
Abstract
Purpose
Smoking is not only one of the main risk factors for the development of most malignant and numerous benign ENT tumours but also has an important influence on therapy and prognosis. Even quitting smoking at the time of diagnosis significantly reduces mortality. Patients have a particularly strong desire to stop smoking when they are diagnosed. The present study investigated to what extent patients were aware of the relationships between smoking and the development and prognosis of tumours and how much information and smoking cessation support they were offered by physicians.
Methods
A total of 194 patients (74.7% male, 62.0 ±10.6 a) with malignant primary ENT tumours, pre-cancerous tumours, Reinke’s oedema and salivary gland tumours were interviewed.
Results
22.7% were nonsmokers, 49.5% were cigarette smokers and 27.8% were ex-smokers. A total of 57.0% of the smokers said they would have quit before the onset of the disease if they had known about the association. Forty-one percent did not receive information about the association between smoking and the development of their disease, while 45.5% did not receive information about the relationship with their prognosis. The provision of information lasted less than 5 min for 40.4% of the patients and more than 10 min for only 13.5%. In total, 50.7% of the patients were directly requested not to smoke. A total of 7.7% received offers of smoking cessation support from otolaryngologists and 18.2% received such offers from family physicians.
Conclusions
There is a pronounced need for improvements in the provision of medical information about the health risks associated with smoking and offers to support patient efforts to stop smoking. In particular, the appointment during which the diagnosis is communicated to the patient should be considered a ‘teachable moment’ that can lead to smoking cessation.
Introduction
Tobacco is a legal drug that kills many of its users when used exactly according to the manufacturer’s instructions. 1 Tobacco kills more people than tuberculosis, HIV and malaria combined. 1 In addition, smoking is one of the biggest risk factors for cardiovascular disease, chronic respiratory disease, type 2 diabetes and cancers, and it also contributes to family poverty cycles, as often a significant portion of income is used to purchase tobacco. 1,2
According to the World Health Organization (WHO), approximately 8 million people worldwide died from tobacco-related diseases in 2017. 3 Fortunately, the number of smokers is slowly decreasing: while the prevalence in Europe was still 34.2% in 2000, it was only 27.4% in 2015. 3 Even more promisingly, the proportion of young people who smoke in Germany fell by nearly 80% to 6.6% from 2001 to 2018. 2 However, due to the time lag before the onset of a disease, it is to be expected that the number of tobacco-related annual deaths will continue to increase in the coming years. 3
Smoking is one of the most important risk factors for the development of most malignant ENT tumours in the oral cavity, epipharynx, oropharynx, hypopharynx and larynx, as well as benign tumours such as Whartin’s tumours and Reinke’s oedema. 4 –9 Furthermore, smoking affects therapy and prognosis. 10 Thus, studies showed a significant reduction in mortality even when smoking was only stopped at the time of diagnosis of a head and neck malignancy. 11 The cessation of nicotine use as late as in the post-diagnosis period was also associated with improved outcomes of cancer treatment: Warren described a median reduction in overall mortality of 45%. 10
Screening for cancer and the communication of a cancer diagnosis represent ‘teachable moments’. 12 In such moments, there is an increased desire and willingness on the part of the patient to initiate changes. It is, therefore, the optimal time to recommend lifestyle changes, such as nicotine use cessation. 12 The present monocentric questionnaire study was designed to investigate how well this ‘teachable moment’ is used in the context of providing medical information and offering support in the form of nicotine withdrawal therapy. In addition, the knowledge of patients with ENT tumours about smoking as a risk factor for the development and prognosis of their disease was surveyed.
Materials and methods
Study description
The study was conducted in the ENT department of a German secondary care hospital. From 01.10.2018 to 30.09.2020, patients diagnosed with leukoplakia or a malignancy (in the epi-, oro-, hypopharynx and oral cavity), Reinke’s oedema or a salivary gland tumour were recruited for the present study. Patients were given a comprehensive printed questionnaire with closed questions (single and multiple choice, plus matrix questions) at the beginning of their inpatient stay, which they had to hand in before discharge. Only patients who provided signed informed consent were included. Patients with metastases from non-ENT tumours and patients with repeated hospitalizations were excluded. The questionnaire has already been investigated and successfully used in a comparable study in urological tumours and was only rewritten to ENT tumours. 13 The questionnaire asked patients about their current and past smoking habits, knowledge of the relationship between smoking and ENT tumour development and prognosis. The questionnaire also included the same questions about lung and urinary bladder cancer to make comparisons regarding knowledge. Furthermore, questions on the duration and quality of medical education about the risks associated with nicotine use were included.
Statistics
The statistical analysis and graph generation were carried out in Microsoft Excel 2016 for Windows (Microsoft Corporation), SPSS Statistics 24 software (IBM Corporation, Armonk/USA) and EvaSys v8.0 (evasys GmbH, Lüneburg, Germany).
