
Abstract
Objective
We conducted this meta-analysis to investigate the utility of anticoagulant treatment in lung cancer patients.
Method
We retrieved studies focused on thrombosis and lung cancer by searching electronic databases. We evaluated the impact of thrombosis on the prognosis of lung cancer patients, assessed the efficacy and effect of anticoagulation treatment in lung cancer patients, and investigated risk factors for thrombosis in lung cancer patients.
Result
Lung cancer patients with thrombosis have a significantly worse overall survival. Anticoagulant treatment did not improve the prognosis of lung cancer patients. Although anticoagulant treatment was associated with a reduced incidence of venous thromboembolism and pulmonary embolism, there was an increased risk of hemorrhage in this population. The risk factors for thrombosis in lung cancer patients are adenocarcinoma, advanced tumor stage, and high serum levels of d-dimer.
Conclusion
Anticoagulation treatment in lung cancer patients should be more individualized. Routine anticoagulant treatment is not recommended.
Introduction
Thrombosis, especially venous thromboembolism (VTE), is a common cardiovascular complication in malignant cancer patients. The occurrence of VTE, which includes deep vein thrombosis (DVT) and pulmonary embolism (PE), can interrupt treatment, decrease quality of life, result in increased treatment costs, and impact the prognosis of cancer patients. However, cancer as well as cancer treatments can increase the risk of thrombosis. It has been demonstrated that cancer alone increases the risk of thrombosis 4.1-fold, while chemotherapy is associated with a 6.5-fold increased risk. 1 Lung cancer, which is the most common cancer type, 2 increases the incidence of thrombosis compared with the general population.
While the incidence of thrombosis in lung cancer patients is increased, the relationship between lung cancer and thrombosis is complicated. Cancer cells can secrete thrombin, but they can also trigger the expression of several pro-coagulation factors in endothelial cells and mononuclear cells, consequently activating blood coagulation. 3 Moreover, leukocytosis has been reported to play an important role in lung cancer-associated thrombosis. Neutrophils generate neutrophil extracellular traps (NETs), and monocytes express tissue factor (TF), which promotes thrombosis. 4 Moreover, the chemotherapy agents used to treat lung cancer, such as gemcitabine, paclitaxel, cisplatin, and carboplatin have been proven to increase procoagulant activity via increased TF expression. 5 However, thrombosis can also impact cancer progression. Thrombosis can trap circulating tumor cells (CTCs) to form tumor thrombus, providing a favorable condition for CTC survival, and thus promote cancer metastasis, leading to poor patient prognosis. Moreover, thrombosis itself, especially PE, can be a potentially fatal complication.
Although the incidence of thrombosis is relatively high in lung cancer patients, anticoagulant treatment for this population is controversial. One reason is that anticoagulant treatment can increase the risk of hemorrhage. A previous report showed that anticoagulation-induced severe bleeding can occur in bevacizumab-treated patients. 6 Additionally, it is still unclear whether anticoagulant treatment in lung cancer patients improves prognosis, as we need to evaluate the benefit of prognosis against the risk of hemorrhage. It is also unclear how to identify the patient population that will need anticoagulant treatment. Herein, we conducted a meta-analysis with the goal of evaluating the impact of thrombosis on lung cancer prognosis, determining the main risk factor for thrombosis in lung cancer patients, and assessing the efficacy and effect of anticoagulant treatment in lung cancer patients.
Methods
Search strategy
We performed a systematic literature search of electronic databases, including PubMed, MEDLINE, the Chinese academic database Wanfang, and CNKI. We reviewed all articles published before May 2019 that studied the prognosis of lung cancer patients with thrombosis, the efficacy and effect of anticoagulation treatment in lung cancer patients, and the risk factors for thrombosis in lung cancer patients. The keywords “thrombosis” and “lung cancer” were used. We included both randomized controlled trials (RCT) and cohort studies in this meta-analysis. Two independent investigators separately retrieved the publications and evaluated the eligible studies. Studies lacking outcome data or without a control group were excluded. Any discrepancies between the two investigators were solved by consulting with a third investigator.
Quality assessment
The quality assessment of the included RCTs was conducted according to the Cochrane Handbook and composed by six terms in five aspects. The criteria included selection bias, performance bias, detection bias, attrition bias, and reporting bias. Each term defined as low risk scored a point, with higher scores indicating the better quality of the study. The highest score possible was 6, which meant the study was of very good quality. The quality of the included cohort studies was assessed based on the Newcastle–Ottawa Scale (NOS), which includes nine terms in three aspects: selection, comparability, and exposure or outcome. The highest score possible was nine, and similarly, higher scores meant a better quality study.
