
Abstract
Objective:
Secondhand smoke (SHS) is a major public health concern. In this study, we evaluated the global burden of otitis media (OM) due to SHS exposure during 1990-2019 and explored the impact of socioeconomic factors on it.
Methods:
With reference to the 2019 Global Burden of Disease (GBD) data, we assessed the OM burden linked to SHS during 1990-2019, stratified by gender, GBD region, and country. Join-point regression models analyzed trends in OM burden by calculating the average annual percent change (AAPC). Spearman’s correlation examined the relationship between the Socio-demographic Index (SDI), Healthcare Access and Quality (HAQ) index, and SHS-related OM burden.
Results:
During 1990-2019, age-standardized disability-adjusted life years (ASDRs) and age-standardized mortality rates (ASMRs) for OM due to SHS declined globally, with AAPCs of −1.45 for ASDR and −7.97 for ASMR. Significant declines in ASMR were noted in low-to-middle SDI regions. Regionally, Eastern Sub-Saharan Africa had the highest OM-related deaths, while South Asia had the highest disability-adjusted life years. OM burden decreased with higher SDI and HAQ.
Conclusion:
Despite global declines, significant regional and national disparities remained, which emphasizes the need for targeted interventions.
Introduction
Otitis media (OM) is a significant cause of hearing impairment and deafness, particularly among children aged <5 years and in populations within developing countries.1,2 The latest Global Burden of Disease (GBD) study indicates that despite a continuous global decline in OM incidence across all age groups from 1990 to 2019, there has been an increase in OM incidence among individuals residing in countries with medium Socio-demographic Index (SDI), the high-income Asia Pacific region, Eastern Europe, and Sub-Saharan Africa during this period. 3
The primary treatment for OM typically involves antibiotics, albeit their misuse can contribute to antibiotic resistance. 4 Therefore, primary prevention plays a crucial role in mitigating modifiable risk factors associated with OM. Secondhand smoke (SHS) exposure, also known as passive or involuntary smoking, presents a significant public health concern for nonsmokers. Approximately 37% of the global population remains exposed to smoke from tobacco products or exhalations, with women and children bearing a higher exposure burden than men, alongside significant racial and economic disparities.5,6 Tobacco smoke comprises thousands of chemicals and compounds, including numerous carcinogens, posing health risks upon inhalation. 7 Compelling evidence links environmental tobacco smoke exposure to OM, with a 2021 systematic review by Jones et al. revealing a 62% increased risk of OM in children cohabiting with smokers. 8 Animal studies have further confirmed the histological changes in the middle ear and Eustachian tube mucosal tissues due to chronic environmental tobacco smoke exposure. 9
Research on SHS exposure’s impact on OM has been geographically limited, often focusing on homogeneous populations within specific cities or counties, with a few national-level studies and minimal exploration of socioeconomic influences. This study utilized data from the 2019 GBD study covering 204 countries and regions with diverse socioeconomic and demographic characteristics to address these gaps. The objectives of this study were to (1) determine the global burden of OM due to SHS exposure, as stratified by gender, GBD regions, and countries; (2) analyze trends in OM burden during 1990-2019; and (3) examine the role of socioeconomic factors in OM burden related to SHS exposure. The study goal was to help policymakers identify high-burden areas and develop targeted public health strategies.
Materials and Methods
Data Sources
We analyzed cross-sectional data on 369 diseases and injuries, including OM, from the GBD database covering 21 regions and 204 countries during 1990-2019. The GBD 2019 study utilized diverse data sources such as vital registration systems, surveys, censuses, medical records, and scientific literature, applying standardized methods to estimate the disease burden by age, gender, location, and year. The key methods included the Cause of Death Ensemble model (CODEm), spatiotemporal Gaussian process regression, and the Bayesian meta-regression tool DisMod-MR. CODEm employs multiple modeling approaches for death analysis, as validated through predictive tests beyond the sample. DisMod-MR synthesizes data on incidence, prevalence, and mortality to ensure epidemiological consistency. Spatiotemporal Gaussian process regression analyzes data across time and regions to assess risk factor exposures and mortality rates. The details of the methods employed in GBD 2019 have been elucidated in a previous study. 10 The GBD study adheres to rigorous reporting guidelines using de-identified and aggregated data under the Institute for Health Metrics and Evaluation.
