoidectomy as indicated by the persistence of PCRS symptoms.
Demographic data collected included age, gender, allergic rhinitis, and asthma statuses. Adenoidectomy outcomes were assessed using a questionnaire on cardinal PCRS symptoms: (1) purulent nasal discharge, (2) nasal obstruction, (3) facial pressure/pain, and (4) cough. Figure 3 shows a copy of the PCRS symptoms assessment questionnaire. Surgical success was defined by the resolution of 50% or more of the symptoms based on the questionnaire whereas failure was defined by the persistence of 50% or more of the PCRS symptoms and/or the need for additional surgical intervention. Patients were followed postoperatively, every 3 months, for at least 12 months, and continued nasal saline sprays and intranasal steroid sprays for any persistent postoperative sinonasal symptoms.
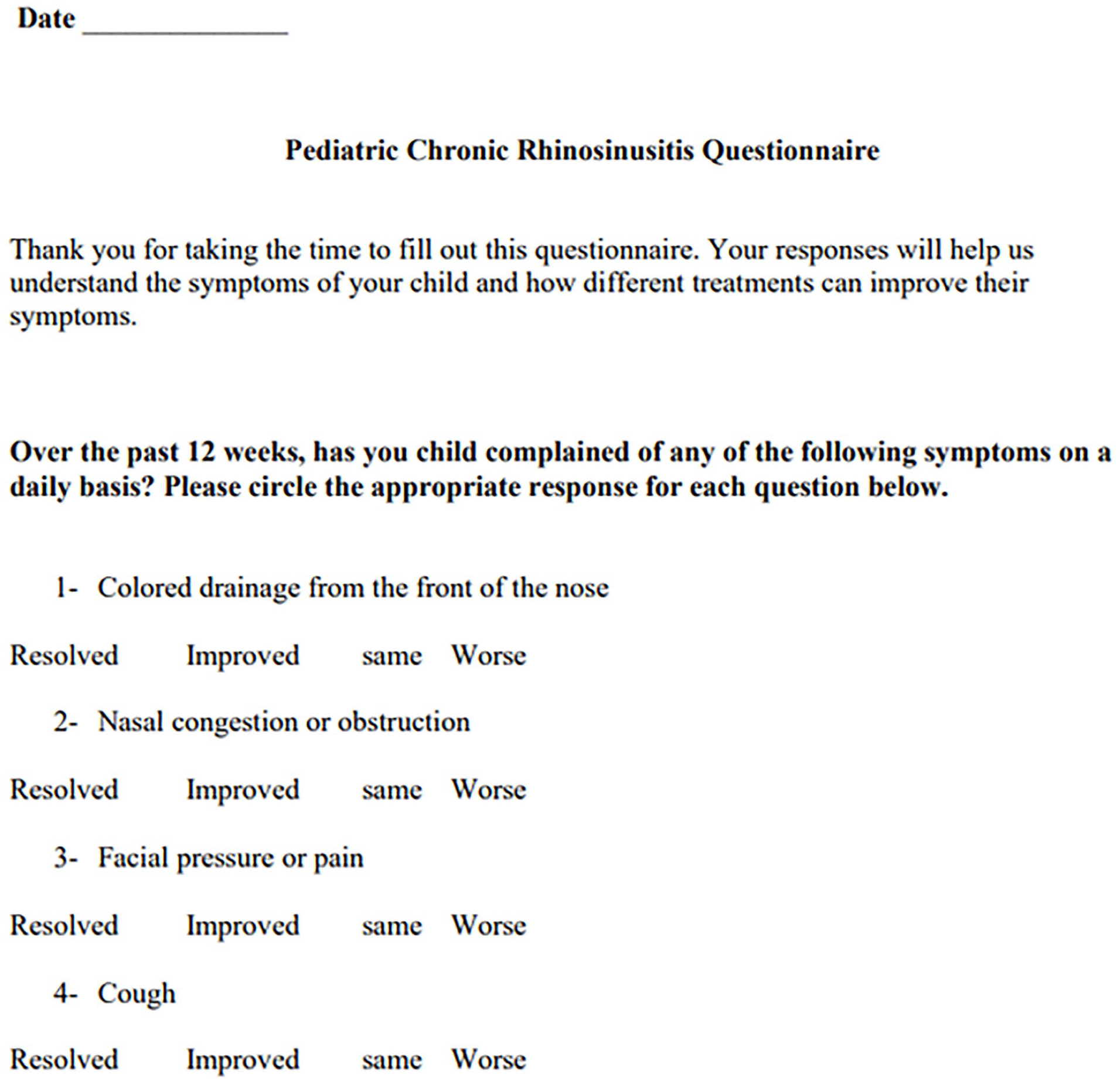
PCRS symptoms assessment questionnaire. PCRS, pediatric chronic rhinosinusitis.
