
Abstract
Background:
Computed tomography (CT) is the preferred noninvasive method for the evaluation of osteitis in chronic sinusitis. Some scholars believe that the bone changes associated with chronic sinusitis always show high attenuation (high density) and are positively correlated with the severity of the disease. However, sinus bone remodeling is a complex process that may cause high or low attenuation. There have been few reports on the spread of osteitis. Therefore, additional research on sinus CT is necessary.
Objective:
To observe bony changes in chronic maxillary sinusitis (CMS) by CT and reveal the mechanism.
Methods:
A retrospective study was conducted in 45 patients with unilateral CMS with bony changes in the sinus walls. The patients’ clinical data and CT results were analyzed and compared between the affected and normal sides. We propose the location, involvement, attenuation, and thickness method to evaluate CMS with osteitis.
Results:
Of the 45 patients, 40 (88.9%), 2, 12, and 7 had posterior external, medial, anterior, and superior lesions, respectively. The nasal region, sphenoid bone, palatine bone, and zygomatic arch were involved in 3, 12, 8, and 18 (40%) patients, respectively. Computed tomography indicated high attenuation in 30 (75.0%) and low attenuation in 10 (25.0%) patients; 6 (15.0%) showed new bone marrow cavities. The bone thickness was significantly different between the affected and normal sides in 40 patients (P < .001), including members of both the high- and low-attenuation groups (high-attenuation group: P < .001; low-attenuation group: P < .01). However, there was no significant difference in the thickness of the affected side between the high- and low-attenuation groups (P > .05).
Conclusions:
Chronic rhinosinusitis with bony changes may occur in the maxillary sinus walls and spread to adjacent bones. Both increased and decreased attenuation may occur in these circumstances. Analyzing the CT features of bone changes in unilateral CMS can improve the accuracy of disease diagnosis.
Introduction
The incidence of chronic rhinosinusitis (CRS) in the population is approximately 5% to 16%.1-3 Chronic rhinosinusitis impairs the quality of life and leads to a significant economic burden on society and patients. Chronic rhinosinusitis recurs easily, and one of the important reasons for the difficulty in curing CRS is that the cause of the disease persists due to bony changes in the sinus wall.4-6 Previous studies have shown that the mechanism of this phenomenon is complex,7-9 and the nomenclature has not yet been unified.10,11 The etiology includes osteitis, bone remodeling, new bone formation, and bone infection caused by CRS. Among these etiologies, there have been many reports on osteitis, and pathological studies have found that bone remodeling occurs.
Multislice helical computed tomography (MSCT) is currently the best modality for evaluating bony changes in sinusitis. 5 The assessment of CRS with osteitis involves integral and local factors. At present, the evaluation of CRS by MSCT mainly focuses on the bone thickness11,15,16 and CT attenuation (Hounsfield unit, HU),17,18 but the criteria have not been unified, and the correlation between them has not been clarified.
The anterior groups of paranasal sinuses are the most frequent sites of CRS, especially the maxillary sinus and the anterior ethmoid sinus. 17 However, the intrinsic bone thickness of the 2 groups is quite different. Previous studies have mostly focused on measurement of the ethmoid sinus, but the anterior ethmoid sinus belongs within the scope of endoscopic sinus surgery and is relatively thin and difficult to measure accurately. The maxillary sinus is quite deep, and it is difficult to reach this region by nasoendoscopy and obtain pathological samples. Thus, imaging evaluation becomes critical, and CT has even become the “gold standard.” In this study, we found that in addition to thickened bone and increased CT attenuation, chronic maxillary sinusitis (CMS) with osteitis can lead to decreased CT attenuation in the sinus walls and adjacent bony tissues.
Materials and Methods
Patients
A retrospective study was conducted in 358 patients with CRS from August 2014 to June 2020. A total of 45 patients (18 women and 27 men; average age: 48.82 ± 16.68 years; age range: 14-80 years; course of disease: 7.244 ± 6.322 years, range: 1-33 years; right side affected, 25 cases; left side affected, 20 cases) with unilateral CMS with osteitis were enrolled in this study. The normal sides were selected as controls. Patients with bilateral rhinosinusitis, fungal sinusitis, previous sinus surgery, benign and malignant tumors, maxillofacial fractures, hypoplasia or congenital anomalies of the facial bone, and severe dental artifacts were excluded. All patients underwent MSCT and were diagnosed with CMS with osteitis. A retrospective analysis of the 45 cases was performed to evaluate the clinical and imaging data; CT examination and measurements were performed, and the data were compared between the affected and normal sides. This study was approved by the medical ethics committee.
Computed Tomography Technique
Spiral CT volume scanning was performed by a GE Bright Speed 16-slice spiral CT scanner. The scanning baseline was parallel to Reid baseline, and the scan ranged from the roof of the frontal sinus to the lower margin of the maxillary alveolar process. The scanning parameters were as follows 18 : 120 kVp, 230 mAs; field of view: 17 cm × 17 cm; slice and gap thickness: 0.625 mm; and matrix size: 512 × 512. After axial CT scanning of all patients, transplanar, sagittal, and coronal multiplanar reconstruction (MPR) was performed on the ADW 4.7 workstation. The reconstruction parameters were slice and gap thickness: 1 mm; window width: 2000 HU; and level: 200 HU (adjustable).
