
Abstract
Salivary gland choristoma is an extremely rare middle ear pathology. We present the case of a 10-year-old girl with unilateral conductive hearing loss. Tympanotomy showed a nonspecific middle ear mass, absence of stapes, anomaly of incus, and displaced facial nerve. It was not possible to remove the mass completely. Histology confirmed salivary gland choristoma. The hearing in this case can be improved with a bone-anchored hearing aid.
Introduction
Choristoma is not a tumor, but rather a remnant of histologically normal tissue in an embryologically abnormal site. 1 In very rare cases, benign salivary gland tissue can be present in the middle ear cavity. To date, just 38 such cases in adults and 10 in children have been reported.
We present the case of a 10-year-old girl with unilateral conductive hearing loss caused by salivary gland choristoma with unique malformation of the middle ear.
Case Report
A 10-year-old girl was referred to the Department of Paediatric Otorhinolaryngology of our tertiary referral hospital. The parents complained of unilateral hearing loss on the right side as identified by her pediatrician during a standard examination at 10 years of age. The patient had no history of ear problems (no otitis media), but only had recurrent infections of the upper respiratory tract due to which she had had an adenoidectomy at 5 years of age. Otoscopy examination showed normal tympanic membrane and type A tympanometry. Pure tone audiometry showed conductive hearing loss on the right side (Figure 1).
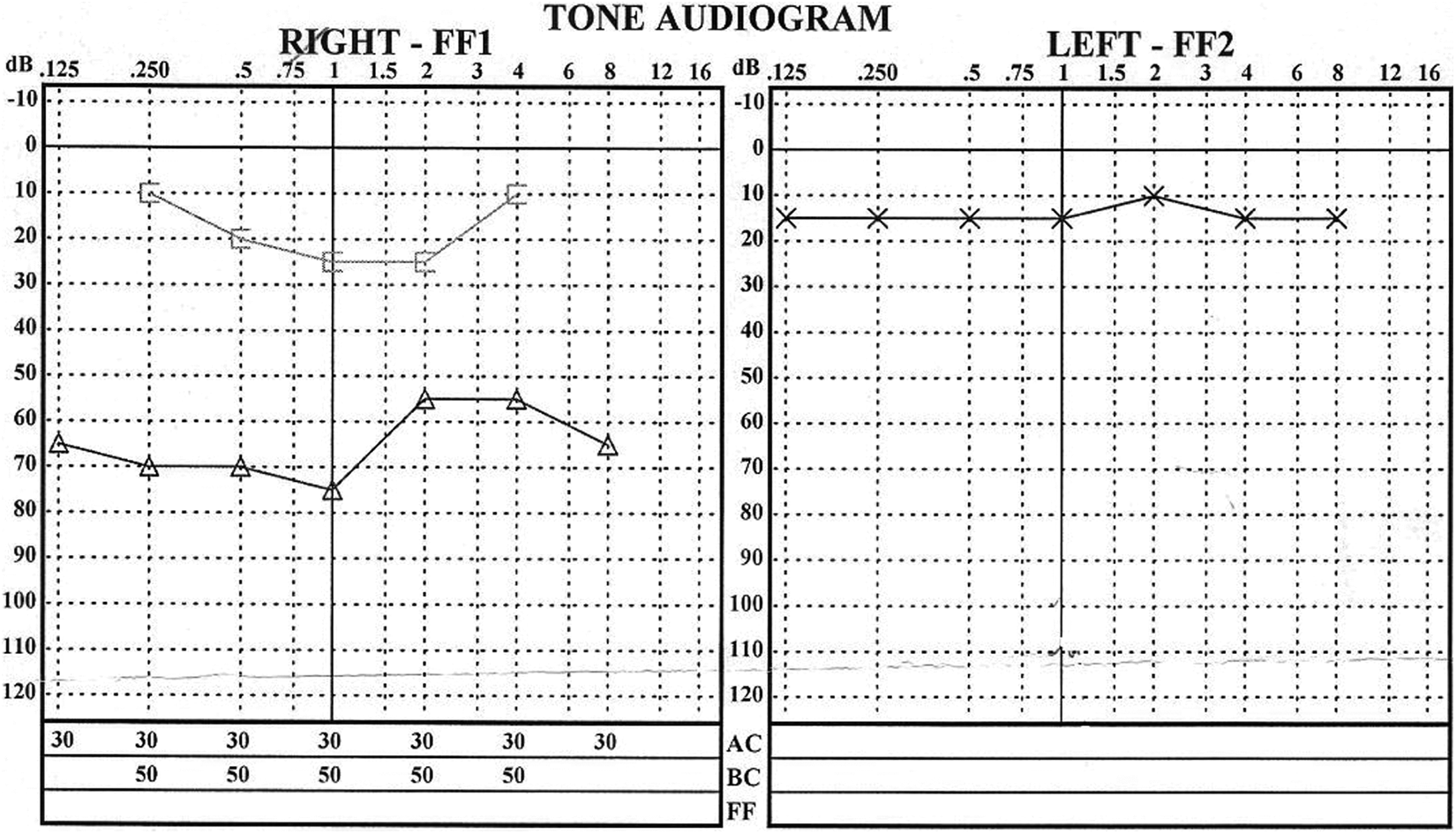
Pure tone audiogram: Conductive hearing loss on the right side.