Results
Study participants
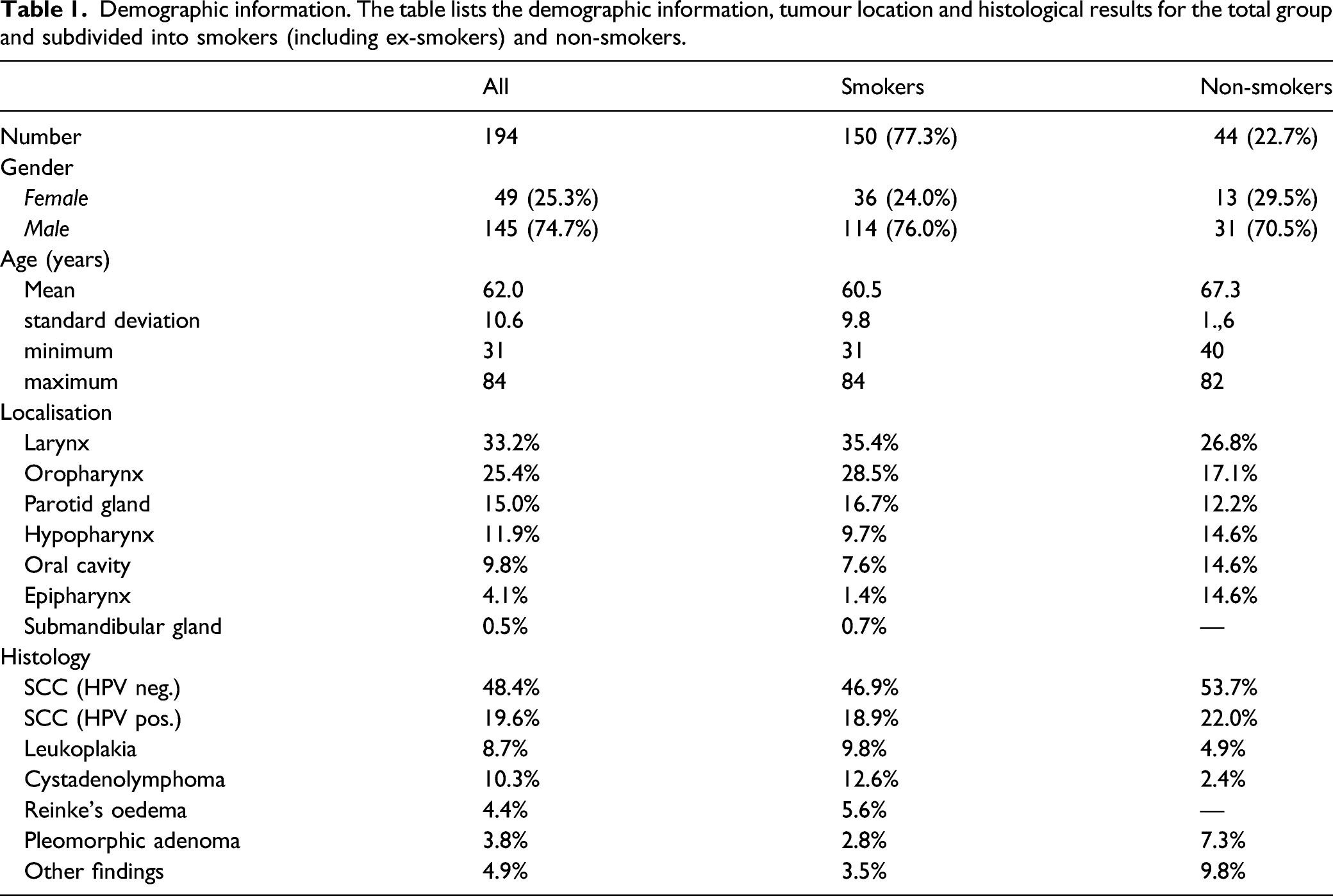
Demographic information. The table lists the demographic information, tumour location and histological results for the total group and subdivided into smokers (including ex-smokers) and non-smokers.
General smoking behaviour
22.7% of the patients described themselves as non-smokers, 49.5% as cigarette smokers and 27.8% as ex-cigarette smokers. A total of 22.5% of the smokers stated that they had stopped smoking due to their disease, and 23.5% had reduced their smoking. A total of 22.5% of the smokers intended to quit smoking due to their current disease.
When asked if they would have quit smoking before the disease occurred if they had known about the connection, 57.0% of the smokers answered yes, while 43.0% answered no. Of the ex-smokers, 40.4% answered that they would have quit to avoid the disease, and 59.6% answered that they would not have quit to avoid the disease. Of the non-smokers, 66.7% answered that the prevention of secondary diseases was one of the main reasons they abstained from smoking.
Provision of medical information about smoking
Provision of medical information about smoking. The table shows the results of the questions for the collective of smokers and ex-smokers.