Diagnostic Criteria and Radiological Analysis
The thickness of the bony wall was measured at the site of osteitis of the maxillary sinus wall and corresponding site on the normal side by CT. The measured regions were as previously described, 14 and the thickness of the posterior external wall of the maxillary sinus was measured. The diagnostic criteria of maxillary sinusitis were 15 soft tissue and a gas–liquid surface observed in the sinus cavity and/or mucosal thickening >3 mm. The specific evaluation of osteitis in CMS was divided into 4 parts: lesion location, involvement, attenuation on CT reconstruction, and thickness. In this article, this evaluation method is referred to simply as “LIAT.” Through MPR, continuous and dynamic observation of the original thin-slice images and analysis of the anatomical characteristics were performed on the workstation. Two senior radiologists confirmed the presence of maxillary sinusitis and osteitis and performed preoperative analysis and confirmation. If there were differences, an agreement was reached after consultation. The bony thickness was measured at the site of osteitis and the corresponding site on the normal side. Measurements were taken randomly at each site 3 times, and the mean and SD were calculated.
Statistical Analysis
Data are expressed as the mean ± SD for the respective groups. Statistical analyses were performed with GraphPad Prism software 5.0. The Wilcoxon matched-pairs test was used. A P value of less than .05 was considered significant. The following designations for the P value were applied: ns, P > .05; significant, *P < .05, **P < .01, and ***P < .001.
Results
Lesion Location
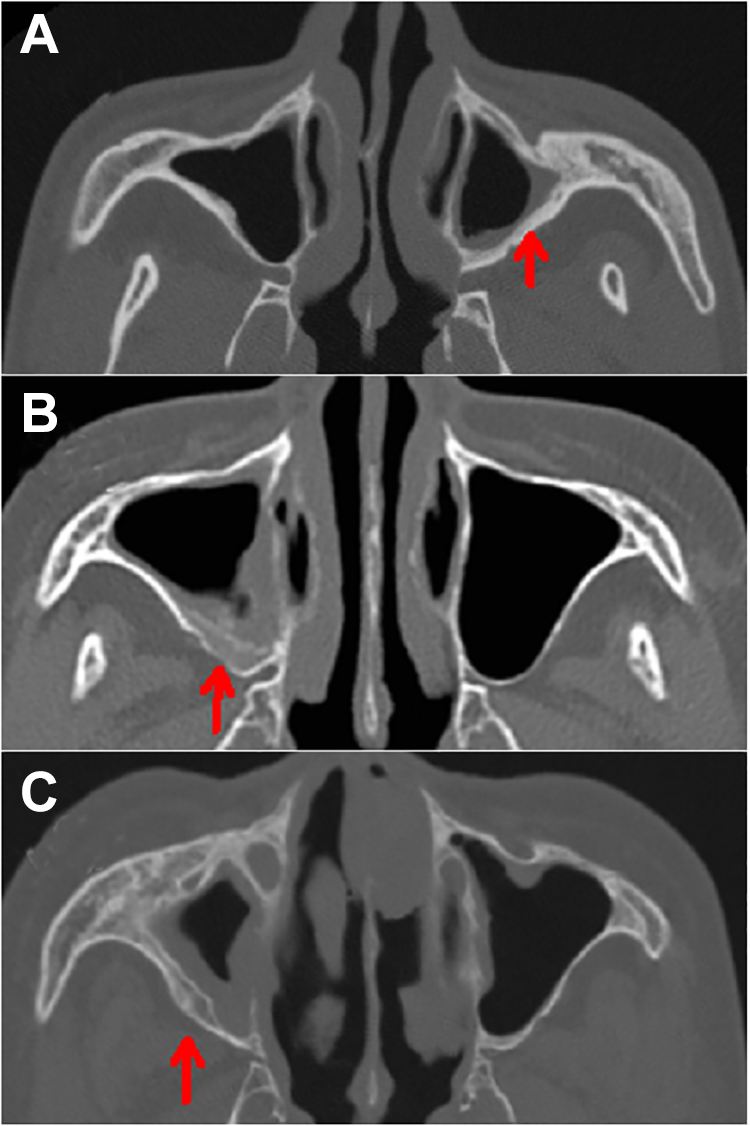
Among 45 patients (18 women and 27 men), the right side was affected in 25 cases, and the left side was affected in 20 cases. Regarding the lesion location, the lesion occurred in the posterior external wall in 40 cases, the medial wall in 2 cases, the anterior wall in 12 cases, and the superior wall in 7 cases (Figure 1A-C). The proportion of single or multiple cases of invasion of the posterior external wall of the maxillary sinus was the highest (40/45, 88.9%; Figure 2).
