
Abstract
Objectives
When there is a difference in hearing on both ears, where to perform the first cochlear implantation (CI) becomes an important issue. The purpose of the study was to evaluate which ear should be chosen for the first implantation in sequential bilateral CI with a long inter-implant period.
Methods
The study population consisted of 34 severe-to-profound sensorineural hearing loss pediatrics with the inter-implant period of ≥3 years between the first CI (CI-1) and the second CI (CI-2) before the age of 19 (mean of inter-implant period: 7.1-year). The patients were classified into Group A (CI-1 was performed on the ear with better hearing), Group B (CI-1 on the ear with worse hearing), or Group C (symmetrical hearing in both ears). Speech intelligibility test results were compared between the groups.
Results
The monosyllabic word scores of CI-1 were excellent in Groups A (91.7±7.9%) and B (92.5±3.6%) but slightly lower in Group C (85.7±14.9%) before the second implantation (P = .487). At 3 years after the second implantation, all groups demonstrated excellent scores in the bilateral CI condition (95.9±3.0% in Group A; 99.1±.8% in Group B; 97.5±2.9% in Group C, P = .600). However, when the patients were tested in using CI-2 only in Groups A and B after using bilateral CI for 3 years, the scores were inconsistent in Group A (79.6±23.9%; range: 22.2-94.4%), while those were higher and more constant in Group B (92.9±4.8%; 86.8-100.0%).
Conclusions
The first CI is strongly recommended to perform on a worse hearing ear if they had different hearing levels between ears. Even with the first CI on a worse hearing ear, its performance never deteriorates. In addition, if they receive the second CI several years later, it will be likely that the second one functions better.
Keywords
Introduction
Binaural hearing plays an important role in sound localization and the understanding of speech in noisy environments.1–4 In bilateral severe-to-profound sensorineural hearing loss (SNHL) pediatric patients, it can be only achieved through bilateral cochlear implantation (CI). Studies have shown that the bilateral implantations were better not only for sound localization and speech understanding in noise but also for the quality of life and language development.5–7 As a result, bilateral CI is now strongly recommended for pediatric patients with bilateral severe-to-profound SNHL.8–10 Simultaneous bilateral surgeries are ideal but sequential surgeries have also shown favorable outcomes.11–14 In sequentially performed surgeries, however, the shorter the interval between the two implantations, the better the outcomes; thus, it is recommended to undergo both surgeries within 12 months.4,6,8,15–17
Nevertheless, neither simultaneous nor sequential CI with a short inter-implant period are feasible for some patients. Typically, the financial burden may be a reason.18,19 However, although there was no financial burden, a few of parents refused to undergo bilateral surgeries for other reasons. 20 In such instances, more careful decision-making is necessary when planning the first CI (CI-1). Furthermore, if a patient shows a different hearing level between ears (ie, 85 dB of threshold in one ear and >90 dB in another), the selection of the ear to undergo CI-1 becomes more important. If CI-1 is performed on the ear with better hearing, better performance of the CI-1 may be expected. If a patient and parents eventually refuse to receive the second CI (CI-2), the decision to perform CI-1 on the better ear would be appropriate. However, the provision of auditory stimulation on the contralateral ear (the ear with worse hearing) is likely to be very limited; the ear would inevitably be nearly deprived of sound. On the other hand, when CI-1 is performed on the ear with worse hearing, a hearing aid (HA) on the contralateral ear can provide auditory stimulation, which will prevent the deprivation on the ear. If a patient and parents finally decide to be given the second implant a few years later, the decision to perform CI-1 on the worse ear may be suitable. However, comparing with CI-1 on the better ear, there would be a concern that the performance of the CI-1 on the worse ear might be somewhat reduced.
This study was designed and performed to resolve those issues, establishing the evidence for the concerns that which ear was appropriate for the first implantation. Particularly, the study will help surgeons decide the first implant ear if a patient would even have a long inter-implant period.
Materials and methods
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Review Board of Ajou University Hospital (AJIRB-MED-MDB-19-449) and with the 1964 Helsinki declaration and its later amendments or comparable standards.