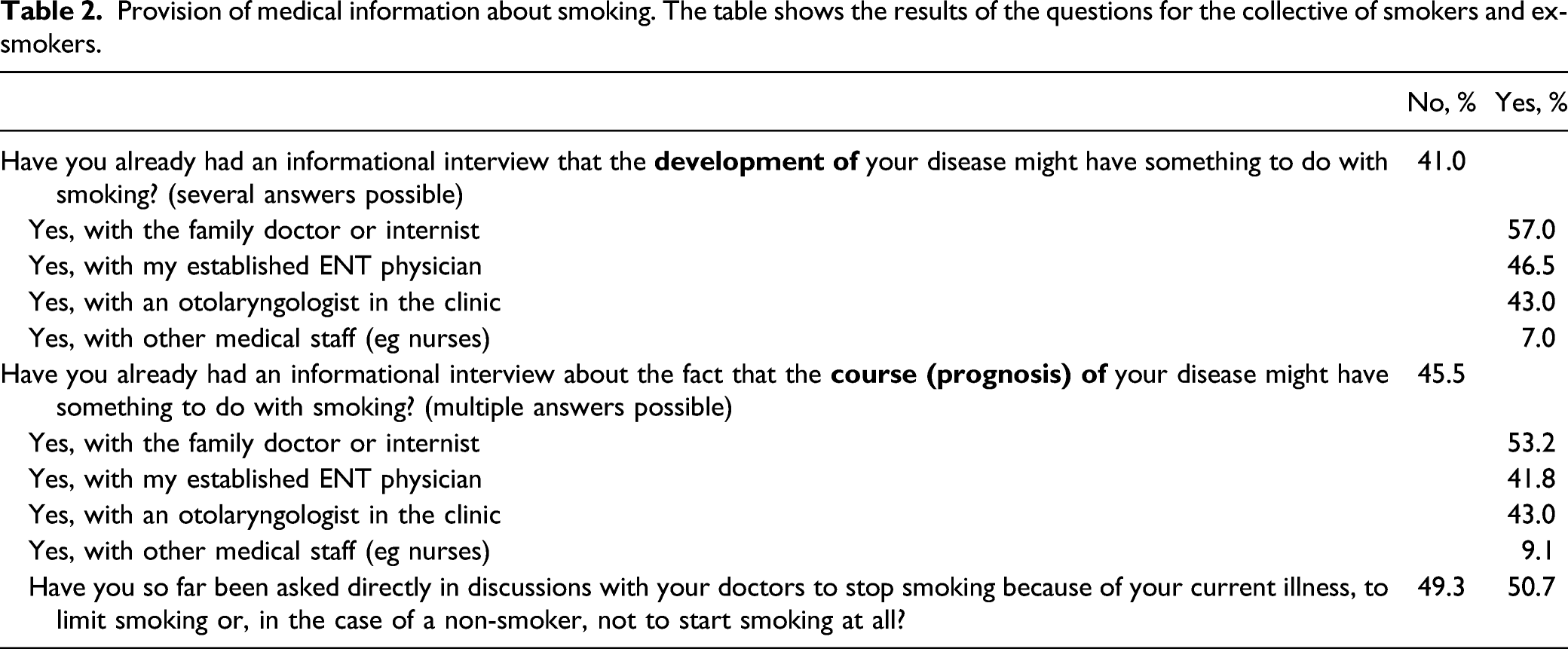
In total, 45.5% of the smoking patients reported that they did not receive information about the effect of smoking on the course (prognosis) of their disease (see Table 2). For those who did receive such information, 53.2% talked with their general practitioner, 43.0% talked with their attending ENT physician and/or clinician, and 10.1% talked with other medical staff members.
45.8% percent of the patients (50.7% of the smokers) received a direct request from doctors due to their current illness to stop smoking, limit their smoking or not to start smoking (see Table 2). A total of 56.7% of the smokers stated that they had not been offered any nicotine use cessation aids by their physicians (see Figure 1). Nicotine replacement options or a treatment plan were given to 7.7% of the smokers by ENT specialists and to 18.2% by general practitioners, and information leaflets were given to 12.5% by ENT specialists and to 20.2% by general practitioners (multiple answers were possible). Provision