Definition
In the GBD 2019 study, OM is defined as a middle-ear infection encompassing acute OM, chronic OM, and hearing loss due to chronic OM, as outlined in the GBD nonfatal outcomes. Hearing loss estimates from chronic OM are detailed in a separate report. 11 Relevant International Classification of Diseases (ICD)-10 codes range from H65 to H75.83, and ICD-9 codes span from 381 to 384.9. Moreover, SHS is classified as a level 3 risk factor, with reference to current exposure to secondhand tobacco smoke at home, work, or public places, with non-daily smokers considered exposed. 12
Statistical Analysis
The mortality rates and disability-adjusted life years (DALYs) attributable to OM under SHS exposure during 1990-2019 were analyzed globally, regionally, and nationally using SDI. The mortality rate reflects OM-related deaths within a population over a period, while DALYs measure healthy life lost due to premature death and disability. SDI, a composite metric of income, education, and fertility, evaluates socio-demographic development, while the Healthcare Access and Quality (HAQ) Index assesses health care accessibility and quality based on facility availability, personnel efficacy, and intervention effectiveness. Rates and 95% uncertainty intervals (UI), derived from the Institute for Health Metrics and Evaluation, account for variability and missing data imputation through iterative sampling, which contrasts with confidence intervals (CI), relying on a standard error.
The Join-point regression model analyzed trends in age-standardized mortality rate (ASMR) and age-standardized disability-adjusted life year (ASDR) for OM attributable to risk factors from 1990 to 2019, segmenting time into intervals for nuanced trend analysis. Average annual percent change (AAPC) and its 95% CI were calculated, defining trends as increasing (AAPC >0), decreasing (AAPC <0), or stable (95% CI includes 0). 13 Spearman’s correlation explored associations between 2019 SDI and OM mortality and DALY rates due to SHS exposure. Statistical analyses were performed using GraphPad Prism (v8.0), R (v4.12), and Join-point regression (v4.9.0.0), with significance set at P < .05.
Results
Global Trends in OM Attributable to Various Risk Factors in 2019
In 2019, SHS exposure globally caused an estimated 25.17 OM-related deaths (95% UI: 8.44-74.35) and 123,056.65 DALYs (95% UI: 63,883.4-214,812.91) (Supplemental Material S1). The global ASMR and ASDR for SHS-related OM were 0.0004 per 100,000 people (95% UI: 0.0001-0.0011) and 1.79 (95% UI: 0.93-3.14), respectively. From 1990 to 2019, both ASMR and ASDR displayed significant declines, with AAPCs of −7.97 (95% CI: −8.29 to −7.66) and −1.45 (95% CI: −1.49 to −1.41) (Supplemental Material S2). Males experienced a higher burden of OM due to SHS, but females displayed a greater decline in ASMR (AAPC: −9.05; 95% CI: −9.53 to −8.56) than males (AAPC: −7.25; 95% CI: −7.66 to −6.84) (Supplemental Material S1 and S2).
Trends in OM by Region and Its Temporal Trends in 2019
The 2019 GBD analysis highlights regional disparities in the burden of OM due to SHS exposure. Eastern Sub-Saharan Africa reported the highest OM-related deaths at 17.49 cases (95% UI: 3.48-61.26) and ASMR at 0.0026 per 100,000 individuals (95% UI: 0.0005-0.0092), while South Asia showed the highest DALYs at 46,054.24 (95% UI: 23,946.74-81,744.76) and ASDR at 2.55 per 100,000 population (95% UI: 1.33-4.52) (Supplemental Material S1). From 1990 to 2019, South Asia achieved the most rapid ASMR decline, with an AAPC of −15.86 (95% CI: −16.38 to −15.33). Except for Central Asia, where the ASMR AAPC had a P-value of .06, reductions in mortality and DALY rates were statistically significant across other regions (Supplemental Material S2).