Data extraction
The study design information and outcome data were independently extracted by two investigators. The relevant information were first author, year of publication, observation or intervention arms, patient numbers of each arm, and survival outcomes or risk ratio. In each study, lung cancer patients with thrombosis or anticoagulant treatment were defined as the experimental arm, while lung cancer patients without thrombosis or anticoagulant treatment were defined as the control arm. Consensus of the two investigators was achieved for all information and data.
Statistical analysis
We conducted a pooled analysis of all studies to compare the prognosis of lung cancer patients with or without thrombosis. The survival outcomes we extracted were overall survival (OS) and hazard ratio (HR) with its 95% confidence interval (CI). A pooled HR<1 indicated a better prognosis of lung cancer patients with thrombosis, while a pooled HR>1 represented a better prognosis of lung cancer patients without thrombosis.
We also performed pooled analysis of the efficacy of anticoagulant treatment in lung cancer patients. The OS and its HR with 95% CI was assessed. Again, a pooled HR<1 indicated a better prognosis of lung cancer patients with anticoagulant treatment, while HR>1 suggested a better prognosis of lung cancer patients without anticoagulant treatment. Finally, we analyzed the effect of anticoagulant treatment on preventing thrombosis and causing hemorrhage risk by pooled analyzed the risk factors. A risk ratio (RR) was used for this evaluation.
Risk factors for thrombosis in lung cancer patients were also investigated by a pooled analysis. The observation goal was the odds ratio (OR) of each factor arm over the control arm. A pooled OR<1 favored the factor arm, suggesting the factor is protective. A pooled OR>1 favored the control arm, suggesting the factor is a risk factor for thrombosis in lung cancer patients.
All statistical analyses were performed by the Cochrane Review Manager (RevMan, version 5.3). Statistical heterogeneity was determined with Cochrane’s Q test and the I2 index. I2 < 50% or p value < 0.10 were considered to represent that significant heterogeneity did not exist, and thus the fixed-effects model was applied. Otherwise, the random-effects model was applied. Funnel plots were used to assess publication bias by constructing each study’s OR against the standard error (SE). Publication bias was determined by the shape of the funnel plot, where a symmetrical shape represented relatively low publication bias, while an asymmetrical shape indicated relatively high publication bias. Sensitivity analyses were performed by excluding the studies one-by-one.
Result
Study selection
In total, 3733 articles were obtained through the comprehensive database search and literature review (Figure 1). After removing duplications, 3329 studies were reserved. After carefully screening the titles and abstracts, 3259 studies were excluded because they were review papers, case reports, molecular level studies, or irrelevant studies. Among the remaining 70 studies, six were excluded because of they were irrelevant. Another 30 were excluded because they lacked relevant outcome data. Finally, 34 studies7–40 were considered eligible and included in this meta-analysis.

Flowchart of the study selection procedure.
Characteristics of the included studies
Among the 34 included studies, there were 10 RCTs and 24 cohort studies. Among them, six were focused on the prognosis of lung cancer patients with or without thrombosis, 15 investigated the potential risk factors of thrombosis in lung cancer patients, and two studied both the prognosis of lung cancer patients with or without thrombosis and the risk factors of thrombosis in lung cancer patients. The other 11 studies concerned the efficacy and effect of anticoagulation treatment in lung cancer patients. Altogether, in the pooled prognostic study of lung cancer patients with or without thrombosis there were 4416 patients in the thrombosis arm and 129,381 patients in the control arm. In the pooled study of the efficacy and effect of anticoagulation treatment in lung cancer patients there were 3451 patients in the anticoagulant treatment arm and 14,495 patients in the control arm. In the pooled risk factors study there were 5642 patients in the potential risk factors arm and 93,174 patients in the control arm. Among the 11 studies regarding anticoagulant treatment, 10 used low-molecular-weight-heparin (LMWH) as the anticoagulant agent and one used warfarin. Detailed characteristics of the included studies are listed in Table 1.
Characteristics of the included studies.

Abbreviation: LC, lung cancer; NSCLC, non-small cell lung cancer; SCLC, small cell lung cancer; RCT, randomize controlled trial.