of medical information. The figure shows the results of the question: ‘Were you offered any smoking cessation aids by your treating physicians?’ (multiple answers possible; only smokers evaluated).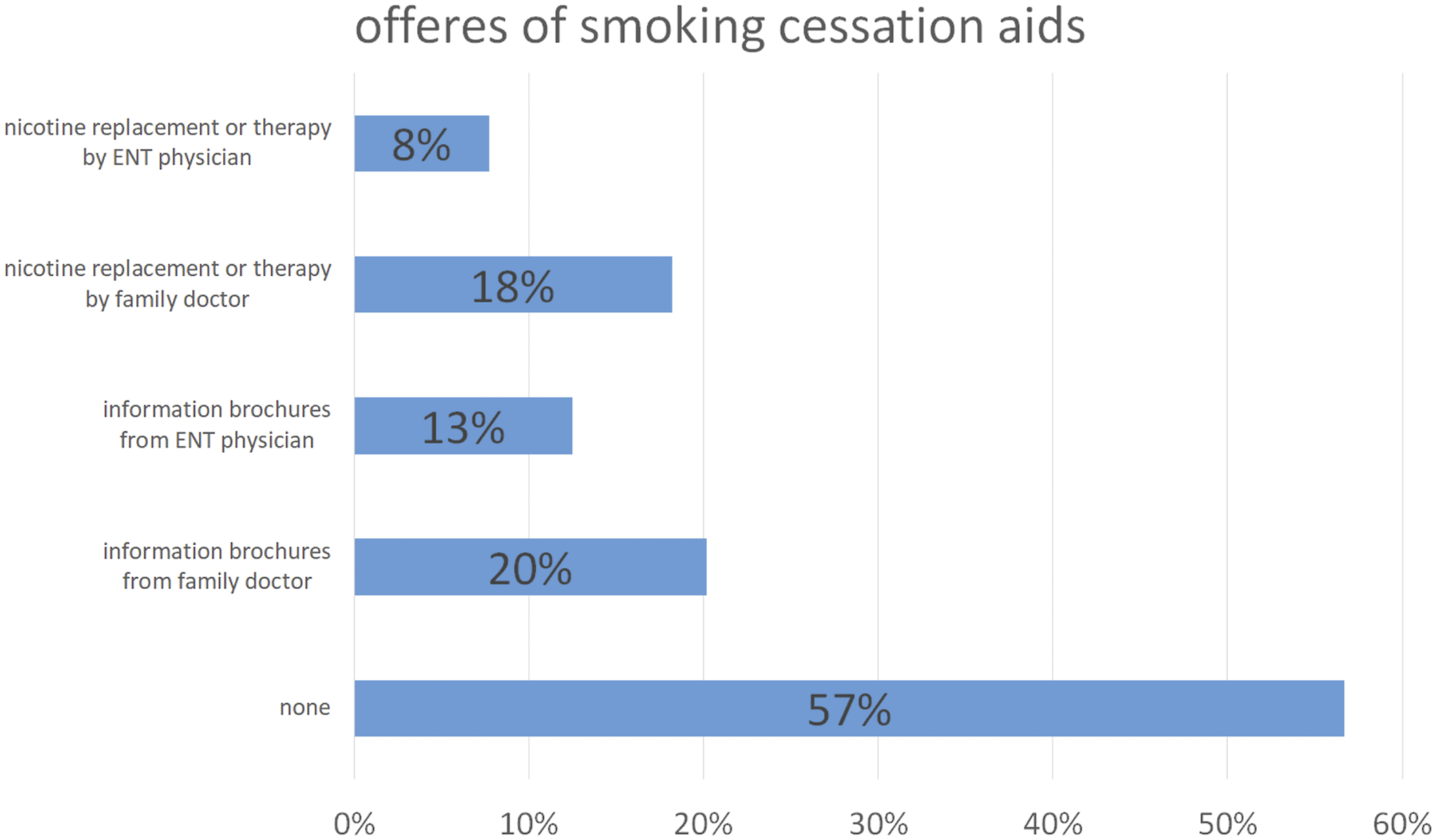
Of the smoking patients who received medical education about the relationship of smoking with their disease, 40.4% reported that the conversation was shorter than 5 minutes, 46.1% reported that it lasted between 5 and 10 minutes, and 13.5% reported that it lasted longer than 10 minutes (see Figure 2). Provision of medical information. The figure shows the results of the question: ‘How much time in total has been spent so far by the doctors treating you to inform you about the possible connection between smoking and your illnesses?’ (only smokers evaluated).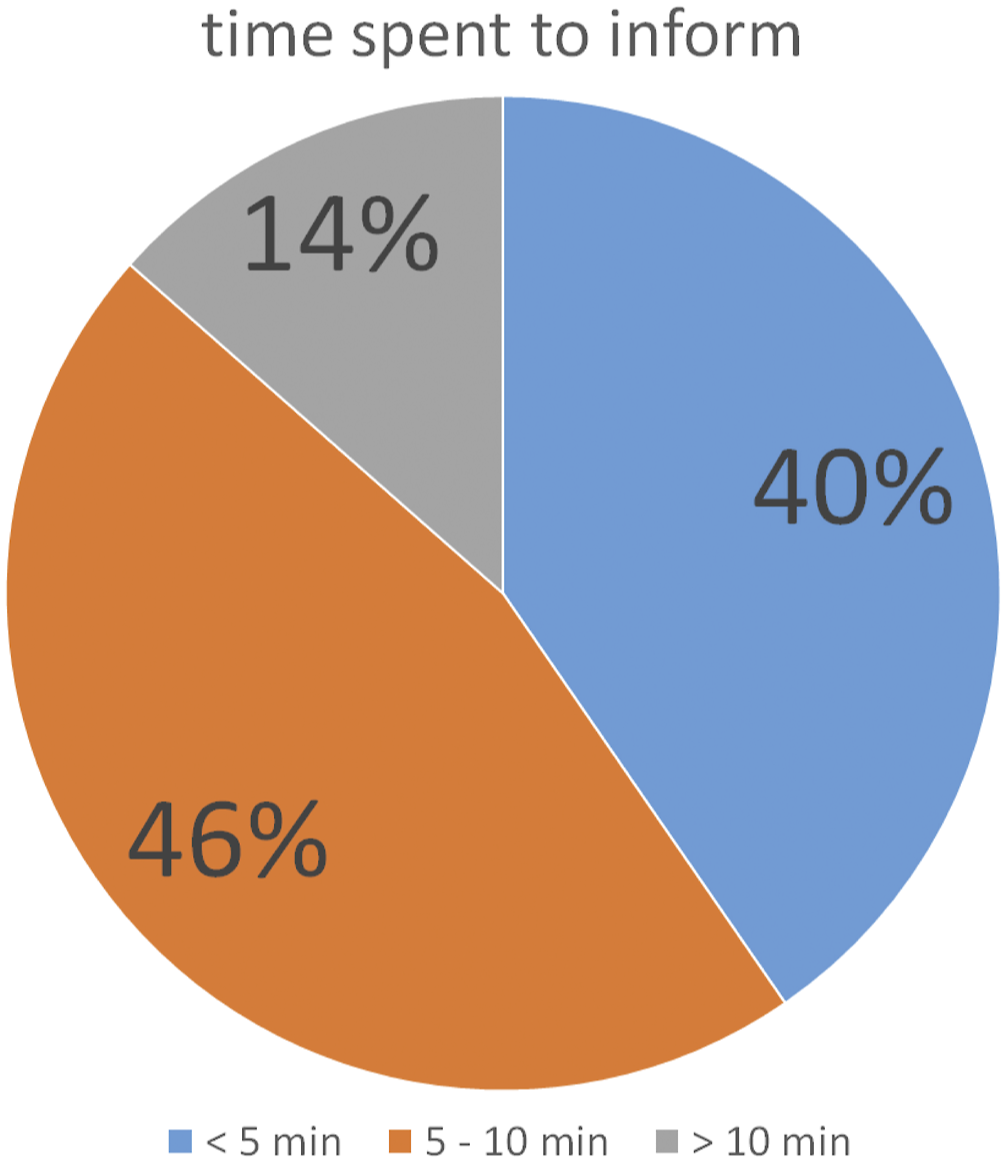
A total of 12.0% of the smoking patients felt that the education provided by the treating physicians was inadequate. A total of 19.5% rated the education provided by the media and