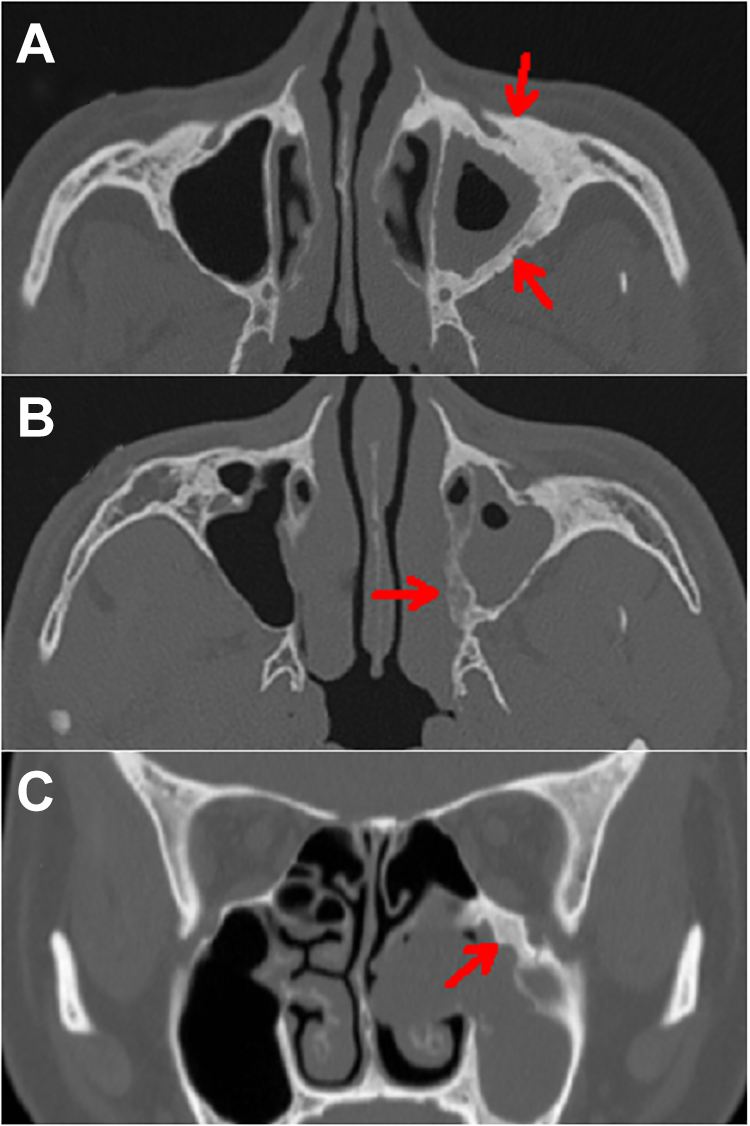
Computed tomography images of the bone window. Soft-tissue shadows were detected in the left maxillary sinus, with anterior wall and posterior external wall thickening and increased attenuation (A, red arrows), medial wall thickening and decreased attenuation (B, red arrow), and superior wall thickening and increased attenuation (C, red arrow). The maxillary sinus in the control group appeared a thin layer of cortical bone.
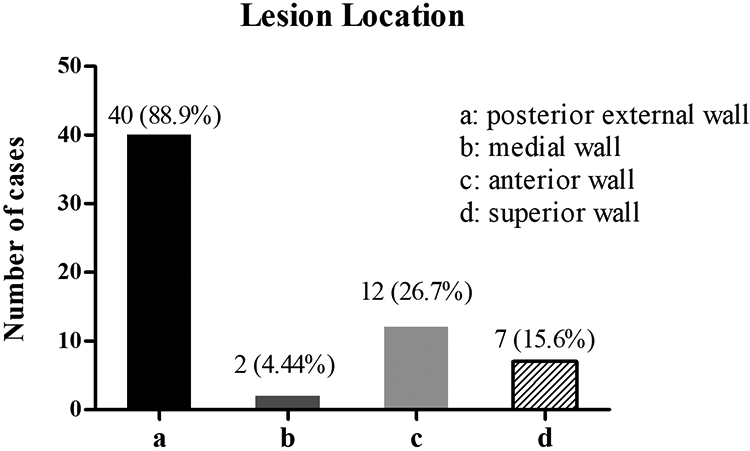
Lesion location in 45 patients with maxillary sinusitis.
Region of Osteitis Involvement
Regarding the region of involvement, osteitis expanded in 21 of the 45 patients, partially crossing the sutures and invading the adjacent bone. The nasal region was involved in 3 cases, the sphenoid bone (pterygoid process) in 12 cases, the palatine bone in 8 cases, and the zygomatic arch in 18 cases (Figure 3A-C). The proportion of single or multiple cases involving the zygomatic arch was the highest (18/45, 40.0%; Figure 4).