Data Analytic Plan
Univariate chi-square analyses were conducted to investigate whether sex (male vs female), allergic rhinitis diagnosis (yes vs no), and asthma diagnosis (yes vs no) were associated with surgical outcomes (success vs failure). Univariate analyses of variance were conducted to investigate whether age (continuous) and LM CT scores (continuous) were associated with surgical outcomes. Variables that were significantly associated with surgical outcomes at the univariate level were then included in a multivariate binary logistic regression model to predict outcomes. Statistical analysis was performed with SAS statistical software (SAS Institute Inc) with P = .05.
Results
The sample consisted of 107 patients with an average age of 4.88 years (SD = 2.54; range = 1-13 years). The majority of patients were male (58.88%), and allergic rhinitis and asthma were each comorbid in 44.2% of patients. Patients’ demographic characteristics are presented in Table 1. Patients who had success with the procedure were on average age 5.46 years (SD = 2.83) whereas patients who did not have success were on average age 4.36 years (SD = 2.40; F = 4.06, P = .047). Surgery was successful in about two-thirds of children aged ≥6 years (68%) but less successful in children younger than 6 years (39%). Patients who had success had lower average LM CT scores [mean (M) = 6.93, SD = 3.81] compared to patients who did not have success with the procedure (M = 8.63, SD = 3.48; F = 4.14 P = .045). Success rates did not differ by sex (χ2 = .01, P = .93), allergy (χ2 = .35, P = .55), and asthma diagnoses (χ2 = .60, P = .11). When age and LM CT scores were both entered into a multivariate binary logistic regression model simultaneously, neither age nor LM CT scores remained significant in predicting surgical outcomes [β = .13, standard error (SE) = .10, P = .20; β = −.09, SE = .07, P = .20; respectively]. Patients’ clinical characteristics by surgery success are presented in Table 2.
Patient Demographic Characteristics by Age Group.
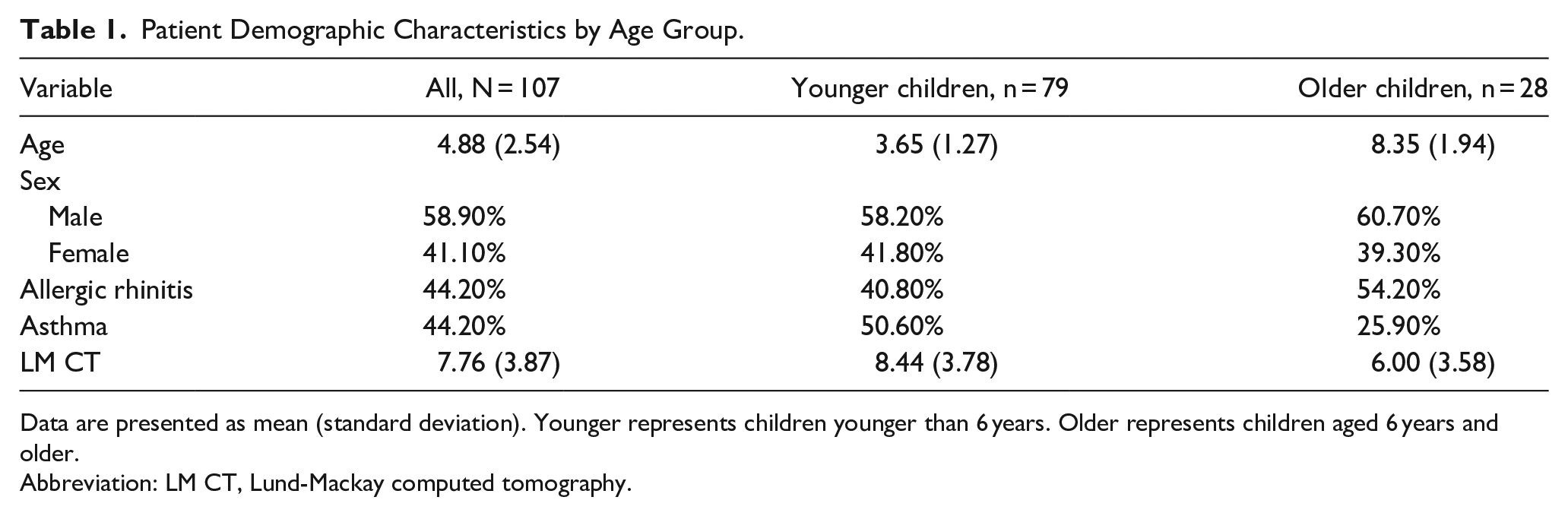
Data are presented as mean (standard deviation). Younger represents children younger than 6 years. Older represents children aged 6 years and older.