public information system as inadequate, while 66.2% thought the information provided by the media and public information system was good. A total of 6.0% of the smokers thought that such information was not necessary because there was no connection between the disease and smoking (multiple answers possible).
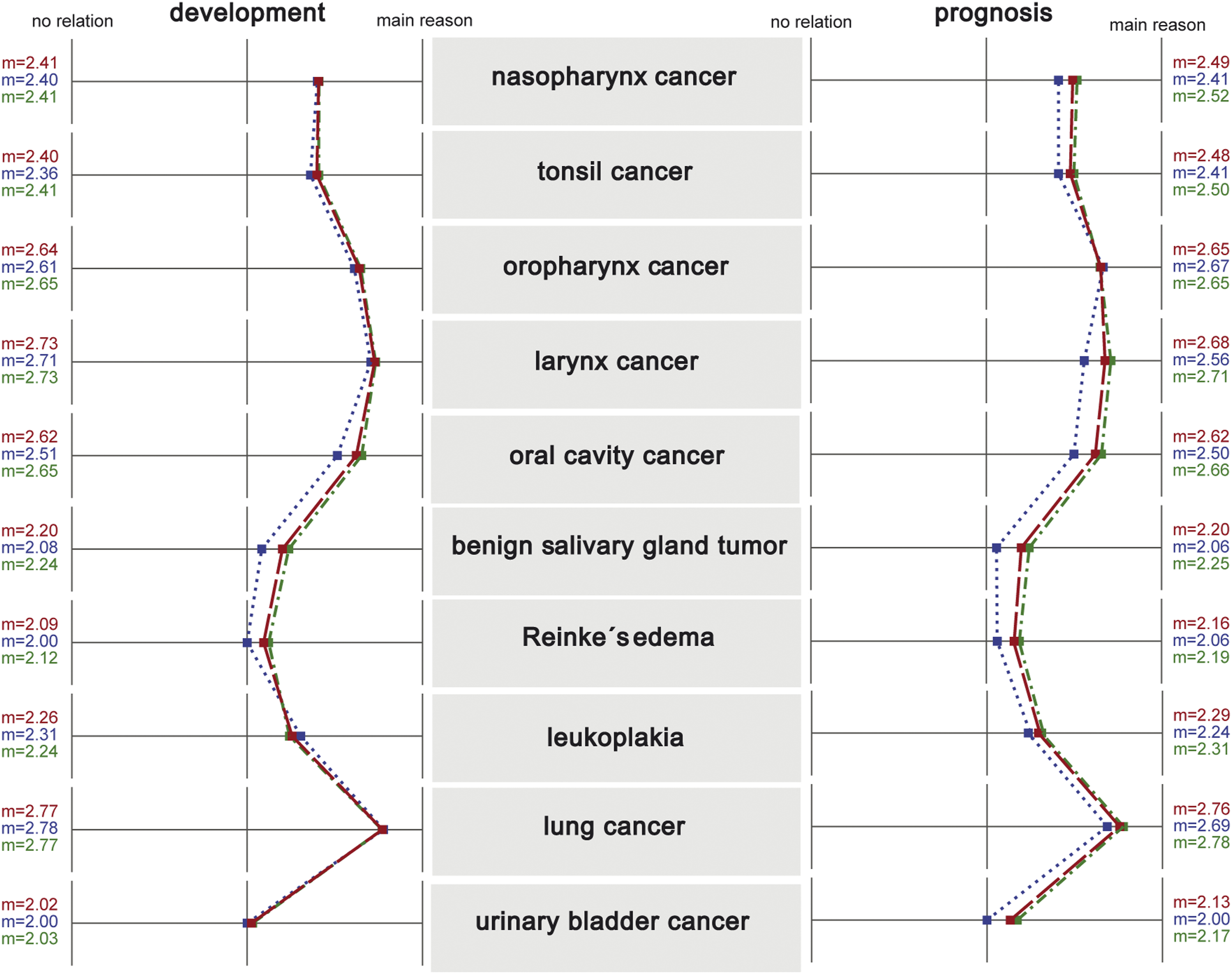
Smoking as a risk factor
In total, 24.8% of smokers and ex-smokers believed that the development of their disease was not related to smoking, and 20.9% of the patients (19.2% of the smokers) believed that continuing or starting to smoke would not affect their prognosis. The survey responses regarding the connection between the development and prognosis of ENT cancer are shown in Figure 3, subdivided for all subjects, the group of and the non-smokers in Figure 4. In the questionnaires, Reinke’s oedema was additionally described as ‘water accumulation in the vocal cords’ and leukoplakia as ‘whitish discolouration of the mucosa’. Smoking and the development of disease and