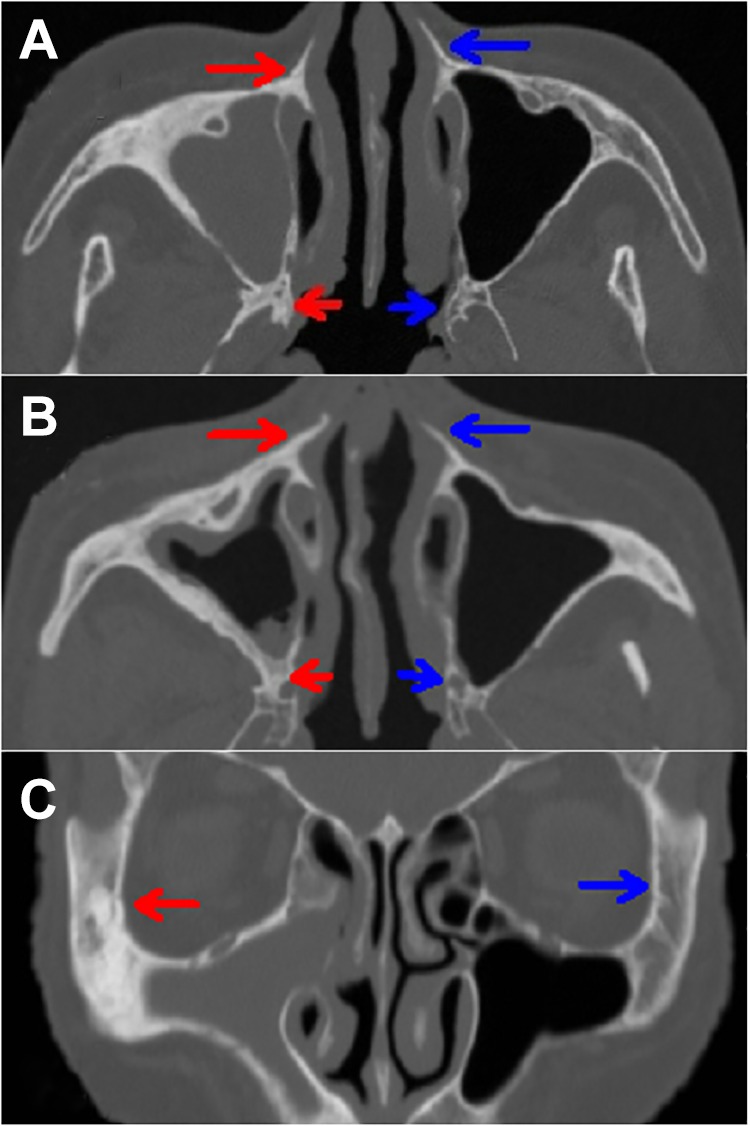
Computed tomography images of the bone window. Soft-tissue shadows were detected in the right maxillary sinus, with sinus wall thickening involving the sphenoid bone (A, short red arrow), bone in the nasal region (A, B, long red arrows), the palatine bone (B, short red arrow), and the zygomatic arch (C, long red arrow). The contralateral bone appeared normal bone histomorphology (A-C, short and long blue arrows).
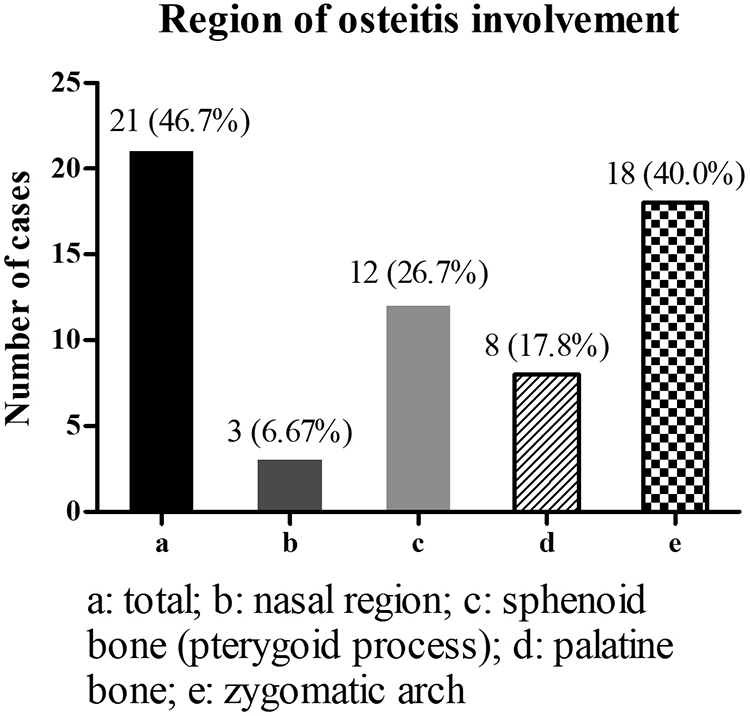
Statistics on the region of osteitis involvement.
Computed Tomography Attenuation
The posterior external wall of the maxillary sinus is a common site of osteitis, so we evaluated changes in the CT attenuation at this site. Forty patients with lesions in the posterior external wall of the maxillary sinus showed differences in CT attenuation (Figure 5A-C). Among the 40 patients, 30 (30/40, 75.0%) had high attenuation (≥500 HU), and 10 (10/40, 25.0%) had low attenuation (<500 HU; Table 1). In the low-attenuation group, 6 exhibited new bone marrow cavities (6/40, 15.0%; Figure 5C).
