
Abstract
This case involves a 30-year-old female who suffered extensive facial burns as an outcome of a horrific assault. The patient subsequently underwent 2 surgeries with the ultimate goal of reducing the cosmetic, physical, and thus mental burden the assault caused. The technique of choice was the novel trapezius fasciocutaneous flap for burn reconstruction of the neck. It is discussed that while this technique is still deemed a novel procedure, its unique characteristics make it an excellent choice for cases similar to this one. While this approach has not been widely popularized in the treatment of patients with burn contracture requiring reconstruction, the donor site characteristics and ideal functionality make the trapezius fasciocutaneous flap such an excellent choice. This particular type of graft yields a hidden donor site, contains rich vascularity with physical qualities similar to those of facial skin, specifically in regard to thickness, color, and texture, and ultimately produces the most ideal cometic outcome. Further, the wide arc of rotation unique to this flap allows for better manipulation and mobility at the transplanted location. While the anatomic implications are very relevant to head and neck surgery, this method also produces exemplary cosmetic outcomes when compared to other graft procedures.
Intro
Burn contracture can pose significant cosmetic burden to the patient as it places additional weight, thus pulling and deforming many structures of the face. Use of a trapezius fasciocutaneous flap for burn reconstruction was first described in 1996. 1 This particular surgical graft has not been widely popularized, but the large area of thin, pliable, well-vascularized tissue in addition to a camouflaged donor site proves it to be an excellent choice for head and neck reconstruction. 2 This technique is an esthetically pleasing choice in patients who may otherwise not be able to undergo regional or fat grafts. Additionally, by design, these patients do not suffer extensive donor site dysmorphia, as seen in various myocutaneous flaps. 2
Case
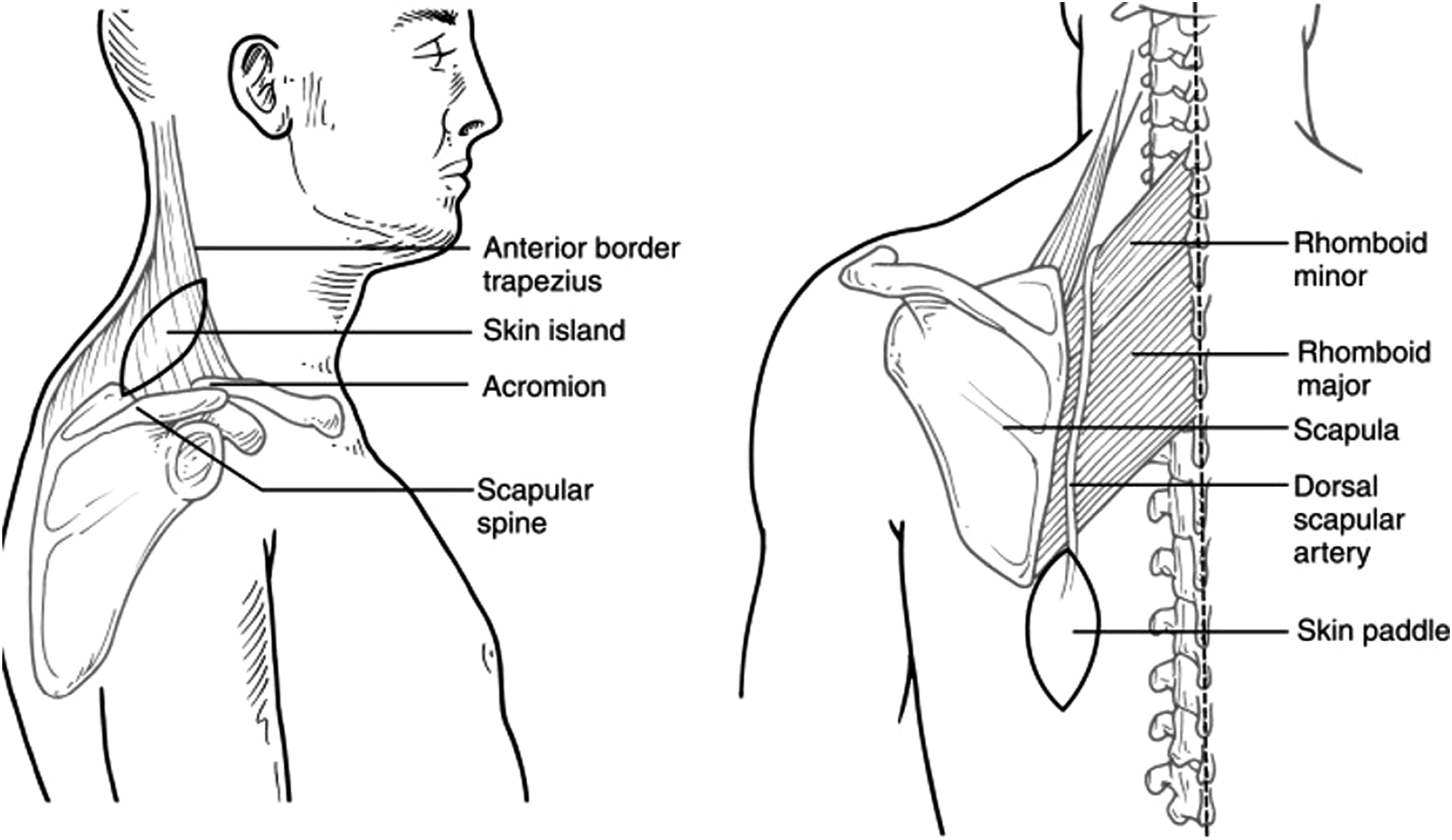
This patient is a 30-year-old female who was beaten unconscious with a hammer and subsequently doused in gasoline and set on fire by her ex-husband. Following the horrific assault, she underwent multiple surgeries for her extensive facial burns with scar contractures. The patient agreed to undergo a novel trapezius fascial cutaneous flap. In the first operation to accomplish this, the flap length was identified and drawn. Borders of the incision were from the right of the spinal column extending to the left of the medial edge of the scapula and down the inferior border of the scapula. The dissection proceeded through the subcutaneous tissue until the fascial layer was identified. The flap was dissected from the teres major and minor as well as the trapezius, and subsequently rotated superiorly (Figure 1). The vascular stalk was narrowed as much as deemed feasible and subsequently elevated. To address the scar bands, the patient was then laid supine, and excision was carried along the anterior neck about 3 fingerbreadths above the clavicle within the preexisting scar. The excision was also carried through the platysma and scar bands were lysed. The skin pedicle was detached under the subcutaneous edges, and the flap was inserted and secured with 4-0 Vicryl with skin closure with a staple and 5-0 Monocryl suture. The flap proved viable at the conclusion of the case. Anatomy of the trapezius flap.