A Total of 204 National and Regional Burdens of OM Caused by SHS and Their Temporal Trends in 2019
Among 204 countries and territories, Somalia reported the highest OM-related deaths and ASMR due to SHS exposure, with 5.19 deaths (95% UI: 0.41-26.05) and an ASMR of 0.0129 (95% UI: 0.0011-0.0641) (Supplemental Material S3). India had the highest DALYs at 33,321.53 (95% UI: 17,501.73-59,586.1), followed by China with 16,403.37 (95% UI: 8341.18-28,261.03). Bangladesh and Indonesia reported the highest ASDRs at 3.12 (95% UI: 1.59-3.56) and 2.93 (95% UI: 1.5-4.15), respectively (Supplemental Material S3 and Figure 1). Temporal trends revealed significant variation, with Kiribati and Montenegro exhibiting the fastest increases in AAPCs for mortality and DALYs at 6.08 (95% CI: 5.51 to 6.65) and 0.31 (95% CI: 0.22 to 0.40), respectively. In contrast, Poland and Hungary achieved the steepest declines in mortality and DALYs rates (Supplemental Material S3 and Figure 2).
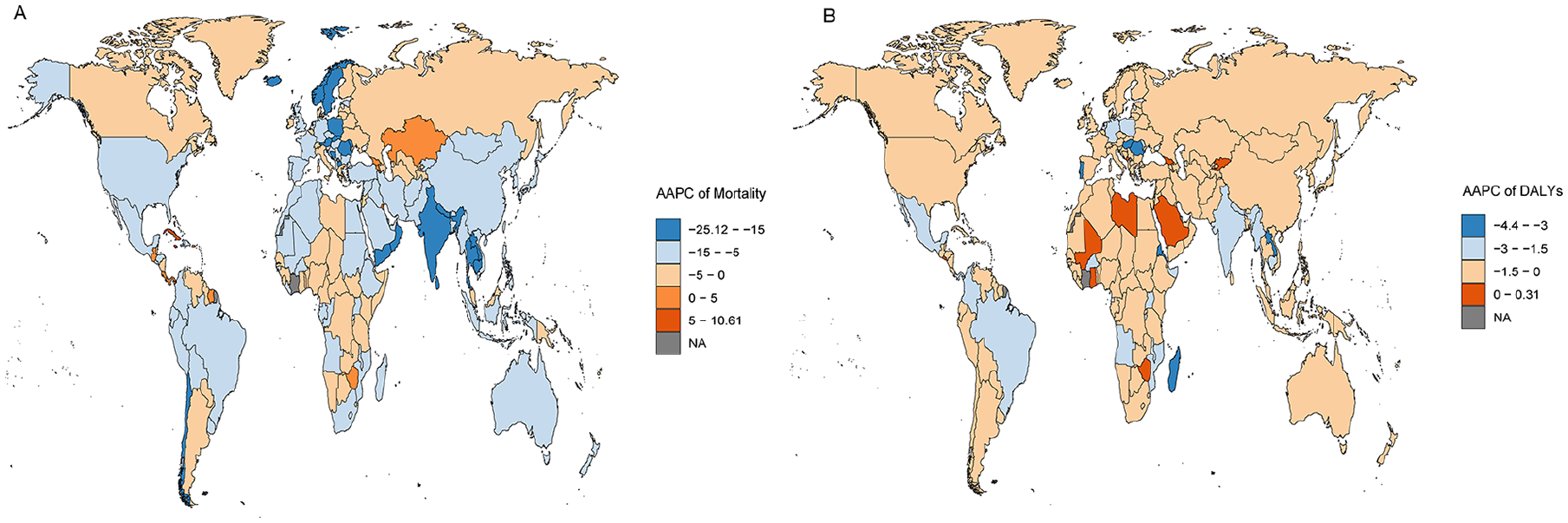
A global map of AAPCs in mortality (A) and DALYs (B) from otitis media attributable to secondhand smoke exposure from 1990 to 2019. AAPC, average annual percent change; DALYs, disability-adjusted life years.