The primary suspicion was congenital cholesteatoma behind an intact tympanic membrane. Computed tomography (CT) scans of the temporal bones showed a soft tissue mass in the space of the tympanic cavity and atypical bone mass under this soft tissue. Only malleus and incus were identified. The mastoid cells on the right side were completely blurry. There was no erosion of the bone and the facial nerve was localized in the bony mass (Figures 2 and 3).
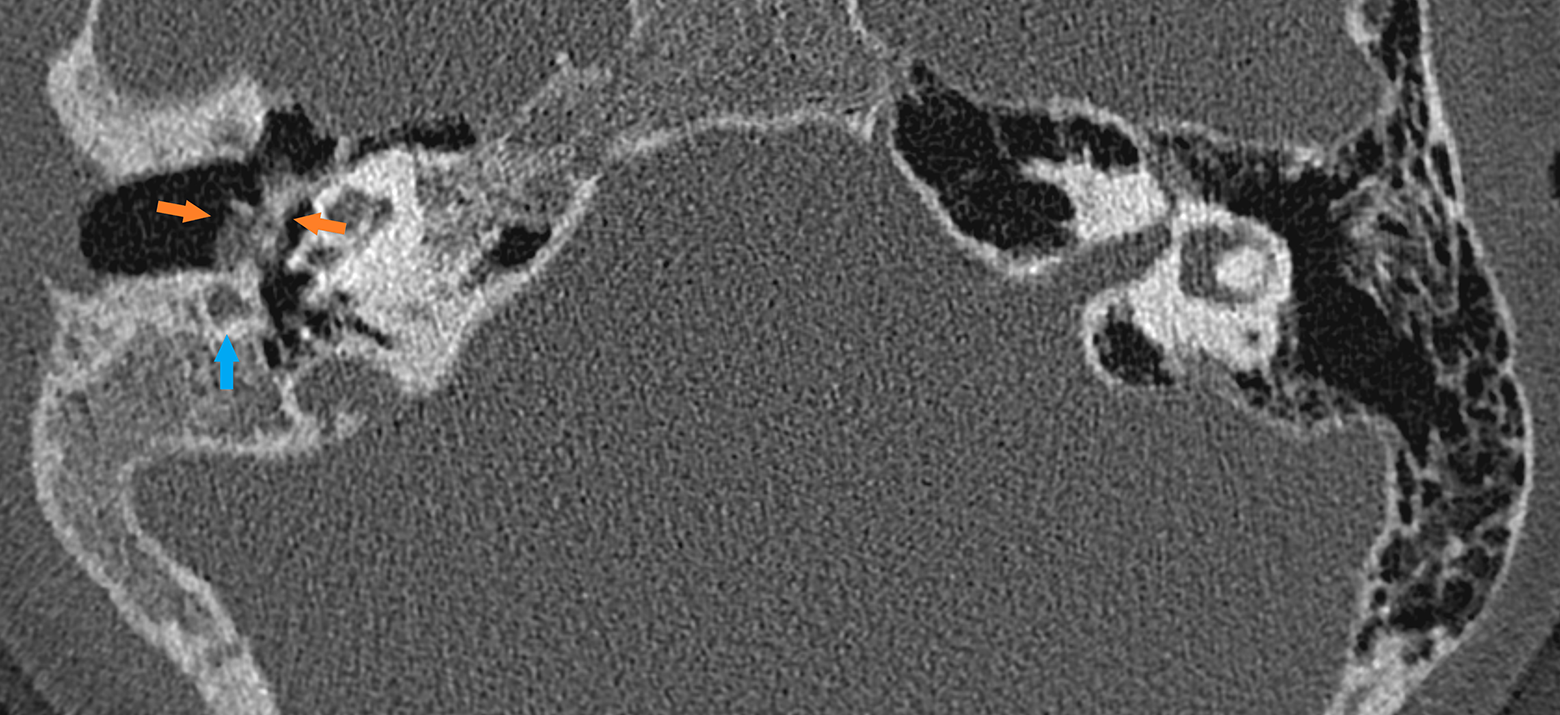
HRCT, axial scan, soft tissue mass and bony bridge in the tympanic cavity. HRCT indicates high-resolution computed tomography.
