
Abstract
Testing for coronavirus disease 2019 is critical in controlling the pandemic all over the world. Diagnosis of severe acute respiratory syndrome coronavirus-2 infection is based on real-time polymerase chain reaction performed on nasopharyngeal swab. If not adequately performed, the viral specimen collection can be painful and lead to complications. We present a complication occurred during a nasopharyngeal swab collection performed in a noncooperative patient where the plastic shaft of the swab fractured during the procedure, resulting in swab tip retention deep into the nasal cavity. The foreign body was found endoscopically, stuck between the nasal septum and the superior turbinate tail at the upper level of the left choana and removed under general anesthesia in a negative pressure operating room with the health care personnel wearing personal protective equipment. Unpleasant complications like the one described can happen when the swab is collected without the necessary knowledge of nasal anatomy or conducted inappropriately, especially in noncooperative patients. Moreover, the design of currently used viral swabs may expose to accidental rupture, with risk of foreign body retention in the nasal cavities. In such cases, diagnosis and treatment are endoscopy-guided procedures performed in an adequate setting to minimize the risk of spreading of the pandemic.
Introduction
In Italy, from the beginning of pandemic (February 2020) to December 8, 2020, there have been 1 728 878 confirmed cases of coronavirus disease 2019 (COVID-19) with 60 078 deaths. Up to now, 23 125 664 severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) tests have been performed since the pandemic began, with a progressive increase during the second “wave” to 180 000 to 280 000 tests performed daily. 1 Diagnostic testing for COVID-19 is critical in controlling the pandemic all over the world, since it allows better control of the outbreak, containment, effective isolation of positive cases, and contact tracing. 2 Centers for Disease Control and Prevention guidelines have recommended that diagnostic swab tests should be performed in specific areas of the respiratory tract, with the nasopharynx and oropharynx as preferred sites. 3 A nasopharyngeal swab (NPS) can be performed simply by a healthcare provider adequately trained about the anatomy of nasal cavities: it has few contraindications and can easily be rolled out on a large scale. 4 However, if not adequately performed or conducted in noncompliant patients, this test can be painful and potentially dangerous for the patients. 5
We here describe a complication occurred during NPS collection performed in an uncooperative patient where the plastic shaft of the swab fractured during the testing procedure, resulting in swab tip retention deep into the nasal cavity. Informed consent for patient information and images to be published was provided by the legally authorized patient’s representative.
Case Report
A 37-year-old noncompliant male with Down syndrome presented to the emergency department (ED) after an attempt of COVID-19 testing at his day care facility performed because of a close contact with a confirmed case. During the procedure, a sudden head movement led to the engagement of swab tip break point mechanism while the NPS was still in the left nasal cavity resulting in swab tip retention deep into the nasal cavity, completely out of direct vision. A second NPS for COVID-19 testing was collected at the ED (with NPS inserted through the right nasal cavity), and a head lateral plain radiograph with no evidence of retained foreign body; a subsequent bedside otorhinolaryngological examination by means of a single-use flexible 3-mm endoscope (Ambu aScope 4 RhinoLaryngo Slim device) and a high-definition (HD) monitor (Ambu aView) showed the tip of the swab retained in the left nasal cavity, stuck between the nasal septum (NS) and the superior turbinate tail at the upper level of the left choana (Figure 1). The foreign body location could not be easily reached, because of a severe deviation of the NS and a concomitant hypertrophy of the inferior and middle turbinate.