5
The patient presented again the following year for further revision of the previous extended rotational flap. A skin graft was borrowed from the left thigh. An incision was made over the right lateral aspect of the previous flap, and dissection was continued until the sternocleidomastoid muscle was identified. The scars were lysed and the flap was then advanced for coverage of that area. It was secured with interrupted 3-0 Vicryl for the subcutaneous later and 5-0 Monocryl for the cutaneous closure. Following this, an incision was made along the left inferolateral aspect of the flap and carried down to the muscle. A scar band of the sternocleidomastoid was identified and released, measuring about 3.5 cm. A skin graft was applied to cover the area and set with a 4-0 chromic suture. Lastly, the left auricle scar band was released using an incision and dissection to create an auriculocephalic crease. The crease was recreated with the skin graft and set in place with 4-0 chromic. The graft took well without any complications. The patient was very pleased with the cosmetic result of both procedures.
Discussion
Use of a trapezius fasciocutaneous flap for head and neck scar contracture, while a cosmetically and logistically favorable option, is still considered a novel flap procedure. Hesitations may arise due to the variation of local vasculature and uncertainty of the anatomic nomenclature.
3
Such an undertaking should certainly be considered when the patient lacks other viable donor site options. The trapezius flap has a wide arc of rotation, making it ideal for any lesions involving the occiput, nuchal, or spinal areas.
3
It is also an advantage that the skin overlying the area supplied by the transverse cervical artery, specifically the supraclavicular portion of the flap, is very useful for facial lesions due to its similar color and texture to that of the facial skin (Figure 2).
4
Many of the more popular graft options, namely, myocutaneous flaps of the deltopectoral, epaulet, and pectoralis major areas can cause significant anterior chest deformities, making them less cosmetically desirable, especially in the female population.
2
The fascial cutaneous flap option is much more desirable due to lack of contracture, as well as the absence of mobility issues that are commonly encountered in musculocutaneous donor flap sites.
2
Pre-op (left) and post-op (right) result of the patient who underwent the procedure
Conclusions
Although there are few reports of trapezius fasciocutaneous flap for burn reconstruction, the implications of this procedure for severe neck contracture are very favorable. The pliability of the grafted tissue, rich anastomoses, ability to blend well with normal facial skin, and hidden nature of the donor site make for excellent functional and cosmetic outcomes for patients.