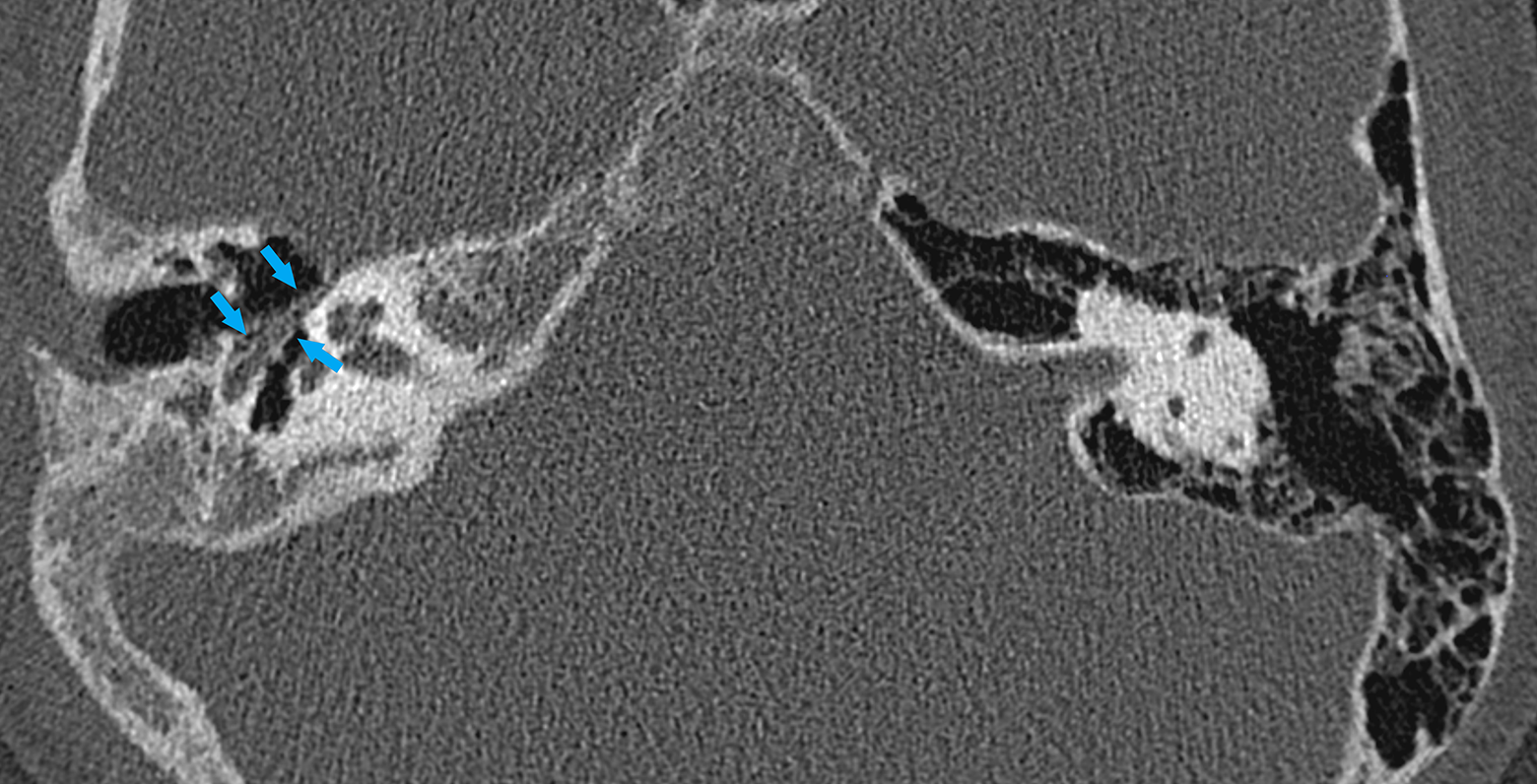
HRCT, axial scan, facial nerve in bony mass in the tympanic cavity. HRCT indicates high-resolution computed tomography.