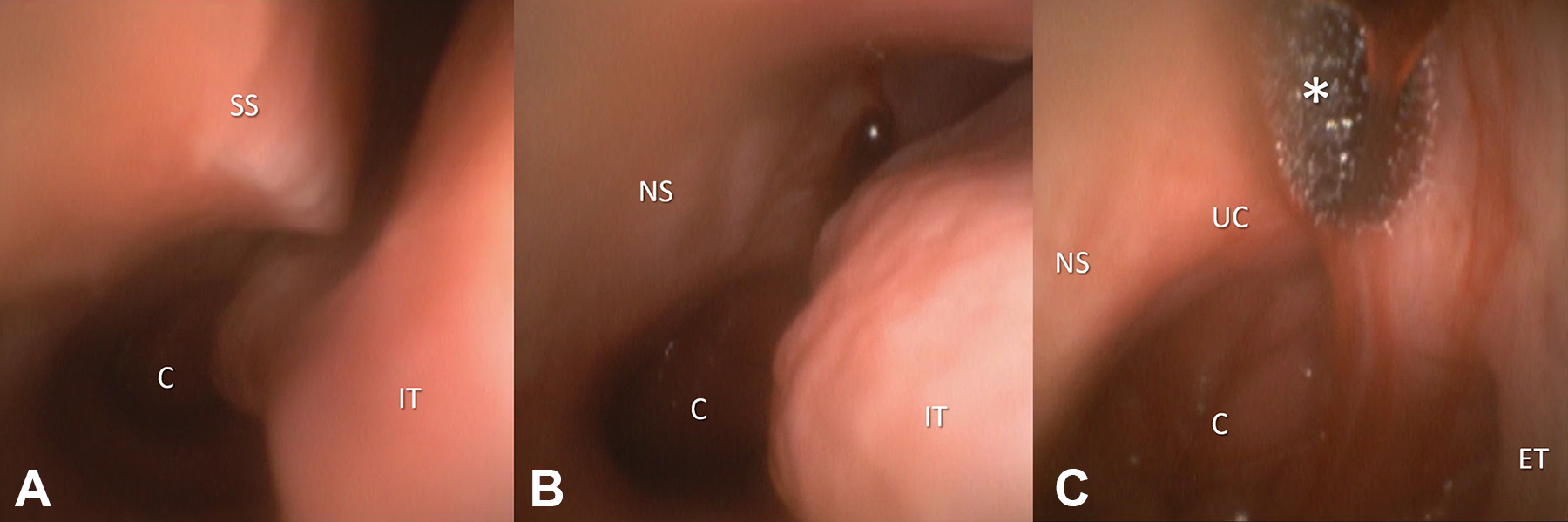
Flexible nasal endoscopy: (A and B) the posterior part of the left nasal cavity and the choana (C) were difficult to reach because of a septal spur (SS) and the hypertrophic tail of the inferior turbinate (IT); (C) a foreign body (asterisk), the tip of a nasopharyngeal swab, soaked in a blood clot, was stuck between the nasal septum (NS) and the superior turbinate tail at the upper level of the left choana (UC). The Eustachian tube ostium (ET) was visible on the right side of the picture.
As the NPS performed at the ED resulted positive to COVID-19, the patient was transferred to a COVID-19 ward, and an operating room (OR) equipped for the management of COVID-19 patients was set up. Due to the deep location of the foreign body and narrow nasal cavity due to the concomitant septal deviation, the risk of displacement during removal maneuver and the noncompliant attitude of the patient, the procedure was performed in a negative pressure OR, with all the health care personnel wearing personal protective equipment, under general anesthesia with laryngeal mask. After topical vasoconstriction of the nasal mucosa with xylometazoline hydrochloride, the foreign body was removed by means of a single-use 5-mm flexible bronchoscope (aScope 4 Broncho Regular), a HD monitor (Ambu aView) and flexible endoscopy forceps inserted through the 2.2-mm operative channel of the bronchoscope. The tip of the nasal swab was grasped using flexible endoscopy forceps (Figure 2) and retrieved from the left nasal cavity (Video 1); the plastic shaft was hidden in the superior meatus and angled with an upper concavity (Figure 2), with no chance of detection during the diagnostic flexible video endoscopy. No further foreign bodies were detected in the nasal cavities. The patient was kept under observation for a few hours without occurrence of nasal bleeding or any other complication and then referred to a COVID-19 ward.
