
Abstract
The SARS-CoV-2 pandemic response utilizes nasopharyngeal swabbing as a prolific testing method for presence of viral RNA. The depth of the swab to the nasopharynx coupled with breakpoints along the shaft leads to a risk for foreign body retention. Here, we present a case of a nasopharyngeal swab that became a retained foreign body during routine swabbing to test for the SARS-CoV-2 virus. Bedside flexible fiberoptic endoscopy was performed and did not reveal a foreign body in the nasopharynx or larynx. Subsequent computed tomography (CT) scan demonstrated the radiopaque retained foreign body at the distal gastroesophageal junction. The patient remained asymptomatic and did not have any upper airway or gastrointestinal symptoms. This unique case demonstrates a potential risk associated with SARS-CoV-2 nasopharyngeal swab testing and highlights management strategies that serve the patient while adequately protecting health care providers. A standardized approach to evaluation optimally includes bedside flexible endoscopy with appropriate personal protective equipment, prompt airway evaluation if aspiration is suspected, and noncontrasted CT imaging if the known foreign body is not identified via other modalities.
Keywords
Introduction
During the SARS-CoV-2 pandemic, disease-specific testing became highly prevalent. 1 A nasopharyngeal (NP) swab of the upper respiratory tract is recommended to detect viral RNA from SARS-CoV-2.1,2 Rare hazards of NP swabbing may include the risk of a premature “breakpoint” in the swabs architecture, injury to the NP mucosa, and epistaxis. 3 Here, we report a case of a broken NP swab initially thought to be impacted in the nasal airway but subsequently detected on imaging above the gastroesophageal junction.
Case Report
This study was exempt from the Vanderbilt International Review Board. A 46-year-old female presented to the emergency department (ED) for management of traumatic injuries secondary to being struck by a motor vehicle. Upon arrival to the ED, the patient underwent routine NP SARS-CoV-2 testing. During testing, she became acutely combative and the NP swab was fractured along the shaft. It was determined that approximately 4 cm of the distal 15 cm swab (Figure 1) was retained. Repeat NP swab was performed without incident; the patient tested negative for SARS-CoV-2. Emergency department staff could not visualize the foreign body in the nares, mouth, or outside the body. The on-call otolaryngology physician performed flexible fiberoptic endoscopy to evaluate the nasopharynx and larynx and no foreign body was identified. A maxillofacial computed tomography (CT) scan was unrevealing; however, a noncontrasted chest CT revealed a 3.6 cm linear radiodensity above the gastroesophageal junction (Figure 2). As the patient was asymptomatic, the decision was made to allow the swallowed foreign body to pass via the gastrointestinal tract without intervention. No gastrointestinal symptoms from the foreign body were reported during admission.
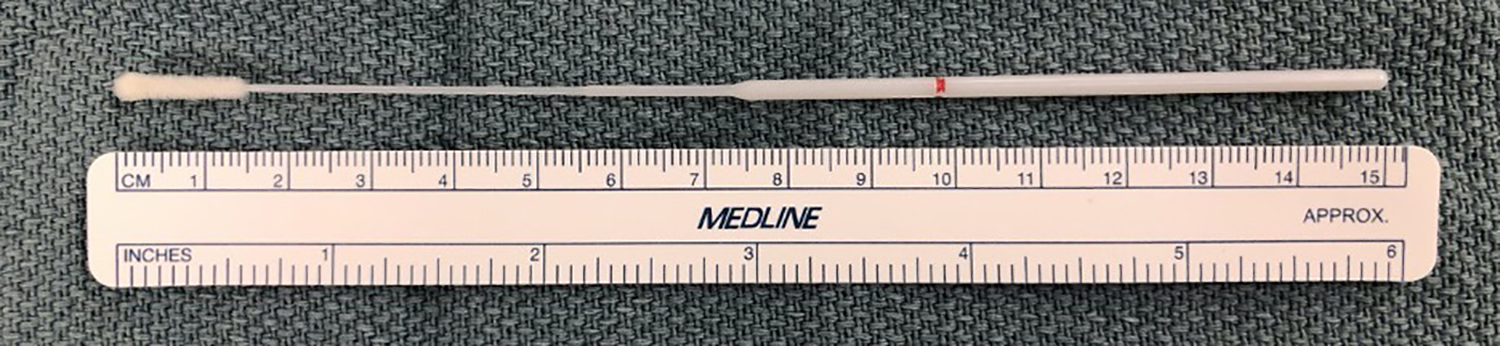
This is an image showing dimensions of a sample nasopharyngeal swab.