Quality assessment
The Cochrane Handbook and NOS were used to assess the quality of RCTs and cohort studies, respectively. The quality assessment results for the 35 enrolled studies are presented in Table 1. For the 10 RCTs, one scored 3 points, three scored 4 points, three scored 5 points, and three scored 6 points. All 10 of the RCTs reported a proper randomize methodology. The major bias source came from the blinding of participants and outcome assessments. Additionally, for the 24 cohort studies, 11 scored 7 points, 12 scored 8 points, and one scored 9 points. The main source of bias came from the controls for additional factors. In summary, most the studies had a relatively high quality score, and no significant biases were observed.
Analysis of prognosis
The pooled analysis results of the eight studies that investigated the prognosis of lung cancer patients with or without thrombosis are presented in Figure 2. The results indicated a significantly worse prognosis of lung cancer patients with thrombosis compared with those without thrombosis (HR: 2.10, 95% CI: 1.82–2.42, p < 0.0001). As heterogeneity existed, the random-effects model was applied. There was no major source of heterogeneity, as the heterogeneity index did not change much when the studies were excluded one-by-one.

Comparison of prognosis between lung cancer patients with or without thrombosis.
Efficacy and effect of anticoagulant treatment
Anticoagulant treatment in lung cancer patients did not benefit prognosis, as there was no significant improvement in OS (HR: 0.95, 95% CI: 0.81–1.11, Figure 3a). However, anticoagulant treatment significantly reduced the incidence of thrombosis (RR: 0.52, 95% CI: 0.41–0.67, p < 0.00001, Figure 3b) and PE (RR: 0.55, 95% CI: 0.42–0.74, p < 0.0001, Figure 3c), but increased the risk of hemorrhage (RR: 1.91 95% CI: 1.34–2.74, p < 0.0004, Figure 3d).

Efficacy and effect of anticoagulation treatment in lung cancer patients. (a) Efficacy of anticoagulation treatment in lung cancer patients; (b) VTE risk in lung cancer patients with or without anticoagulation treatment; (c) PE risk in lung cancer patients with or without anticoagulation treatment; (d) hemorrhage risk in lung cancer patients with or without anticoagulation treatment.
Analysis of risk factors
OR was used to evaluate risk factors for thrombosis in lung cancer patients. In this meta-analysis, five factors (pathology type, chemotherapy, tumor stage, serum d-dimer level, and white blood cell count [WBC]) were investigated as potential risk factors.