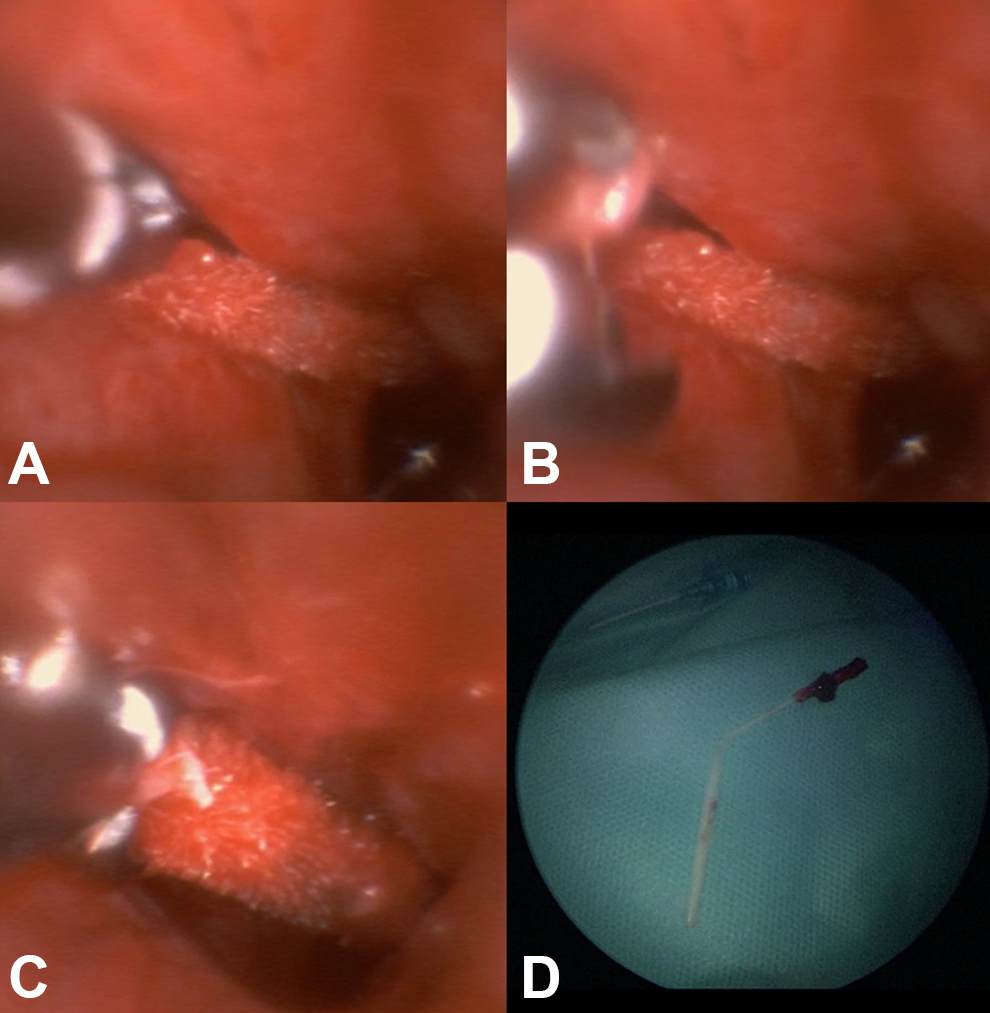
A, The tip of the nasal swab was reached by means of a 5-mm disposable video bronchoscope, (B) then grasped by flexible endoscopy forceps inserted through the operating channel, (C) and retrieved; (D) the foreign body after the retrieval. The plastic shaft was hidden in the superior meatus and angled with an upper concavity with no chance of detection during the diagnostic endoscopy.