disease prognosis. The graph shows the results of the survey on smoking as a risk factor for the development of diseases and disease prognosis of various ENT tumours. The bars show the distribution of the answers (1 = no relation, 2 = connection is discussed but not yet proven, 3 = main reason), above the absolute (n) and percentage frequency of answers. The black line shows the standard deviation (s) in each case, and the red line indicates the mean value (m). Smoking and the development of disease and disease prognosis. The graph shows the results of the survey on smoking as a risk factor for the development of diseases and disease prognosis of various ENT tumours, subdivided for all subjects (red line), the group of smokers (green line) and the non-smokers (blue line). (m = mean value)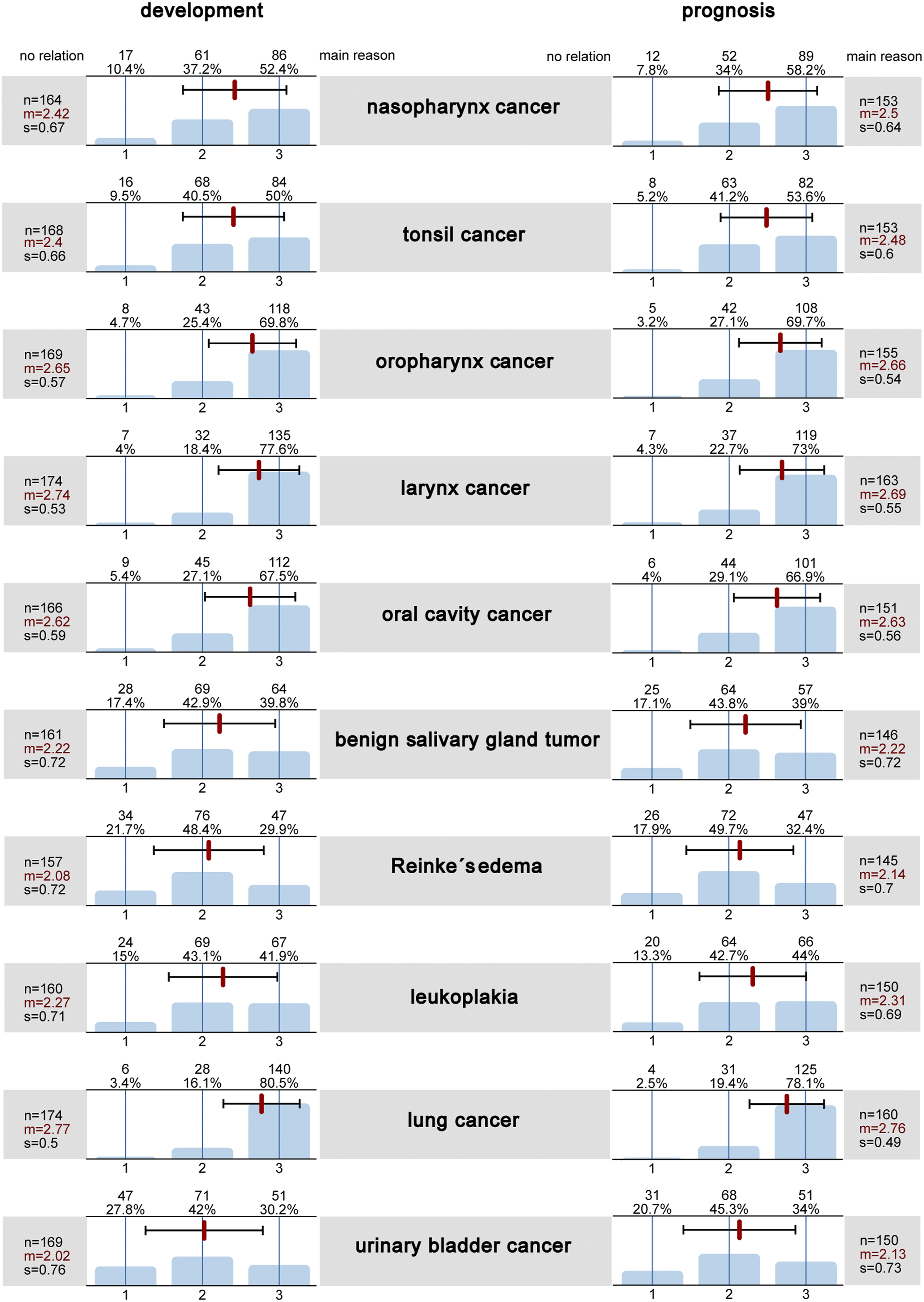
Discussion
Reducing tobacco consumption and creating a smoke-free society, defined as a smoking prevalence less than 5%, are the stated goals of the German Federal Ministry of Health and the WHO.