Computed tomography images of the bone window. High attenuation (A, red arrow) and low attenuation (B, C, red arrows) were detected in the posterior external wall of the maxillary sinus, with sinus wall thickening. New bone marrow cavities were also found (C, red arrow). The maxillary sinus in the control group appeared a thin layer of cortical bone.
Statistics on the CT Attenuation in 40 Patients With Lesions in the Posterior External Wall of the Maxillary Sinus.
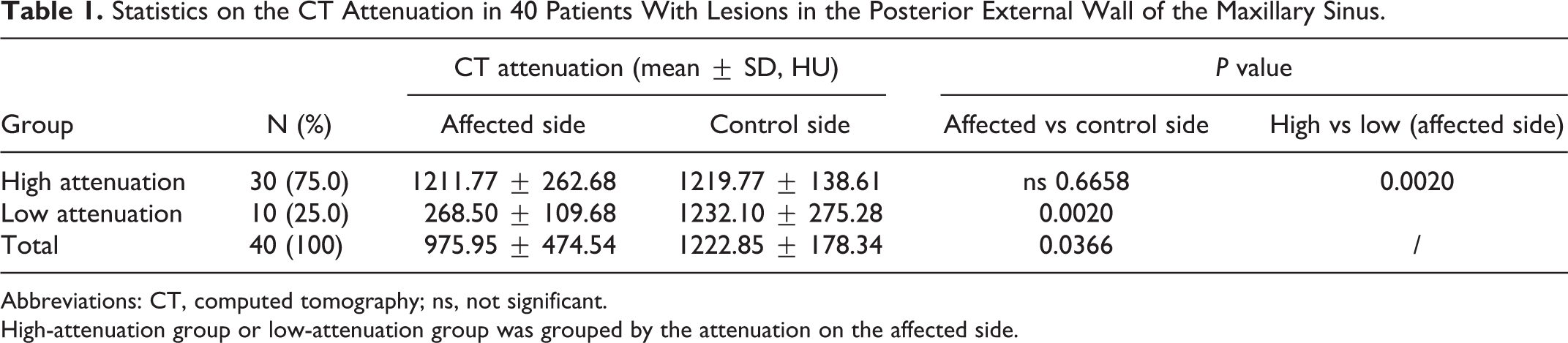
Abbreviations: CT, computed tomography; ns, not significant.
High-attenuation group or low-attenuation group was grouped by the attenuation on the affected side.
Bone Thickness
Computed tomography showed bone thickening in the posterior external wall of the maxillary sinus to varying degrees among the 40 patients. Normal sinus walls consist of thin cortical bone (Figure 6A-C). The maxillary sinus thickness on the affected side was 0.388 ± 0.121, and the thickness on the control side was 0.0933 ± 0.0369. There was a significant difference in bone thickness between the affected and control sides (P <.001). Comparing the thickness on the affected and control sides in both the high- and low-attenuation groups revealed a significant difference in the bone thickness between the affected and control sides in both groups (high-attenuation group: P < .001; low-attenuation group: P < .01). However, there was no significant difference in the thickness on the affected side between the high- and low-attenuation groups (P > .05; Table 2, Figure 7).
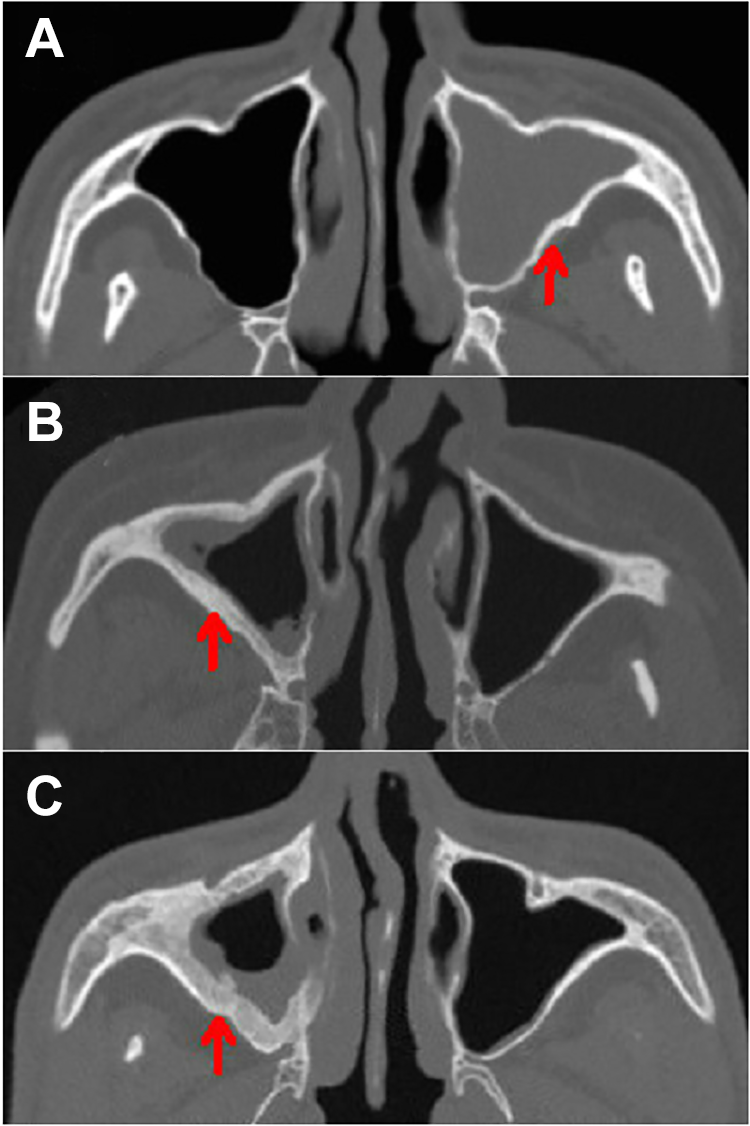
Computed tomography images of the bone window. Different degrees of bone thickening were observed in the posterior external wall of the maxillary sinus (A-C, red arrows). The maxillary sinus in the control group appeared a thin layer of cortical bone.