Discussion
Nasopharyngeal swab fracture during COVID-19 testing with retention of (portion of) the swab into the nasal cavity have been reported in only few cases6,7; to our knowledge, this is the first case in which the tip of the swab was embedded in the upper choanal region. Many factors may predispose to this unpleasant condition, with possible risk of inhalation 8 or ingestion. 9
The increased availability and need of testing have boosted numbers and types of health care providers who conduct these tests in various settings, ranging from hospitals to drive-through test centers. In order to correctly and safely perform NPS, an adequate training about sampling procedures and familiarity with some concepts of nasal anatomy are mandatory for health care workers. 2 Education of health care personnel may be performed by means of educational sessions focused on nasal anatomy and sampling technique 10 or active training on 3D printed models. 11 The correct procedure for COVID-19 testing involves inserting a 15-cm long swab through the nostril, along the NS and parallel to the palate until the nasopharynx, and gently rotating the swab several time.2,12
The swabbing should then be repeated on the other side of the nose to make sure that enough material is collected. Challenges to providers include poor understanding of nasopharynx location relative to the nasal cavity, inability to pass the swab through either nostril, and subsequent patient and provider discomfort with COVID testing. These challenges are worsened in case of uncooperative patients, such as in the described case, with higher risk of complications. 9
In this case, the nasopharynx was very difficult to be accessed through the left nasal cavity due to a severe septal deviation, extending from the inferior to the middle meatus, and a concomitant hypertrophy of the inferior and middle turbinate; quite the opposite, the right nasal cavity was patent and free from any anatomical obstruction. The hypothetical dynamics of this complication can be summarized as follows: the NPS, introduced in the left nasal cavity, was pushed high up in the nasal cavity because of the impossibility to pass through the inferior meatus, and forced against the choanal wall, it broke in 2 parts and folded up, and was subsequently embedded in the superior meatus at the upper level of the choana. The painful NPS insertion in this narrow nasal cavity exacerbated the already noncooperative attitude of the patient. In such a case, a better familiarity with anterior rhinoscopy could lead to the choice of the more accessible nasal cavity to make the sampling procedure less discomfortable.
Another issue concerns the swabs. The types of NPS used to collect the specimens for COVID-19 testing may vary, ranging from plastic to aluminium shaft. 13 In our case, the shaft of the swab consisted of 2 components: a plastic swab, which incorporates a break point halfway down the shaft of the swab, and an open-celled foam tip to collect the specimen. The break point mechanism prevents contamination while transferring the shaft into the container. However, this feature makes the swab susceptible to fracture while still in the nasal cavity. This situation could arise in noncooperative patients, such as pediatric, neurologic, and/or syndromic patients, and in case of anatomical variations (eg, septal deviations and spurs). Unexpected head or limb movements can easily lead to the swab breaking and its subsequent retention in the nasal cavity, as illustrated in the present case. In our case, it was impossible to establish with certainty whether the rupture of the NPS was secondary to a defective kit or to excessive pressure exerted during sampling. The simplest way to avoid this complication is to utilize a product without a break point. Based on the information available from different sources,1,14 alternative products for viral sampling with no break point do exist. The use of alternative swabs may provide a useful alternative in patients at risk of experiencing premature breaking of the viral swab shaft in the nasal cavity. Moreover, the plastic NPS, which is not radiopaque, went undetected on radiographic evaluation, which revealed to be completely useless in this case. In patients with strong suspicion of non-radiopaque foreign body retention, endoscopic evaluation is recommended. In the COVID-19 era, close face-to-face proximity should be avoided and therefore a nasal video endoscopy should be carried out. 15 During the COVID-19 pandemic, the use of disposable endoscopic devices has been encouraged in many different fields, thanks to the potential to create a safer working environment for patients and for health care personnel. 16 In this case report, a single-use flexible video endoscope was used to detect the foreign body, while for its removal a single-use flexible video bronchoscope with operating channel helped the surgeons to reach the posterior region of the nasal cavity avoiding septal surgery and to shorten surgical time. General anesthesia allowed to bypass the noncooperative habit of the patient and to avoid an aerosol-generating procedure, reducing the risk of disease transmission to the health care staff.
In summary, testing for COVID-19 can lead to unpleasant complications when NPS is performed without the necessary knowledge of nasal anatomy and when conducted inappropriately, especially in noncooperative patients. The design of currently used viral swabs may expose patients and health care providers to accidental rupture, with risk of retention of a foreign body in the nasal cavities and subsequent inhalation or ingestion. In such cases, diagnosis and treatment are necessarily endoscopy-guided procedures performed in an adequate setting to minimize the risk of spreading of SARS-CoV-2 infection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.