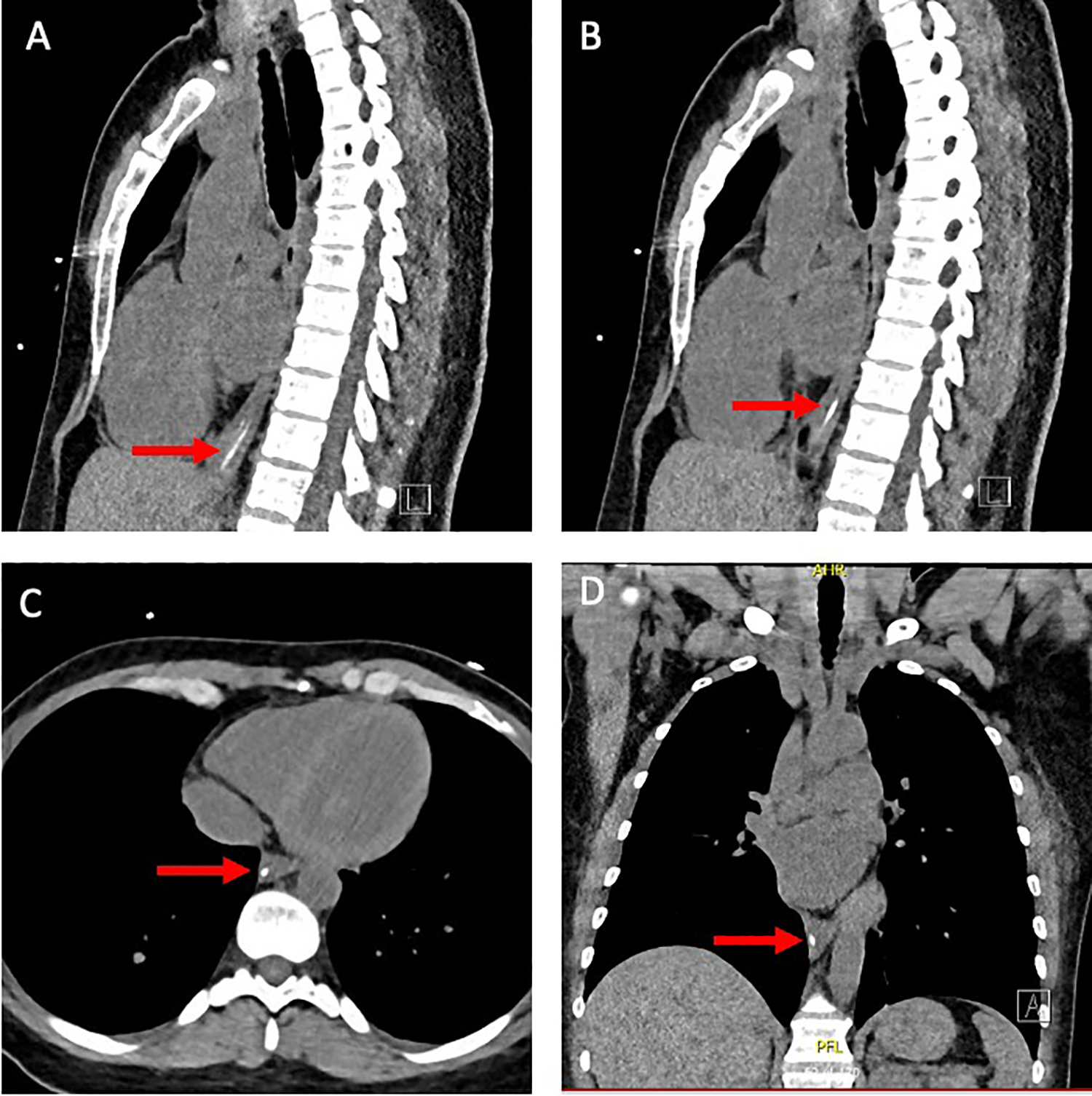
Computed tomography (CT) images showing the foreign body located above the gastroesophageal junction. (A) Sagittal CT showing shaft of the nasopharyngeal swab; (B) Sagittal CT showing head of swab foreign body; (C) axial CT showing foreign body; (D) coronal CT showing foreign body above the gastroesophageal junction.