Statistics on the Bone Thickness in 40 Patients With Lesions in the Posterior External Wall of the Maxillary Sinus.
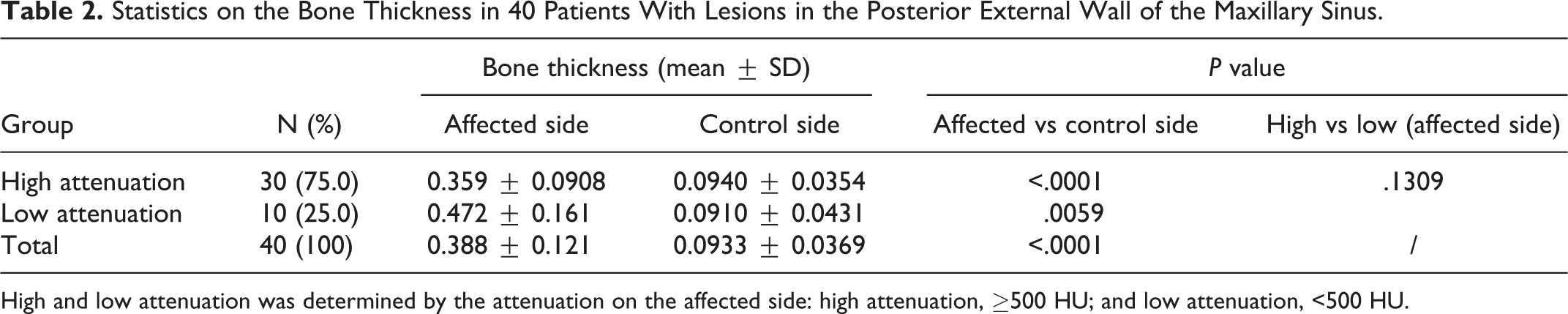
High and low attenuation was determined by the attenuation on the affected side: high attenuation, ≥500 HU; and low attenuation, <500 HU.
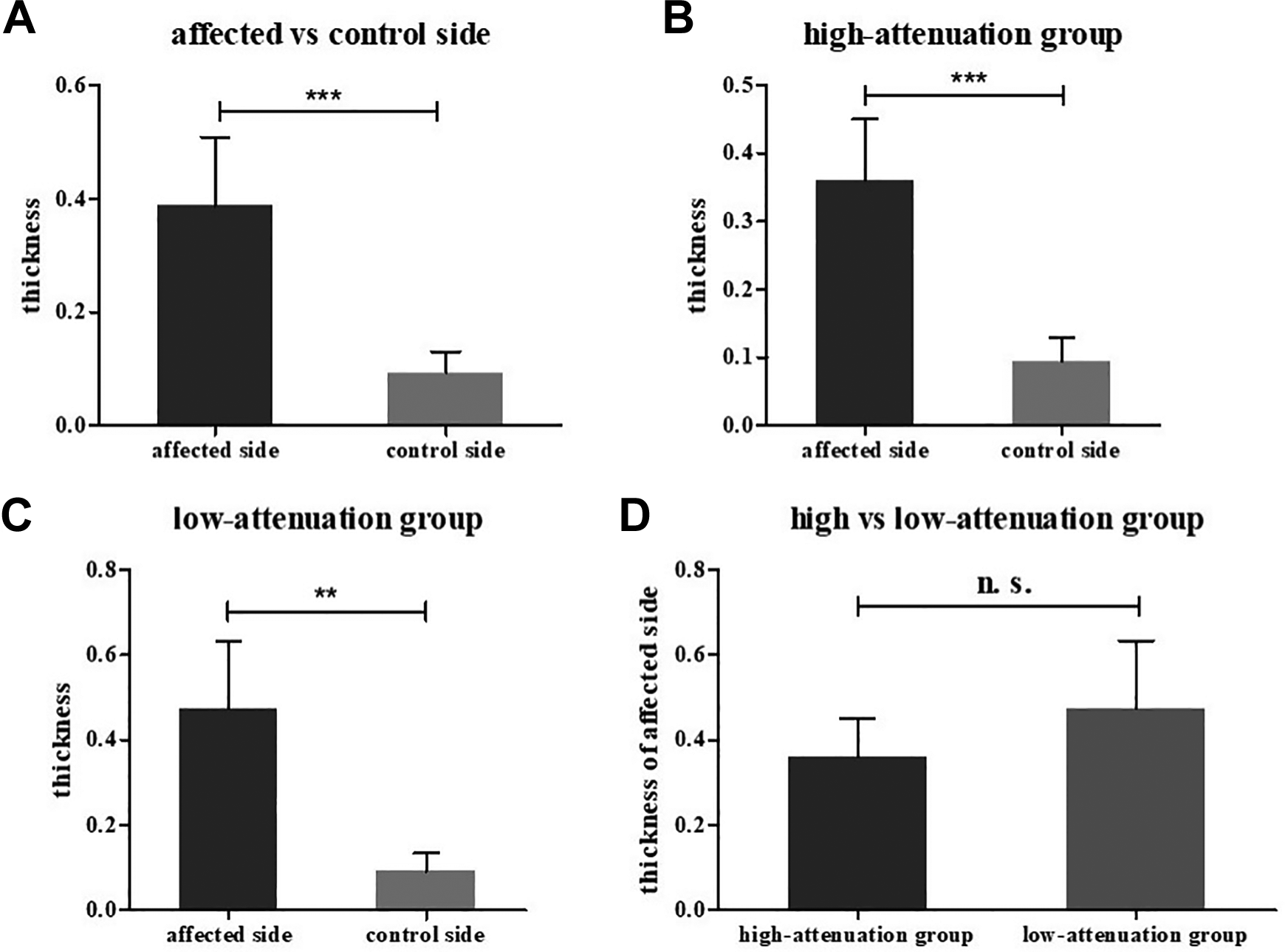
Comparison of bone thickness before and after grouping 40 patients by computed tomography attenuation. A, Comparison of the affected and control sides in 40 patients without grouping. B, Comparison of the affected and control sides in the high-attenuation group. C, Comparison of the affected and control sides in the low-attenuation group. D, Comparison of the affected side between the high- and low-attenuation groups.
Discussion
Chronic rhinosinusitis may cause submucosal bony changes, which has been confirmed by many previous studies.10-12 Computed tomography has obvious advantages in displaying mucosal and bony changes. It has been used as the most conventional method for evaluating CRS and bony changes. The attenuation of the CT value may be used to quantify the process of bone remodeling and could be used as an objective marker. At present, there have been few evaluations of unilaterally affected sinuses,17,19,20 and each sinus has a different anatomical structure and thus needs to be evaluated separately. In addition, invasion of the surrounding area has not attracted much attention in the past, so this study performed an assessment by the LIAT method.
Location of CMS With Osteitis
The range for evaluating bone remodeling in CRS is wide, involving 10 paranasal sinuses and nasal-related structures. Previous studies13-15,17-19 on integral and local assessments of CRS have always included the maxillary sinus. This study focused on the evaluation of the unilateral maxillary sinus for a comparative analysis. Through our research, we found that in CMS with osteitis, lesions occurred in locations including the posterior external wall, the medial wall, the anterior wall, the superior wall, and other sinus walls. Odontogenic factors are involved in the inferior wall, 20 which are not discussed in this study. The proportion of single or multiple cases of invasion of the posterior external wall of the maxillary sinus was the highest (88.9%), which has been reported in previous studies. Lesions also occurred in other locations, but there have been few related previous studies.