2
The latter has developed the MPOWER project for this purpose, which is a bundle of measures to be implemented by the individual member states
3
:
Through various measures, including multiple increases in the tobacco tax, an increase in the legal age for the purchasing of tobacco products to 18 years and the obligation to include picture-based warnings on packaging, the number of smokers in Germany has been significantly reduced since the turn of the millennium. In 2018, 18.5% of women and 24.2% of men smoked in Germany. 2 In the present study, the percentage of smokers was thus above average, with almost 50% of the patients classified as cigarette smokers and nearly 30% as ex-smokers. This high percentage of smokers is due to the selection of patients with ENT tumours, given that smoking is a major risk factor for the development of such tumours.5,6,7,8,9
Fortunately, most of the patients in the present study were aware of the connection between smoking and ENT cancer: only a quarter of the patients believed that smoking was not related to the development of their disease, and a fifth of them believed that it would not influence their prognosis. However, when asked about the different disease patterns, relevant differences emerged. While 80% said smoking was a major cause of lung cancer and almost as many stated that it caused laryngeal cancers, less than 70% reported connections with pharyngeal and oral cavity cancers and only 50% reported a connection with tonsillar carcinoma. In the case of Reinke’s oedema, less than 30% believed that smoking is one of the main causes, although the studies are clear on this: not only is the development and recurrence of Reinke’s oedema primarily caused by tobacco consumption but also they have direct relationships with the number of daily cigarettes and the duration of smoking exposure. 8,9 The same applies to benign Whartin tumours of the salivary glands: less than 40% of the patients knew of this connection. However, Klussmann et al. had already shown in 2006 that 89% of the patients with such tumours were smokers and that the risk of bilateral tumours was significantly correlated with nicotine consumption. 7 As a comparison, the patients were also asked about carcinoma of the urinary bladder, for which smoking is the main risk factor along with occupational noxae. Only approximately 30% knew this, and approximately 40% thought it was possible but not proven. This result matches the finding in a study by May et al. on patients with bladder carcinoma, in which only approximately 60% of those with the disease thought a connection was possible. 14 Interestingly, smokers and ex-smokers tended to rate smoking as a risk factor even more frequently than non-smokers (see Figure 4).
Fifty-seven percent of the smokers in the present study stated that they would have stopped smoking before the onset of their disease if they had known about the harmful connection. These results clearly show that there is a need to catch up with regard to the ‘Warning’ aspect of the MPOWER project, that is, in the education of the population. 2 The 14 different warning labels on tobacco products play a relevant role here. Of these 14, however, there are only two carcinomas, namely, lung carcinoma and ‘cancer of the mouth, throat and larynx’, mentioned. Other tumour types are not mentioned. 15
Likewise, there is a relevant need for action with regard to helping patients quit (offering assistance). Only every second patient stated that they had received information about smoking being a risk factor for the development of the disease, and less than 50% stated that smoking was an unfavourable prognostic factor. Only 45.8% of the patients had been asked to reduce or quit smoking. Nearly 60% of the smokers had not been offered any help with regard to smoking cessation, and less than 10% had been offered a treatment plan or nicotine replacement products. Interestingly, most of the education had not been provided by ENT specialists but by general practitioners. Fortunately, the duration of the educational talks was longer than 5 minutes in almost 60% of the patients. Despite the poor dissemination of information, surprisingly, only 12% felt that the information provided by the treating physicians was not detailed enough.