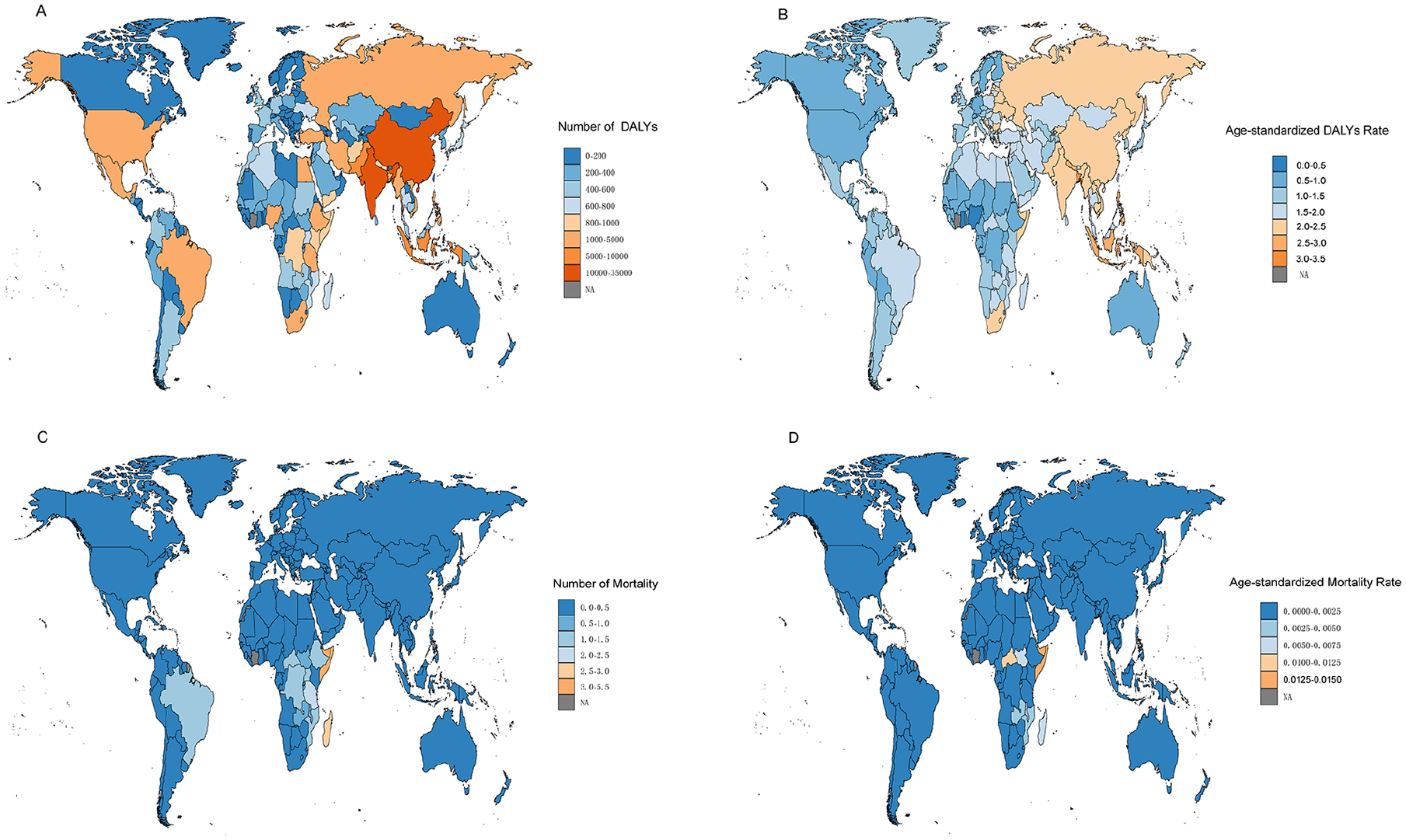
Global 2019 maps of otitis media DALYs (A) and mortality (C) attributable to secondhand smoke exposure, along with age-standardized rates of otitis media DALYs (B) and mortality (D) due to secondhand smoke exposure. DALYs, disability-adjusted life years.