Osteitis occurring in the posterior external wall of the maxillary sinus is adjacent to fat and is unlikely to cause symptoms. Osteitis occurring in the superior wall (inferior orbital wall) can easily involve the infraorbital canals, infraorbital nerves, and blood vessels; in this case, osteitis can also easily protrude into the orbit across the sinus wall and compress the extraocular muscles and thus merits greater attention. Osteitis occurring in the medial wall may affect internal maxillary sinus drainage and cause nasolacrimal duct obstruction. Osteitis occurring in the anterior wall can cause facial bulging and affect the appearance of the face. It should be noted that osteitis in a single sinus wall is relatively rare and occurs in multiple sinus walls in most cases. In summary, osteitis may occur in any wall of the maxillary sinus, and comprehensive imaging evaluations should be performed.
Region of CMS With Osteitis Involvement
In this study, we found that osteitis in CMS may spread along the sinus wall and even cross the sutures and invade adjacent bone, but there have been few related previous reports. In our study, the sites of invasion included the zygomatic bone, sphenoid bone (pterygoid process), palatine bone, and nasal bone. The proportion of single or multiple cases involving the zygomatic bone was the highest (40.0%), followed by that of cases involving the sphenoid bone and palatine bone; the proportion of cases involving the nasal bone was the lowest. Sutures between adjacent bone are blocked by a double periosteal layer, which is a natural physical barrier. Thus, it is unclear how osteitis broke through this barrier to achieve cross-suture invasion. According to previous studies, the periosteum may be destroyed by inflammatory factors, and whether this finding could be explained by biomembrane theory7,21 or gene microarray analysis 22 is worthy of further investigation.