Subjects
This study included prelingual bilateral severe-to-profound SNHL pediatric patients who underwent sequential bilateral CI between January 2002 and December 2016 at the Department of Otolaryngology, Ajou University Hospital, Suwon, Republic of Korea. Both CI-1 and CI-2 were performed before patients reached 19 years of age. Patients with inner ear anomalies or other systemic disorders including intellectual disability that could affect surgical outcomes were excluded. Thirty-four patients were finally included in the study. In all subjects, the surgeries were performed by round window approach for the electrode insertion with soft surgery techniques. Pre-, peri, and postoperative steroids (0.1 mg/kg body weight) were applied. Manufacturers of the implant device were Cochlear, MED-EL, or Advanced Bionics.
The Inter-implant period between two surgeries
The inter-implant period was equal to or longer than 36 months in all patients. Thus, 34 patients were finally included in this study. All of them were successfully followed up for at least 3 years. Their mean inter-implant period reached 7.1 (±2.9) (range 3.0-14.2) years.
Hearing differences and grouping
When preoperative pure-tone audiometry was available, the hearing difference between both ears was evaluated based on the pure-tone thresholds. If pure-tone audiometry could not be performed, the difference was determined by auditory steady-state evoke responses, especially in young children. The hearing differences were measured as the average of thresholds at 500, 1000, 2000, and 4000 Hz. If neither pure-tone audiometry nor auditory steady-state evoked response data were available, auditory brainstem responses were used in each patient.