Based on the pooled analysis (Figure 4), we found that adenocarcinoma (OR: 2.20, 95% CI: 1.68–2.88, p < 0.00001, Figure 4a), advanced tumor stage (OR: 1.62, 95% CI: 1.03–2.55, p = 0.04, Figure 4c), and increased serum d-dimer level (OR: 5.84, 95% CI: 4.25–8.03, p < 0.00001, Figure 4d) were the risk factors for thrombosis in lung cancer patients.
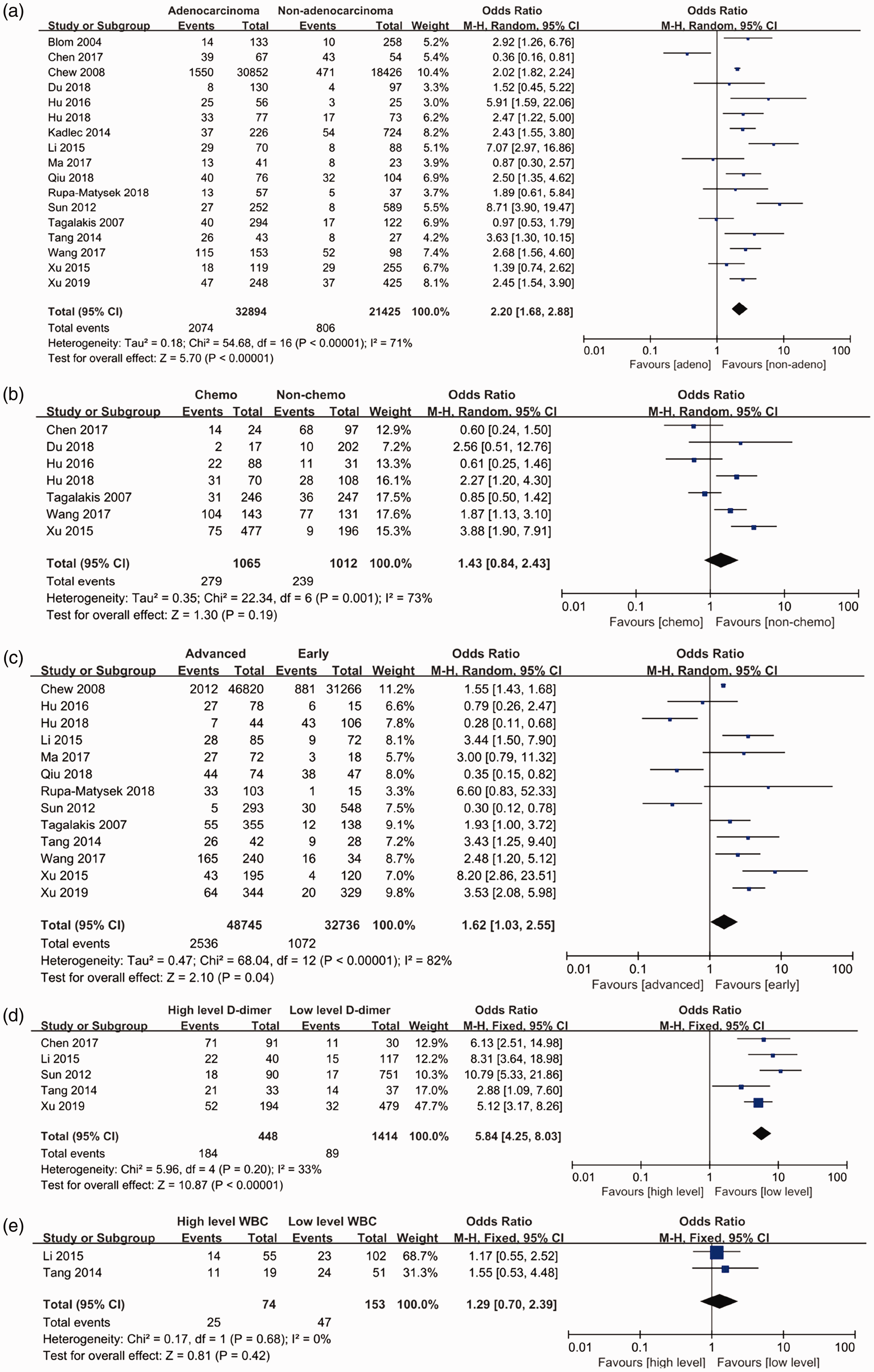
Risk factors for thrombosis in lung cancer patients. (a) Pathology type; (b) chemotherapy; (c) tumor stage; (d) serum d-dimer level; (e) white blood cell counts.
The publication bias was evaluated in both pooled pathology type analysis and tumor stage analysis. There was no obvious bias observed as the shape of the funnel plots was basically symmetrical (Figure 5).

Potential publication bias, as analyzed by funnel plot. (a) Publication bias for the pathology type analysis; (b) publication bias for the tumor stage analysis.
Discussion
The interaction between malignant tumors and activation of the coagulation system has been investigated for over a century. Thrombosis has been reported to be common complication in cancer patients. 41 However, lung cancer has been reported to be in the group of cancers that have the highest incidence of thrombosis. 42 The mechanism of the high thrombosis incidence in malignancies is complicated because several hemostatic factors and signaling pathways are involved in the process. It has been demonstrated that cancer cells can express procoagulant factors including TF, cancer procoagulant (CP), and heparanase, which are important for activation of the coagulation cascade. Tumor cells can also secrete soluble mediators such as tumor necrosis factor α (TNFα), interleukin-1β (IL-1β) or make direct contact with the host vascular and blood cells to stimulate the expression of procoagulant factors in these cells. 43 As previously mentioned, the NETs released by neutrophils also contribute in platelet adhesion and thrombosis. In summary, malignancies give rise to a blood hypercoagulable state in cancer patients. In turn, coagulation factors such as TF and thrombin, which have also been demonstrated to facilitate cancer cell migration, angiogenesis, and to impact host vascular cells, thus promoting cancer invasion and metastasis, contribute to cancer dissemination through activation of protease-activated preceptors (PARs). 44 The crosstalk between tumor cells and thrombosis create a vicious circle that impacts malignant processes. In this meta-analysis, we found that the prognosis of lung cancer patients with thrombosis is worse than those without thrombosis. This finding could either be due to the impact of thrombosis on disease progression or the occurrence of fatal PE.