The Global Burden of OM Due to SHS Exposure in Different SDI Regions and Its Temporal Trend
In 2019, significant disparities in the global burden of OM due to SHS exposure were observed across SDI regions. Lower middle SDI regions reported the highest DALYs at 39,780.83 (95% UI: 20,660.43-69,494.5) and ASDR at 2.17 (95% UI: 1.13-5.47) (Supplemental Material S1). Low SDI regions had the highest deaths and ASMR, with 19.53 deaths (95% UI: 4.06-64.18) and an ASMR of 0.0011 (95% UI: 0.0002-0.0036). From 1990 to 2019, all SDI regions experienced declining trends in ASMR and ASDR, with the sharpest ASMR reduction in lower middle SDI regions (AAPC of −12.45; 95% CI: −12.85 to −12.06) and the most notable ASDR decline in low SDI regions (AAPC of −1.8; 95% CI: −1.85 to −1.74).
The Relationship Between OM Burden at the National Level and SDI and HAQ Indexes
Figure 3 illustrates a significant inverse relationship between the ASMR for OM attributable to SHS exposure and both the SDI and HAQ index across 204 countries in 2019, with statistically-significant correlations (P < .001). In contrast, the association between ASDR for OM and the SDI and HAQ indices was not significant, yielding P-values of .565 and .101, respectively. Gender-specific analyses of the relationship between OM burden due to SHS exposure and the SDI and HAQ indices are presented in Figures S1 and S2. Thus, both females and males exhibited negative correlations between ASMR and the SDI and HAQ indices (P < .001). Interestingly, a significant negative correlation was observed between male ASDR and the HAQ Index (P = .018).
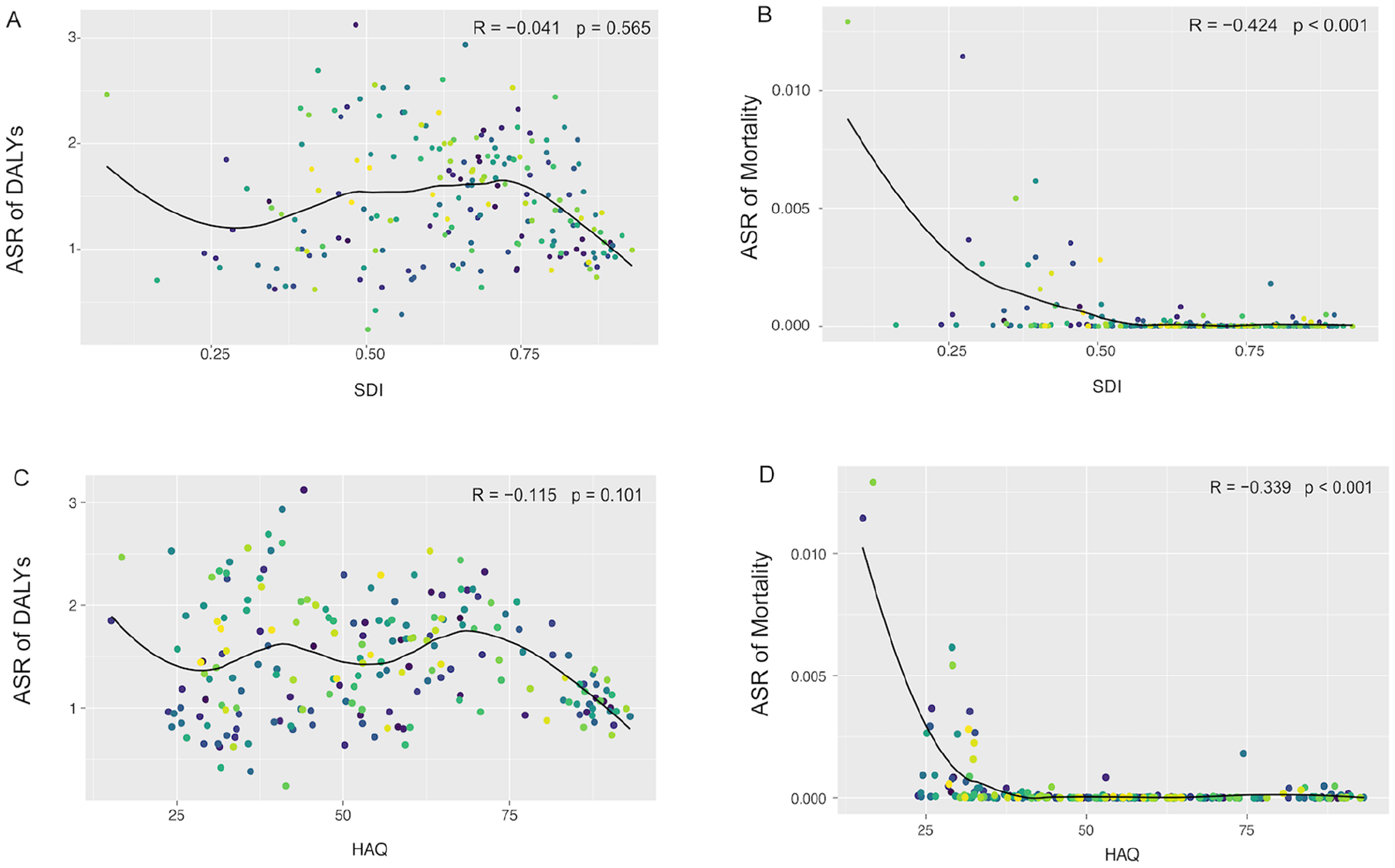
Age-standardized mortality and disability-adjusted life years of otitis media in 2019 in 204 countries and territories by sociodemographic and HAQ Index. (A) DALYs and SDI; (B) mortality and SDI; (C) DALYs and HAQ Index; (D) mortality and HAQ Index. The circles represent countries that had available sociodemographic, health care, and quality index data. CI, confidence interval; DALY, disability-adjusted life year; HAQ, Healthcare Access and Quality; SDI, Sociodemographic Index.
