
Abstract
Pemphigus is a rare autoimmune mucocutaneous bullous disease that can be life-threatening. We report a case of pemphigus vulgaris with pharyngeal ulcer as the initial presentation that was treated with glucocorticoid therapy.
Keywords
Introduction
Pharyngeal ulcer is a common oral manifestation of a systemic disease, particularly of pemphigus vulgaris. It commonly affects the soft palate, bilateral tonsils, posterior and lateral walls of the pharynx, base of the tongue, and the pyriform fossae, which are characterized by easily ruptured mucosa and ulcer surface of varying sizes and depths. It may be chronic or recurrent, and severe. The etiology is complex and is mostly associated with an inflammation, fungal infection, tumor, or a systemic autoimmune disease. Skin manifestations include blisters, bullae, and a positive Nikolsky sign.
Case report
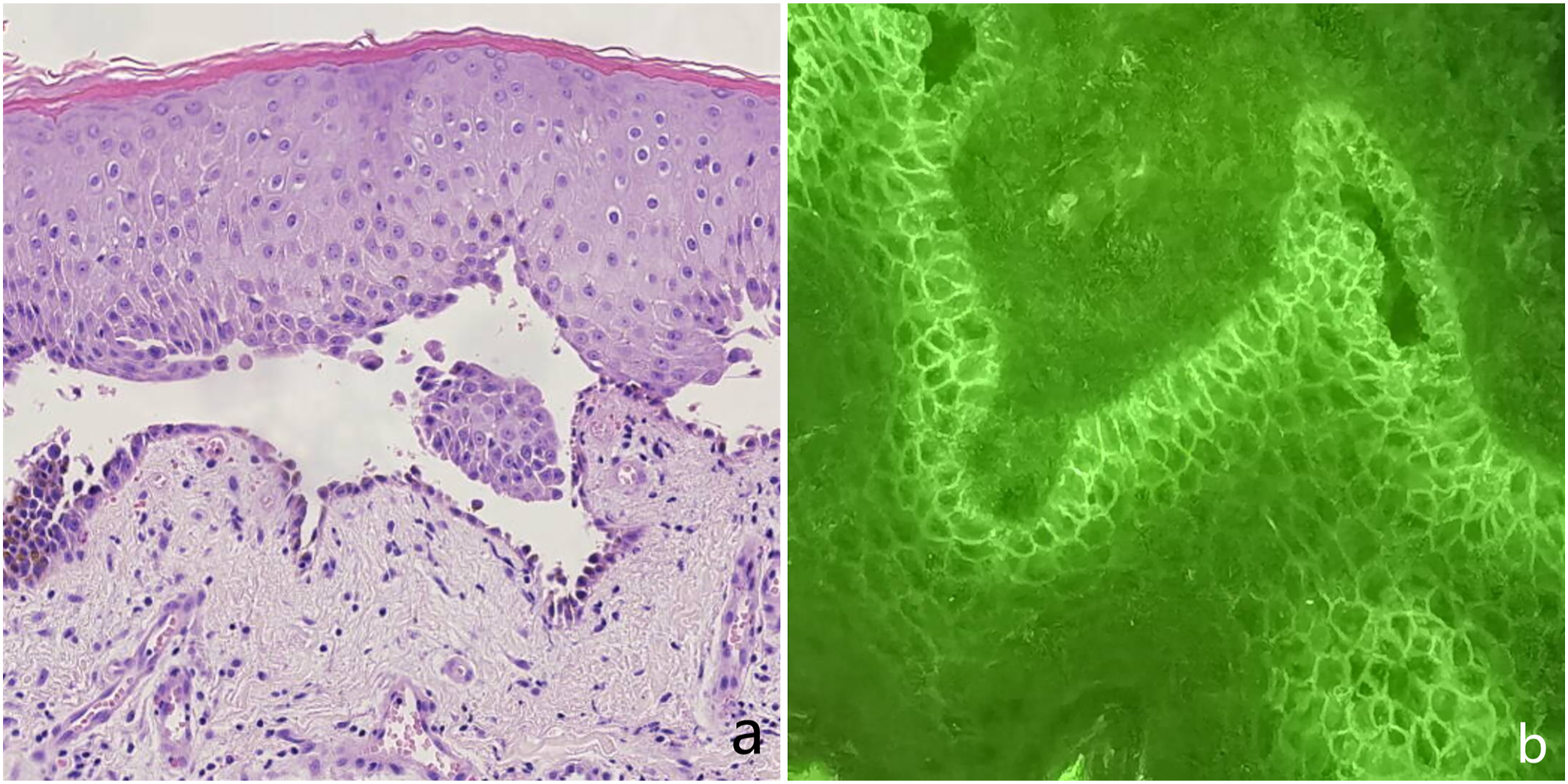
An 85-year-old, previously healthy male patient presented with pharyngeal pain for 3 months after a cold, associated with sore throat and fever (maximum temperature of 38.6°C). Electronic laryngoscopy was done and showed scattered ulcers in the epiglottis, posterior and lateral pharyngeal walls, and bilateral piriform fossae covered with white secretions (Figure 1A). After COVID-19 was ruled out, he was admitted at the hospital where he was given anti-inflammatory and hormone atomization treatment. Gram-staining of the pharyngeal ulcer surface showed Gram-negative bacilli without fungi, and the purified protein derivative (PPD) test was negative. One week later, he still complained of sore throat and blisters appeared in the oral mucosa and the lips. Two days later, the oral and anterior nasal mucosae and the lips developed erosions and exudations with scab formation (Figure 1B), the lower limbs had blisters (Figure 1C), the left eyelid margin had erosions, and conjunctival hyperemia began to develop (Figure 1D). Skin biopsy of the dorsal lesions was performed and showed epidermal hyperkeratosis and blister formation, and infiltration of pemphigus-like cells and local inflammatory cells within the epithelium (Figure 2A). Further immunofluorescence staining showed granular and mesh-like deposition of C3 in the interstitial region of the epithelial spinous layer (Figure 2B). Clinical symptoms (a) Hematoxylin-Eosin Stains; (b) Immunofluorescence stainin.
Discussion