Discussion
Widespread testing for SARS-CoV-2 is part of the strategy to contain the virus, with polymerase chain reaction detection of viral RNA from a NP swab being the primary modality. The presented case is a novel contribution to a handful of recent reports of broken SARS-CoV-2 swabs as retained foreign bodies in the respiratory or digestive tracts.3-5 In 2 cases, the swab remained lodged in the nares.3,4 This required instrumentation of the nasal airway at bedside for removal, including rigid nasal endoscopy. Only one other case reported an ingested swab. Nasopharyngoscopy failed to identify the foreign body in that case, and no imaging was performed. It was identified in the stomach via esophagoscopy performed under general endotracheal anesthesia. 5
This case raises important concerns regarding aerosol-generating procedures (AGPs), including nasal endoscopy in patients with unknown COVID-19 status. Variability exists in addressing AGPs and minimizing risks to health care workers and patients. Additionally, retained swabs represent a potential aspiration risk, particularly in altered or pediatric patients, often necessitating further evaluation and/or intervention. The wide variance in approaches suggests the need for a standardized approach to a lost NP SARS-CoV-2 swab. The authors advocate for initial examination with flexible fiberoptic nasopharyngoscopy performed at bedside, with thoughtful attention to the risks of potential risk with AGPs. If safe to do so, immediate repeat SARS-CoV-2 testing should be performed. Evaluation should be performed with appropriate personal protective equipment (PPE) including face shield, gown, gloves, and N95 or higher respirator if COVID-19 status unknown. 1 Should direct visualization fail to identify a foreign body, noncontrasted CT imaging of the aerodigestive track is preferable to a more invasive operative approach if the patient is deemed medically stable. This also minimizes the risk of SARS-CoV-2 exposure to other individuals that exists with a procedure requiring anesthesia and intubation. However, if an airway foreign body is suspected, prompt operative intervention with direct laryngoscopy and bronchoscopy should be performed, again with appropriate precautions and PPE. The decision to remove a digestive tract foreign body or allow it to pass naturally is a matter of active discussion. In the presented asymptomatic patient with multiple traumatic injuries, allowing the swab to pass the gastrointestinal tract naturally was deemed the safest approach.
This unique case demonstrates a potential risk associated with SARS-CoV-2 NP swab testing and highlights management strategies that serve the patient while adequately protecting health care providers. We advocate for a standardized approach to evaluation including bedside flexible endoscopy with appropriate PPE, prompt airway evaluation if aspiration is suspected, and noncontrasted CT imaging if the known foreign body is not identified via other modalities.
Footnotes
Authors’ Note
Madelyn Stevens contributed to conception and design, data acquisition, writing and revising, final approval. George Lin contributed to data acquisition, writing, final approval; Sarah Tittman contributed to conception and design, writing and revising, final approval; Kevin Motz contributed to design, critically revising for intellectual content, final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.