Discussion
This study is the first to comprehensively assess the global, regional, and national burdens of OM attributable to SHS exposure from 1990 to 2019. Over 3 decades, OM-related mortality rates and DALYs due to SHS have declined, highlighting advancements in prevention and treatment strategies. In 2019, higher SDI and HAQ index values correlated with reduced OM incidence and DALY burden; however, notable regional disparities remain.
Decades of research have confirmed strong links between tobacco use and diseases such as cancer, 13 as well as SHS exposure’s association with developmental issues in children, including low birth weight, reduced lung function, and worsened asthma.14-17 The pathogenesis of OM related to SHS involves several factors: (1) SHS exposure alters mucosal epithelium structure, impairing the respiratory and middle-ear mucociliary function, which, in turn, reduces bacterial clearance and promotes bacterial colonization; 18 (2) smoke exposure can modify airway epithelial cell gene expression, immune function, induce inflammation, damage epithelial tissue, and increase bacterial colonization;19,20 (3) tobacco smoke can enhance microbial adhesion to respiratory epithelial cells. 21 Past studies have shown how smokers have increased bacterial adhesion to respiratory cells, harboring more pathogens and fewer interfering biota than nonsmokers. 22 In 1983, Kraemer et al. first proposed a potential link between parental smoking and OM with effusion risk in children. 23 Since then, numerous studies have supported the connection between SHS exposure and otorhinolaryngological diseases.8,24 However, most research has been regionally limited, thereby hindering the global understanding. A major strength of the GBD study is its consistent observation periods, methods, and model specifications, which allow cross-country comparisons. Thus, the results of the present study highlight global changes in SHS-related disease burden, thereby emphasizing the need for more proactive measures in this direction.