Surgery was indicated, the aim being complete removal of the tumor and reconstruction of the middle ear ossicles. We performed tympanotomy using the retroauricular transmeatal approach. Perioperative findings revealed soft tissue limited to the tympanic cavity, and a hard bridge of bone was localized under this tissue. This bridge had its origin in the tympanic bone and adhered to the promontorium. There was no stapes, only anomalous incus. The facial nerve was localized in the bony bridge. It was not possible to remove the mass completely. The surgery achieved tumor biopsy without any peri- or postoperative complications. A definitive histopathological examination confirmed a presence of salivary gland tissue in the middle ear cavity (Figure 4). The patient was followed up for 2 years, with no evidence of progression in conductive hearing loss. The parents are waiting for the possibility to use a bone-anchored hearing aid.
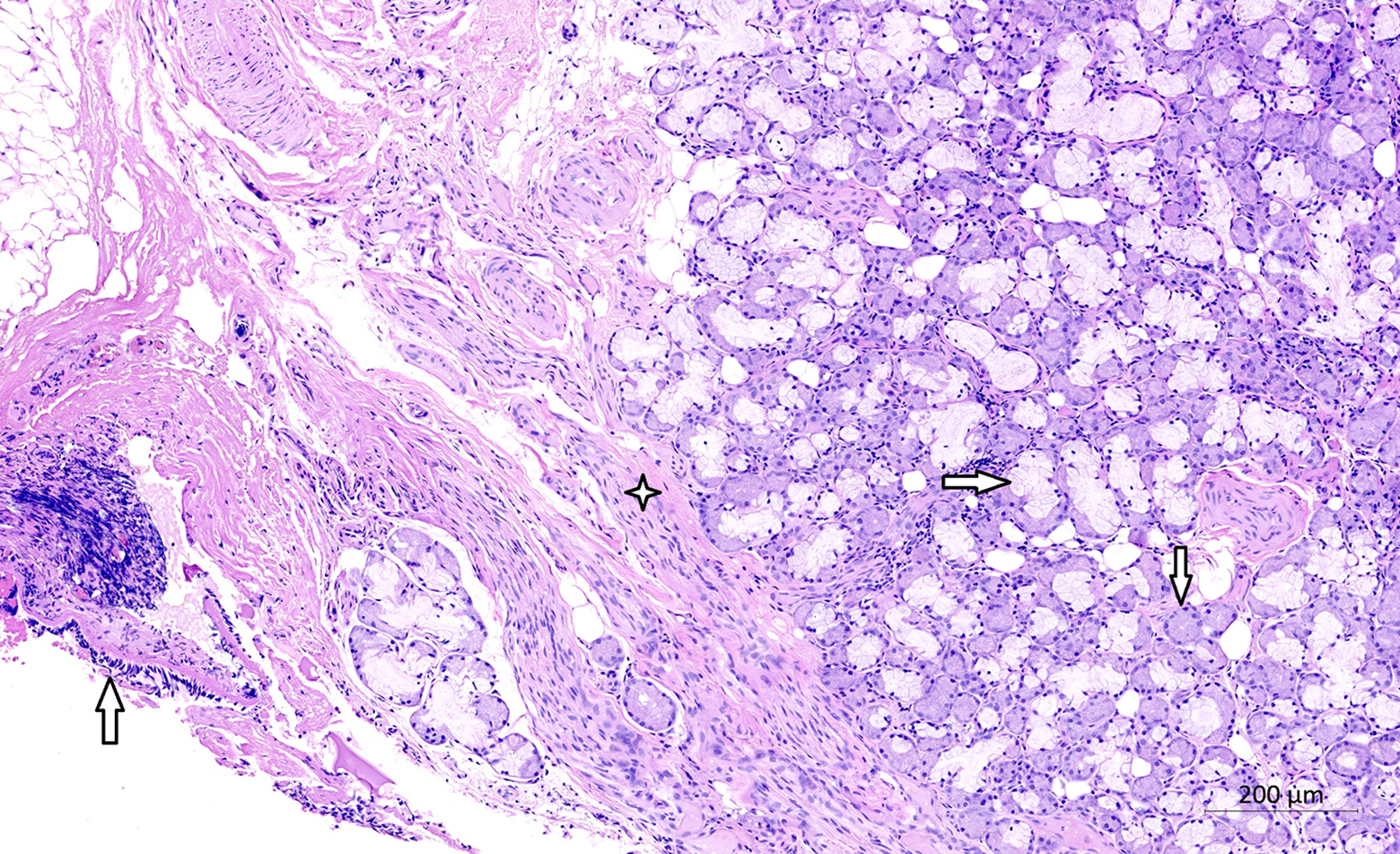
Histology of salivary gland choristoma of the middle ear, Hematoxylin-eosin, *collagen fibres, ⇒serous acinus, ↓mucinous tubule, ↑middle ear mucosa.
Discussion
Salivary gland choristoma of the middle ear is a rare pathology first described by Taylor and Martin in 1961. 2
Typical symptoms include unilateral conductive hearing loss, ear fullness, tinnitus, otalgia, and otorrhea. 3 In our patient, only unilateral conductive hearing loss was present. In some cases, malformation of the external ear or neck is reported. 4 Salivary gland choristoma of the middle ear is hypothesized to form due to malformation of the second branchial arch prior to the fourth month of gestation. 5 Salivary tissue becomes trapped in the middle ear during fusion of the tympanic ring with the temporal bone. 6 Abnormal second branchial arch development may also underpin the frequent findings of malformed incus, stapes, and facial nerve canal. During surgery, we identified the anomalous incus and a bony bridge adhering intimately to the promontorium and the facial nerve localized in the bony bridge. This is a unique finding. There was no stapes and no round window in the tympanic cavity.
There appears to be a left-sided and female predominance (2:1) of this pathology, 7 but in our case the tumor was localized on the right side.