Computed Tomography Attenuation Assessment of CMS With Osteitis
Some clinical studies17,23 and animal experiments 24 have suggested that the CT value could be used to evaluate bony changes. The HU is used to represent the attenuation coefficient measured on CT reconstruction. 25 Studies 17 based on the human ethmoid sinus 17 and rabbit maxillary sinus 24 have both indicated that compared with the normal side, the side with osteitis showed a significantly increased CT value. However, the ethmoid sinus is thin, and accurate measurement of the CT value is difficult. The posterior external wall of the maxillary sinus is a common site of osteitis, and it is also one of the 3 conventional measurement sites proposed by Kim et al. 14 From an anatomical point of view, the thickness variation in the posterior external wall is the most stable and minimal among that of all sinus walls, which makes it an ideal measurement site. Therefore, we evaluated the bone remodeling of the posterior external wall of the maxillary sinus.
Osteitis has been previously reported to feature high attenuation.17-18,23 In our research, among the 40 patients with osteitis in the posterior external wall of the maxillary sinus, 75.0% showed high attenuation (≥500 HU). However, we also found some patients (25.0%) with low attenuation (<500 HU). According to previous studies,10,11 we speculate that CMS may disrupt the normal bone balance and cause bony changes in the sinus. The disease is caused by inflammation of the sinus mucosa and remodeling of the submucosal bone. Animal experiments and pathological results of clinical cases26,27 have confirmed that the pathological mechanism may be that the mucosa diffuses into the bone through the Haversian canal, and a dynamic process of osteoclastic and osteogenic reactions occurs, leading to increased or decreased CT attenuation. On the basis of histomathological analysis, when the osteoclastic reaction occurs, the bone tissue reduces, exhibiting low CT attenuation. When the osteogenesis occurs, bone tissue increases, exhibiting high CT attenuation. When the osteogenesis and osteoclastic reaction exist at the same time, it may cause uneven bone tissue density, resulting in uneven CT attenuation.
A more bizarre finding in the low-attenuation group was the formation of new bone marrow cavities in 6 (15%) cases. Therefore, we further speculated on the possible causes of the formation of new bone marrow cavities. Osteitis could enter a quiescent period, and bone remodeling could occur. The normal wall, consisting of a thin and single bone cortex, could evolve into an abnormal wall similar to long bone, composed of cortical and cancellous bone. Regions of low attenuation could actually be marrow cavities composed of cancellous bone and could be called remodeling marrow cavities. Whether the condition of osteitis tends to stabilize after entering a quiescent period and the corresponding impact on prognosis are still unknown. In summary, the CT value could reflect changes in the bone remodeling in patients with CMS, but whether it is positively correlated with osteitis remains to be confirmed by further studies.
Bone Thickness in CMS With Osteitis
Assessment of the bone thickness is a routine way to evaluate bone remodeling in CRS. The severity of osteitis is usually evaluated based on the increase in bone thickness. In this study, there was a significant difference in the bone thickness between the affected and control sides, which confirms this trend. In addition, we compared the thickness on the affected side between the high- and low-attenuation groups and compared the bone thickness between the affected and control sides in both the high- and low-attenuation groups. The results indicated that there was a significant difference in the bone thickness between the affected and control sides in both the high- and low-attenuation groups (high-attenuation group: P < .001; low-attenuation group: P < .01). However, there was no significant difference in the thickness on the affected side between the high- and low-attenuation groups (P >.05). These findings suggest that the increase in bone thickness is an important reference index for osteitis and that the thickness was positively correlated with the severity of CMS with osteitis. Previous studies have also reported similar findings. However, the change in CT attenuation may have no direct correlation with the thickness of the diseased bone.
There are still some limitations to this study. First, the sample size was small, and further verification in larger samples is needed. Second, although some special signs have been found (such as low attenuation and cross-suture invasion), the pathogenesis is still unclear and needs further research. Additionally, future studies need to include a pathological control and further examine the clinical symptoms and course of the disease.
Conclusion
Multislice helical computed tomography is the preferred method for the noninvasive assessment of CRS because it can provide details of the mucosa and bony anatomical changes. It is the most useful alternative to minimally invasive treatment. In addition to morphological changes, current CT evaluation methods mainly focus on measurement of the bone thickness and changes in attenuation caused by CRS. In patients with CMS with osteitis, the sinus bone on the affected side has a different morphology and different quantitative values than that on the normal side, which could be evaluated through the “LIAT” method. In the past, bony changes in CRS were considered to be positively correlated with bone thickness and attenuation. However, bone remodeling caused by CRS is supposed to be dynamic, so bony changes are not static, and the assessment and quantification of morphological changes on CT could be used to reflect the characteristics of bony changes in patients with CRS with osteitis. Such radiological evidence of bony changes may elucidate the propagation of CRS and provide clinicians with more information to lay a foundation for revealing the pathogenesis in the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by the National Natural Science Foundation of China (contract grant numbers 61931013, 61527807, and 62041103) the Beijing Scholars Program (contract grant number [2015] 160 [to Zhenchang Wang]), and Nanjing Medical Science and Technique Development Foundation (contract grant number QRX17207 [to Zigang Che]).