Education about smoking, even in the presence of tumours, is important for several reasons. First, the time at which the diagnosis is delivered and therapy is started is a ‘teachable moment’, that is, an opportunity because patients are particularly open and committed to quitting. 12 In particular, patients who are already thinking about quitting should be particularly encouraged and supported at this time (more than 20% in the present study). In addition, numerous studies have shown that nicotine abstinence, even if it only starts at the time of diagnosis, leads to a significant improvement in prognosis in patients with malignant diseases. 6,10,16 For example, the 5-year survival rate for lung carcinoma patients increased from approximately 30% to more than 60%, and patients with head and neck tumours also experienced a significant decrease in mortality (relative risk 0.6) and longer recurrence-free survival. 11 As early as in 1993, a study by Browman et al. showed a correlation between the course of the disease and the timing of the initiation of nicotine abstinence in patients with head and neck tumours undergoing radiotherapy with and without fluorouracil. 17 The mortality risk decreased by 40% in patients who stopped smoking less than 12 weeks before the diagnosis compared to the risk in patients who continued to smoke. Abstinence from nicotine for at least one year before diagnosis led to a risk reduction of 70%. Voet et al. reported that in 383 patients undergoing primary radiotherapy for T1 glottic carcinoma, patients who continued to smoke during and after radiotherapy had a significantly higher 10-year complication risk. 18 Smoking was the most important significant single factor in that study. HPV is currently the main risk factor for oropharyngeal carcinomas and is found in over 70% of cases in the USA. While HPV-induced tumours were formerly considered a disease of young adulthood, the mean age of patients is now increasing significantly. 19,20 Although patients with HPV-positive carcinoma have a different risk profile and a better prognosis, Maxwell et al. showed that patients with HPV-positive oropharyngeal carcinoma who are also smokers have a 5.2-fold higher risk of recurrence after radiochemotherapy. 21 In ex-smokers who had quit more than one year before diagnosis, the risk had already decreased significantly from 34.4% to 19.6%. However, it only reached the level of non-smokers (6.1%) after a period of nicotine abstinence lasting longer than 20 years
Other studies, for example, in the field of urology, have also reported that the provision of information about the harmfulness of tobacco use by physicians is inadequate: Dombrowski et al. reported that more than 72% of the patients with a malignant urological tumour had not received information about smoking. 22 In another study specifically focused on patients with bladder cancer, only 33% of the patients were told to stop smoking by their doctor, only 42% of the smokers received information about nicotine and only 29% were given nicotine replacement products. 14 Similarly, in the population of patients with prostate cancer, in which active smokers are up to 80% more likely to have biochemical recurrences after radical prostatectomy, only 27.3% of the smokers were told to quit by their doctor, and only 18.2% received information about the effect of smoking on their prognosis. 13
There is a deficit in medical education in Germany. Smoking cessation is not part of the curriculum in the medical education system or further medical training. In addition, the medical service of smoking cessation counselling, that is, the time spent engaged in the medical motivational interview, is not paid for by the health insurance companies. 2,23 However, this time is important and should, if possible, be optimized by restructuring the framework of inpatient therapy in favour of patient education. 24 While the physician’s recommendation to stop using tobacco is effective and should be made at every appropriate opportunity, it has only a limited influence on the abstinence rate. 23 Conversations lasting at least 10 minutes and conducted according to the principles of motivational interviewing, with information on the long-term advantages of abstinence and the disadvantages of tobacco use, have been shown to be effective in both the short and long terms. 23 A recommended counselling algorithm is the five-step scheme of the 5 Rs: show the relevance, name the risks, work out the rewards (advantages), address the roadblocks (obstacles) and repeat the information. 23 Behavioural treatment elements, smoking cessation groups and medication support can significantly increase the success rate. The 6-question Fagstroem test can help clinicians assess the severity of tobacco dependence. 23
The present study was a pseudonymised questionnaire study. Such studies have some weaknesses: for example, there is a recall bias when using questionnaires, questions might not have been sufficiently understood by the participants, not all questions may have been answered or answered truthfully and socially desirable answers are more likely to be given. For example, Hald et al. showed that up to 50% of the tested persons reported incorrectly that they would no longer smoke, 25 and Alberg et al. reported that 24% of the responses were false negatives. 26 Nevertheless, questionnaire studies provide an important overview and information on the existing trends in the topic under investigation. It should be noted, however, that the study was done in a single centre and may not be generalizable.
In summary, the present study shows that there is a great need for medical education about smoking as a risk factor among affected patients. In particular, the time at which the diagnosis is communicated should be used as a ‘teachable moment’, and help with smoking cessation should be offered promptly. Improvements in medical education and cessation support are of great importance, especially in view of the fact that even nicotine abstinence starting at the time of diagnosis can lead to a significant reduction in mortality and an improvement in prognosis. In addition, it seems sensible to extend public education to other tumours, such as through warning labels on tobacco products, to ensure that the role of nicotine as a main risk factor is even more widely known.
Supplemental Material
sj-pdf-1-ear-10.1177_01455613211070899 – Supplemental Material for Tobacco use in patients with ENT tumours: Deficits in the provision of education and smoking cessation support
Supplemental Material, sj-pdf-1-ear-10.1177_01455613211070899 for Tobacco use in patients with ENT tumours: Deficits in the provision of education and smoking cessation support by Christian Rohrmeier, Hazem Salloum, Rainer Keerl, Christopher Bohr and Steffen Mueller in Ear, Nose & Throat Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in this study involving human participants were conducted in accordance with the ethics standards of the Ethics Committee of ‘Bayerische Landesaerztekammer’ in Munich (Nr. 18044, 05.09.2018) and with the 1964 Helsinki Declaration and its later amendments or comparable ethics standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.