Radiological findings for salivary gland choristoma are not specific. Computed tomography shows a well-demarcated soft tissue mass without bony erosion and which commonly encases the ossicular chain. Definitive diagnosis is possible only based upon histopathological examination. Differential diagnosis must include cholesteatoma, paraganglioma, schwannoma, glioma, dermoid cyst, or teratoma. 8 Because these middle ear lesions are very often small, it is better to visualize them using high-resolution CT scans rather than magnetic resonance imaging. 9 Microscopically, the salivary gland choristoma was composed of collagen fibers, serous acini, and mucinous tubules (Figure 4).
The treatment of choice for salivary gland choristoma is complete tumor resection and reconstruction of the ossicular chain. The surgical strategy depends upon the localization and size of the tumor. In our case, it was not possible to remove the tumor completely because of a large bony bridge enclosing the facial nerve and adhering to the promontorium. A conservative strategy (ie, biopsy to diagnose and follow-up; regular checkups, including radiological and audiological methods) is recommended in cases where the choristoma tissue is in intimate relationship with the facial nerve 10 and the risk of injury to the facial nerve is high. 11 Many authors have stated that complete removal of the choristoma is not necessary and the risk of malignancy is very low. 10,12 In case of destroying the middle ear ossicles, it is possible to make a reconstruction using a prosthesis (partial or total). 11 Bone-anchored hearing aids can provide a viable alternative to hearing enhancement in other cases, 13 such as the case reported here.
Conclusion
Salivary gland choristoma of the middle ear is a very rare pathology, but it should be considered in a differential diagnosis. Because it can resemble many other processes, the pathology presents a diagnostic challenge. Surgical removal and reconstruction of the ossicular chain is the treatment of choice, but, in cases of unique anomalies in the tympanic cavity, bone-anchored hearing aids can provide a good alternative to hearing repair.
Footnotes
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for the research, authorship, and/or publication of this article was provided by the Masaryk University in Brno under grant MUNI/A/1118/2020.