Abbreviation: LM CT, Lund-Mackay computed tomography.
Patient Clinical Characteristics by Surgical Outcome Group.
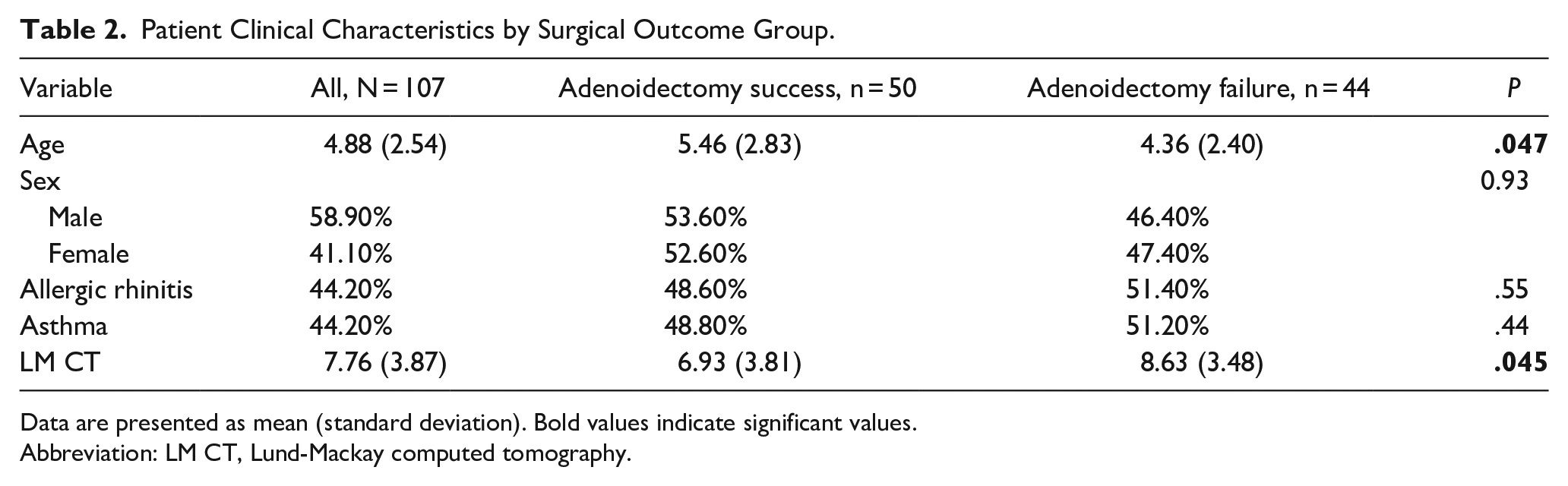
Data are presented as mean (standard deviation). Bold values indicate significant values.
Abbreviation: LM CT, Lund-Mackay computed tomography.
Of the 44 patients who did not experience surgical success with adenoidectomy, 12 (27%) underwent surgery with ESS. Age did not differ in those who did and did not undergo ESS (M = 4.43 years, SD = 2.27; M = 4.94, SD = 2.57; respectively, P = .52). Patients’ clinical characteristics by ESS group are presented in Table 3.
Patient Clinical Characteristics by ESS Group.
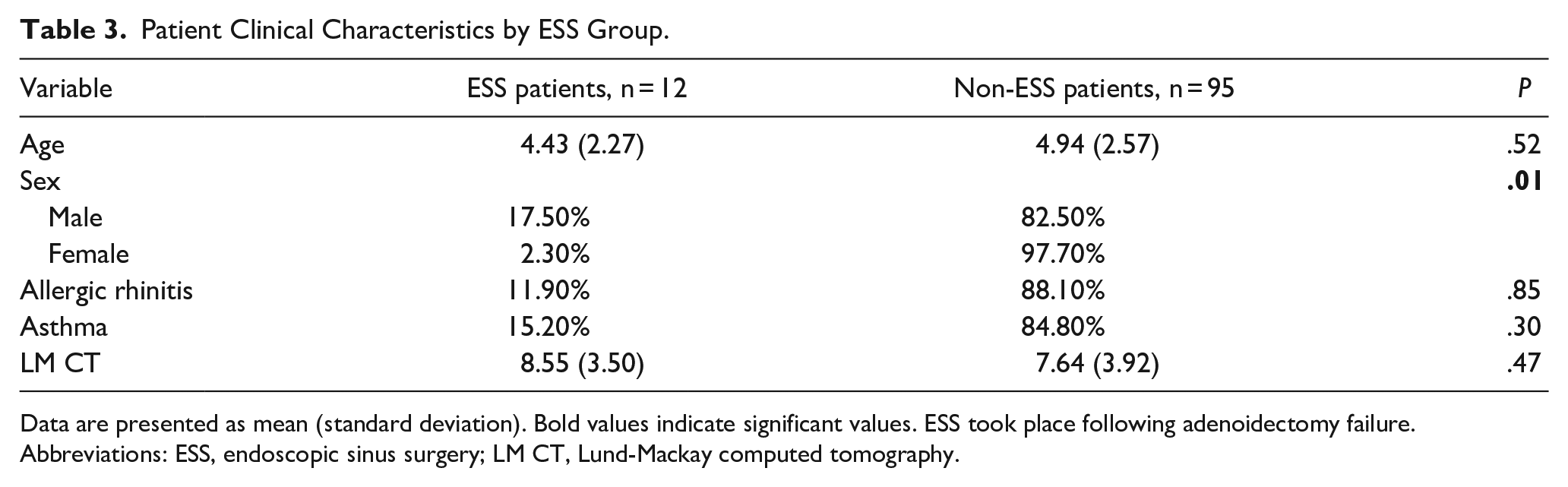
Data are presented as mean (standard deviation). Bold values indicate significant values. ESS took place following adenoidectomy failure.