Smoke-free policies are a key tobacco control intervention aimed at protecting nonsmokers from SHS while not directly reducing tobacco use, thus garnering broad support by creating smoke-free environments. 25 These policies, when implemented in public places, have proven to reduce heart disease and lung cancer rates, 26 emphasizing their critical role in public health. Research also shows that smoke-free laws reduce clinic visits for childhood ear infections, which further underscores their importance. 27
While the global burden of OM has declined, partly due to pneumococcal vaccines and changes in environmental and socioeconomic factors, challenges persist. 3 For example, the age-standardized prevalence of smoking among males and females aged 15 and over decreased by 27.5% and 37.7%, respectively. Despite progress in reducing the smoking rates worldwide, gaps remain in implementing tobacco-control measures. 28 Although global deaths and DALYs from SHS exposure decreased from 1990 to 2019, about 77% of the global population continues to face SHS exposure. 29 As the population grows, more numbers of nonsmokers are getting exposed to SHS, with significant regional differences in SHS-related disease burdens. 30
Research shows that, in countries such as China, India, Bangladesh, Indonesia, and the Philippines, where male smoking rates are high and smoke-free households are rare, around 430 million children face increased SHS exposure risks. 5 These countries, concentrated in South Asia, bear a significant OM burden from SHS. In contrast, residents of affluent areas in high-income countries, with higher education and greater engagement in tobacco control, typically experience less SHS exposure. 31 Children in lower and middle-income countries suffer more frequent OM episodes due to higher SHS exposure. 24 Globally, about 19% of men and 33% of women are at risk of SHS, with women facing higher exposure. 6 Therefore, smoke-free policies particularly benefit populations in low and lower middle SDI regions and women, where the decline in OM burden from SHS exposure is more noticeable. While smoke-free policies have yielded positive outcomes, their importance remains, which highlights the need for continued innovation in policy-making to further advance smoke-free initiatives.
Our research finds a significant negative correlation between socioeconomic indicators, such as SDI and HAQ, and the OM mortality rate from SHS exposure, highlighting the role of socioeconomic factors in the OM burden. Regions such as Eastern Sub-Saharan Africa and Somalia, with high SHS-related OM mortality, can partly attribute this to lower socioeconomic status and inadequate health care.32,33 While a negative correlation is observed between socioeconomic indicators and DALYs attributable to SHS exposure, the lack of statistical significance suggests that higher socioeconomic status may be associated with a reduced health burden. Gender-specific analysis revealed that men, who generally exhibit higher smoking rates in several regions, may experience a disproportionately-greater burden of SHS-related health issues. However, in areas with higher health care access (as indicated by HAQ indices), targeted interventions and early treatment appear to mitigate this burden, particularly among men. 34 This dynamic underscores the influence of gender-specific behaviors and health care access on the observed correlations, warranting further research to disentangle these complex interactions.
An ecological study spanning 31 European countries found no significant correlation between higher socioeconomic status and the facilitation of stricter tobacco control policies, contrary to expectations. 35 This finding suggests that the effective implementation of tobacco control policies may rely more on specific policy design and enforcement rather than solely on a country’s economic standing. Moreover, there is a need to adopt a multifaceted and tailored approach to public health strategies, particularly in curbing SHS exposure and its associated health impacts.
This study has multifaceted significance in public health. It highlights the global burden of OM from SHS exposure, emphasizing the need to raise awareness among health care providers, community workers, and individuals. Identifying regions with high SHS-induced OM burdens provides key geographic and demographic insights for evidence-based public health strategies. In addition, the study explores the role of socioeconomic factors in OM burden, stressing the need for improved education and public awareness in low- and lower middle-income countries. Such efforts can foster societal support, leading to stronger tobacco control policies and reduced public health burdens in these regions.
Despite its helpful contributions, our study has several limitations. Similar to previous research, 36 a key constraint is its exclusive focus on the relationship between time (year) and disease rates, neglecting other factors that may influence epidemiological trends. This limits our ability to fully capture the disease dynamics. Additionally, the study is affected by variations in the quality and availability of GBD data, particularly in low- and middle-income countries where limited health care infrastructure and diagnostic resources may lead to an underestimation of the OM burden, potentially skewing results. Consequently, more research is needed in regions with limited data to better assess the true OM burden. Lastly, the use of different methodologies across studies incorporated into our analysis could introduce estimation and informational biases, affecting the consistency and comparability of results.
Conclusion
Our findings demonstrate a significant global decline in the burden of OM attributable to SHS exposure. However, persistent high-burden regions and countries demand targeted attention and resource allocation. These results provide crucial evidence for shaping public health policies to mitigate SHS-related health impacts, particularly among vulnerable populations and resource-limited settings. Effective interventions in these areas can not only improve public health but also enhance socioeconomic well-being, offering a robust scientific basis for global health strategies.