Pemphigus is an autoimmune mucocutaneous bullous disease with an average age of onset of 50–60 years, 1 and pemphigus vulgaris (PV) is its most common and severe clinical form that can be life-threatening. Clinical manifestations include (1) multiple flaccid, easily ruptured bullae; (2) blister formation followed by progressive, refractory erosions and scabs; (3) non-inflammatory mucosal erosions and ulcers; and (4) a positive Nikolsky sign (the location of the blister and bullae is in the epidermis, which is significantly diagnostic for pemphigus). 2 Diagnosis was based on the following: (1) histopathological features of visible spinous layer cells above the basal layer and the formation of clefts or blisters and (2) direct immunofluorescence examination (DIF) showing deposits of IgG and/or complement C3 throughout the epidermis.
Glucocorticoids are the mainstay of treatment of pemphigus 3 ; moreover, immunosuppressive agents (i.e., rituximab), intravenous infusion of immunoglobulin, and plasma exchange may be added in severe cases. 4
Here, the patient was an elderly male with sore throat as his first symptom. The initial electronic laryngoscopy showed pharyngeal ulcers. As the disease progressed, erythema and blisters appeared on the skin. It was only then skin biopsy and immunofluorescence examination were performed, which delayed treatment. The glucocorticoid better controls the disease, if given early. However, in this case, it could not be controlled effectively as the dosage was insufficient and new blisters continued to appear. When the dosage was increased, disease control and symptom improvement were achieved. Therefore, accurate diagnosis and early treatment are of great significance in the management of pemphigus.
Conclusions
The possibility of pemphigus should be considered in patients with sore throat and pharyngeal ulcers. Careful physical examination, and targeted laboratory, and histopathological examination should be done to arrive at an accurate diagnosis, provide early treatment, and achieve long-term remission.
Footnotes
Appendix
Acknowledgments
We would like to acknowledge Dr. Wensheng Ge for general guidance and providing clinical materials.
Authors’ Contributions
Dong Liu: data collection and manuscript preparation; Maocai Li: manuscript preparation; Lianqing, Lili Gong: collecting pictures; Zuping Zhang: manuscript preparation and review. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This article was approved by the Ethics Committee of Liaocheng People’s Hospital
Informed Consent
The patient provided us informed consent for the publication of this case report.