Abbreviations: ESS, endoscopic sinus surgery; LM CT, Lund-Mackay computed tomography.
Discussion
Adenoidectomy is the most common first-line surgical treatment in PCRS after the failure of maximal medical therapy. ESS is more effective than adenoidectomy but is often reserved for older children and those with more severe disease or complicated presentations.11,12 Although clinical guidelines support the use of adenoidectomy as a first-line treatment for PCRS, those guidelines note that there is less consensus for adenoidectomy in children aged 6 years and older compared to those younger than 6 years. 4 There is a growing literature on surgical treatment for PCRS13,14; however, no studies to date have demonstrated an association between age and likelihood of adenoidectomy success for PCRS. A systematic review by Brietzke and Brigger 15 demonstrated an overall pooled effectiveness of 69% for PCRS with adenoidectomy alone. 15
Our study investigated predictors of adenoidectomy success among pediatric patients with PCRS. In our patient population, all children had PCRS refractory to maximal medical therapy and consequently underwent adenoidectomy. ESS was performed in 12 patients due to persistent PCRS symptoms after adenoidectomy. In our study, we found that older age was associated with greater adenoidectomy success rate of 68% in children aged 6 years and older, similar to the article of Brietzke and Brigger 15 ; however, children younger than 6 years had success rates of only 39%. These findings of higher success rates in older children are consistent with recent research by Mahomva et al 16 that showed that adenoidectomy alone provided significant symptom control and medication reduction in children aged 7 years and older. Our study’s finding of greater adenoidectomy success rates in older children provides support for adenoidectomy as the initial surgical therapy for PCRS in those aged 6 years and older.
CT imaging is useful for the diagnosis of PCRS and may have some prognostic value. All patients in our study received CT imaging. Bhattacharyya et al 6 demonstrated that a CT LM score with a cutoff level of 5 may be considered diagnostic for PCRS, a score of 3 to 4 is equivocal and hinges on clinical judgment, and a score of 0 to 2 ruled out PCRS. 6 All patients in our study had CT imaging with scores of 3 or more. We demonstrated that adenoidectomy success was associated with having lower LM CT scores. Those with higher LM scores may have more complex pathophysiology, thus warranting caution in the use of adenoidectomy alone. 17 Future studies may investigate whether pediatric patients with high LM CT scores may benefit more from ESS as compared to adenoidectomy.
Our study has several limitations. The small sample size may have limited our statistical power to detect significant effects, which is one possible explanation for why neither age nor LM CT score remained significant on our multivariate binary logistic regression. Four patients were 11 years or older, thus limiting the generalizability of findings to adolescent populations. Last, the few patients with lower LM CT scores could have instead had chronic adenoiditis mimicking PCRS.
Adenoidectomy is an accepted initial surgical therapy for PCRS in children aged up to 12 years, but there is less consensus for the 6 to 12 years age group compared to those less than 6 years. Our study was the first to demonstrate an association between age and the likelihood of adenoidectomy success for PCRS. These findings indicate that adenoidectomy is a good first-line surgery for children aged 12 years and younger, especially in the 6 to 12 years group which had a high rate of success with 68% experiencing remission of symptoms after surgery.
Footnotes
Authors’ Note
This article was presented at the COSM 2023: Combined Otolaryngology Spring Meetings; Boston, MA; May 3 to 7, 2023.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the institutional review board of West Virginia University, Morgantown, WA, USA (Protocol Number: 2004956868).
Informed Consent
This study consisted of retrospective analysis of data collected from routine care and thus informed consent is not applicable.