Supplemental Material
sj-docx-1-ear-10.1177_01455613241310582 – Supplemental material for Global Burden of Otitis Media Attributable to Secondhand Smoke in 204 Countries and Territories from 1990 to 2019: The Analysis of the Global Burden of Disease Study
Supplemental material, sj-docx-1-ear-10.1177_01455613241310582 for Global Burden of Otitis Media Attributable to Secondhand Smoke in 204 Countries and Territories from 1990 to 2019: The Analysis of the Global Burden of Disease Study by Shuhan Liu, Sirui Wang, Xiaofeng Fan, Wei Tang, Yongran Cheng, Yu Sun, Wendi Shi and Lili Dai in Ear, Nose & Throat Journal
Supplemental Material
sj-docx-2-ear-10.1177_01455613241310582 – Supplemental material for Global Burden of Otitis Media Attributable to Secondhand Smoke in 204 Countries and Territories from 1990 to 2019: The Analysis of the Global Burden of Disease Study
Supplemental material, sj-docx-2-ear-10.1177_01455613241310582 for Global Burden of Otitis Media Attributable to Secondhand Smoke in 204 Countries and Territories from 1990 to 2019: The Analysis of the Global Burden of Disease Study by Shuhan Liu, Sirui Wang, Xiaofeng Fan, Wei Tang, Yongran Cheng, Yu Sun, Wendi Shi and Lili Dai in Ear, Nose & Throat Journal
Supplemental Material
sj-docx-3-ear-10.1177_01455613241310582 – Supplemental material for Global Burden of Otitis Media Attributable to Secondhand Smoke in 204 Countries and Territories from 1990 to 2019: The Analysis of the Global Burden of Disease Study
Supplemental material, sj-docx-3-ear-10.1177_01455613241310582 for Global Burden of Otitis Media Attributable to Secondhand Smoke in 204 Countries and Territories from 1990 to 2019: The Analysis of the Global Burden of Disease Study by Shuhan Liu, Sirui Wang, Xiaofeng Fan, Wei Tang, Yongran Cheng, Yu Sun, Wendi Shi and Lili Dai in Ear, Nose & Throat Journal
Supplemental Material
sj-tif-4-ear-10.1177_01455613241310582 – Supplemental material for Global Burden of Otitis Media Attributable to Secondhand Smoke in 204 Countries and Territories from 1990 to 2019: The Analysis of the Global Burden of Disease Study
Supplemental material, sj-tif-4-ear-10.1177_01455613241310582 for Global Burden of Otitis Media Attributable to Secondhand Smoke in 204 Countries and Territories from 1990 to 2019: The Analysis of the Global Burden of Disease Study by Shuhan Liu, Sirui Wang, Xiaofeng Fan, Wei Tang, Yongran Cheng, Yu Sun, Wendi Shi and Lili Dai in Ear, Nose & Throat Journal
Supplemental Material
sj-tif-5-ear-10.1177_01455613241310582 – Supplemental material for Global Burden of Otitis Media Attributable to Secondhand Smoke in 204 Countries and Territories from 1990 to 2019: The Analysis of the Global Burden of Disease Study
Supplemental material, sj-tif-5-ear-10.1177_01455613241310582 for Global Burden of Otitis Media Attributable to Secondhand Smoke in 204 Countries and Territories from 1990 to 2019: The Analysis of the Global Burden of Disease Study by Shuhan Liu, Sirui Wang, Xiaofeng Fan, Wei Tang, Yongran Cheng, Yu Sun, Wendi Shi and Lili Dai in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
We highly appreciate the work of the GBD 2019 collaborators.
Author Contributions
S.L. performed the statistical analyses, conducted the literature search, and wrote the first draft of the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published. All authors read and approved the final manuscript.
Data Availability
Data supporting the conclusions in this study are available from the corresponding author on a reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Hangzhou Health Commission Project (A20240124) and the Hangzhou Science and Technology Bureau Project (2021WJCY133) and the 2024 Anhui Provincial Health and Wellness Research Project—Youth Program.
Ethical Considerations
This study was approved by the Ethics Committee and the Information Department of the Hangzhou Normal University Affiliated Hospital.
Consent to Participate
Not applicable. Since all the data used in the current study are available online, and no individual patient was involved, it could be confirmed that we have obtained all written informed consent.
Consent for Publication
We declare that this article is original and has not been published in any other journal not is under consideration for publication in any other journal.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.