As thrombosis contributes to a worse prognosis of lung cancer patients, we next investigated whether anticoagulant treatment improved patient status. Heparin and LMWH, which is purified from natural glycosaminoglycans (GAGs), is widely used in clinical practice for thromboprophylaxis and anticoagulant treatment. 45 In addition to its anticoagulation effect, LMWH has also been confirmed to have an anticancer effect. An in vitro study revealed that the second generation LMWH Bemiparin inhibited angiogenesis of the microvascular endothelium that is triggered by the conditioned media from human lung cancer, breast cancer, and leukemia cell lines. 46 LMWH has also been proven to have anti-metastatic effects in a mouse model of lung cancer . 47 The other commonly used anticoagulant agent, warfarin, also provides an antitumor effect. 48 Therefore, in a high thrombosis incidence population such as lung cancer patients, LMWH and warfarin are generally used as a part of a treatment strategy that attempts to improve survival. However, the efficacy and effect of anticoagulant treatment remains controversial. Several clinical trials have revealed that anticoagulant treatment improved the OS of lung cancer patients,16,17,20,25 whereas more trials have shown little evidence for an improvement of OS from anticoagulant treatment among lung cancer patients.18,19,21–24 In this meta-analysis, pooled analysis of 11 studies that compared the efficacy and effect of lung cancer patients with or without anticoagulant treatment showed no improvement in OS, although anticoagulant treatment effectively reduced the occurrence of VTE and fatal PE. The reason for this finding could either be due to the generally poor prognosis of lung cancer itself, or inadequate dosages and times of anticoagulant treatment. Furthermore, anticoagulant treatment significantly increased hemorrhage risk in lung cancer patients. In summary, based on the results of this meta-analysis, routine anticoagulant treatment in lung cancer is not recommended. However, the occurrence of thrombosis in lung cancer patients was associated with worse survival outcomes; thus, it is important to develop novel and effective anticoagulant treatment strategies, or to make anticoagulant treatment more individualized and precise.
To determine the characteristics of lung cancer patients who are more likely to develop thrombosis, we next conducted a meta-analysis of risk factors for thrombosis in lung cancer patients. These results showed that a pathology of adenocarcinoma, advanced tumor stage, and high levels of serum d-dimer were risk factors for thrombosis. Although routine anticoagulation treatment is not recommended for lung cancer patients, there is evidence to suggest benefits from giving such treatments to these high-risk groups. However, further clinical trials are needed to determine if anticoagulant treatment can improve the prognosis of these high-risk lung cancer patients.
Taken together, the results of this meta-analysis indicated that thrombosis is associated with a worse prognosis in lung cancer patients, but the pooled efficacy analysis revealed that anticoagulation treatment did not significantly improve survival, despite reducing the risk of VTE and PE. Therefore, a more precise anticoagulant treatment is recommended rather than routine anticoagulant treatment. Further analysis showed that adenocarcinoma pathology, advanced tumor stage, and a high serum d-dimer levels were risk factors for thrombosis in lung cancer patients. This result gave us an indication of which lung cancer patients should receive anticoagulant treatment.
Inevitably, our meta-analysis had limitations. Owing to the limitations of the included studies and their data, we were unable to perform any subgroup analysis for the efficacy of anticoagulant treatment based on pathology type, tumor stage, or other patient characteristics. Such subgroup analyses could give us a better idea of which groups of patients would actually benefit from anticoagulant treatment, which would provide a clearer direction for a treatment strategy.
Conclusion
In this meta-analysis, we found that lung cancer in combination with thrombosis had a worse prognosis compared with patients without thrombosis. Anticoagulant treatment did not improve the prognosis of lung cancer patients; although it was associated with a reduced risk of VTE and PE, there was also an increased risk of hemorrhage. Adenocarcinoma, advanced cancer stage, and high serum d-dimer level are risk factors for thrombosis in lung cancer patients. More individualized and precise anticoagulant treatment is recommended in lung cancer patients instead of routine anticoagulation treatment.
Footnotes
Author Contributions
Conception and design, C.H. and M.Z.; methodology, M.Z. and S.W.; analysis, M.Z.; validation, M.Z. and S.W.; original draft preparation, M.Z.; review and editing, M.Z. and C.H.; supervision, C.H.
Acknowledgments
We sincerely thank all the reviewers and editors for their supportive suggestions.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.