Patients with hearing differences ≥5 dB were included in this study. Thirty-four patients were classified into either Group A (CI-1 on the ear with better hearing; “better group”) (n = 12), Group B (CI-1 on the ear with worse hearing; “worse group”) (n = 10), or Group C (no difference in hearing level between ears) (n = 12) based on the hearing level at the time to undergo their first CI.
Performance of CI and statistical analyses
Data were collected regarding sex, ages at CI-1 and CI-2, inter-implant period, preoperative hearing thresholds, and manufacturer of the implanted devices. Speech intelligibility test results (monosyllabic word, disyllabic word, and sentence scores) were investigated under aided conditions, CI-1 only and CI-1 with HA, before CI-2 surgery. Those scores were also evaluated under aided conditions, CI-1 only, CI-2 only, and bilateral CI, at 1 and 3 years after implantation of CI-2.
The Mann–Whitney U test and the Kruskal–Wallis H test were used to compare the difference for continuous variables. The Chi-square test was used for categorical variables. All statistical analyses were performed using IBM SPSS Statistics for Windows (version 23.0; IBM Corp., Armonk, NY, USA). In all analyses, P < .05 was taken to indicate statistical significance.
Results
Ages at surgeries and the inter-implant period
Demographic characteristics of the patients.
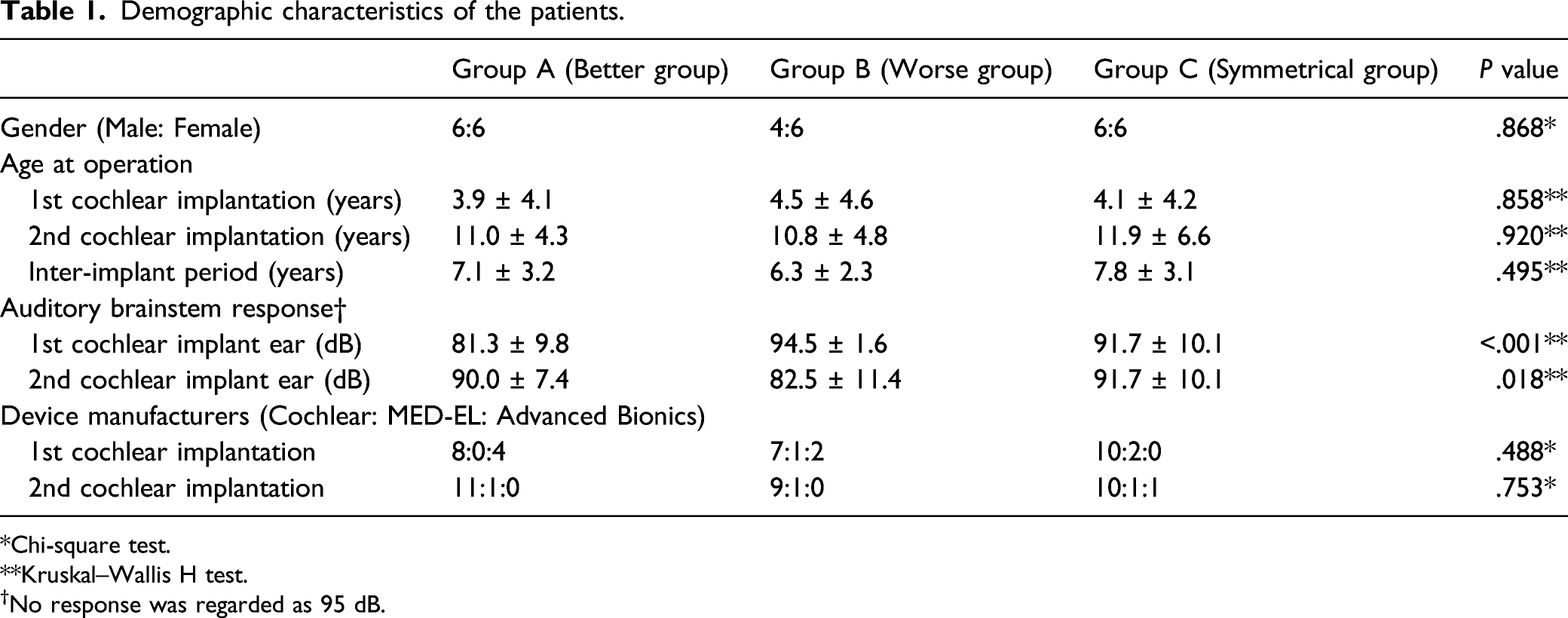
*Chi-square test.
**Kruskal–Wallis H test.
†No response was regarded as 95 dB.
Performance of CI-1 before the second implantation
Tests in the CI-1 only condition were used to compare the performance of CI-1 just before the second implantation (Figure 1). In the Group A, the monosyllabic word score was 91.7 (±7.9) %, disyllabic word score was 94.5 (±12.1) %, and sentence score was 92.9 (±9.4) %; in the Group B, these scores were 92.5 (±3.6) %, 97.7 (±1.7) %, and 92.2 (±9.5) %, respectively; the scores were 85.7 (±14.9) %, 90.6 (±16.5) %, and 78.4 (±27.1) %, respectively, in the Group C. Although the scores in Group C were slightly low, there were not statistically significant. Performance of the first cochlear implant (CI) before the second implantation in the CI-only condition. Group C showed slightly lower performance; however, there were no statistical significances (Kruskal–Wallis H test).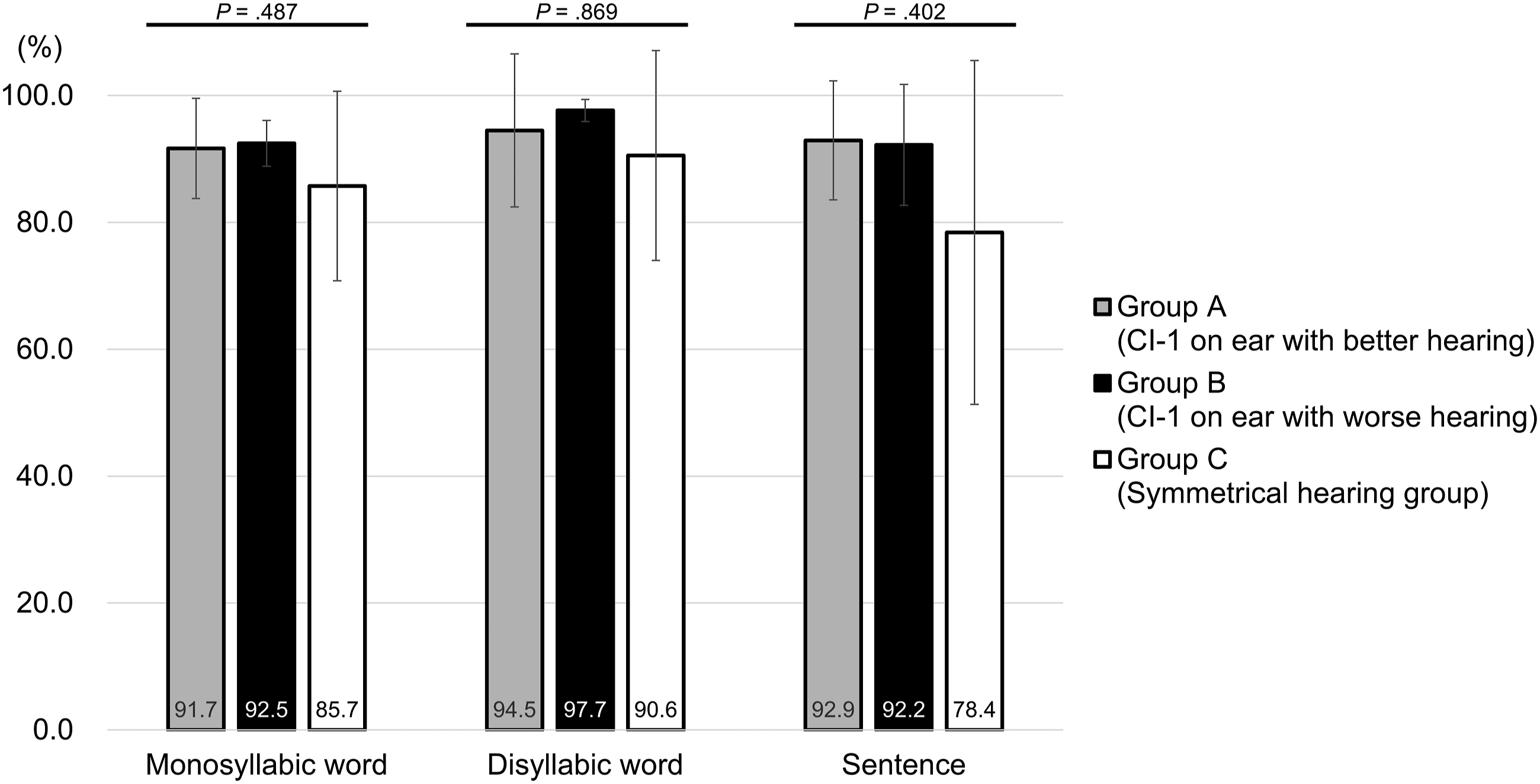
Changes in the speech intelligibility scores in bilateral CI condition
The test results were compared in the bilateral CI condition after CI-2 (Figure 2). The average monosyllabic word scores were 92.5 (±8.9) % in Group A, 93.9 (±3.0) % in Group B, and 85.1 (±15.4) % in Group C under the CI-1 with HA condition. The scores increased after the CI-2 under the bilateral CI condition. After 3 years from CI-2, those scores were 95.9 (±3.0) %, 99.1 (±.8) %, and 97.5 (±2.9) % in Groups A to C, respectively, (Figure 2A). Group C showed slightly poor performance of CI-1 but excellent scores in the bilateral CI condition. Similar patterns were observed in disyllabic word and sentence scores. The average disyllabic word scores were 96.2 (±7.8) %, 97.1 (±3.4) %, and 91.5 (±16.1) % in the Groups A to C, respectively, under the CI-1 with HA condition; those increased each 99.6 (±.6) %, 100 (±.0) %, and 100 (±.0) % after 3 years in the bilateral CI condition (Figure 2B). In sentence scores, it increased from 91.0 (±17.1) % to 98.1 (±2.3) % in the Group A, 92.2 (±11.3) % to 99.0 (±2.3) % in the Group B, and 79.6 (±26.2) % to 96.6 (±6.9) % in the Group C (Figure 2C). Changes in performance in the bilateral cochlear implant (CI) condition. Longitudinal changes of scores of (A) monosyllabic word, (B) disyllabic word, and (C) sentence for 3 years.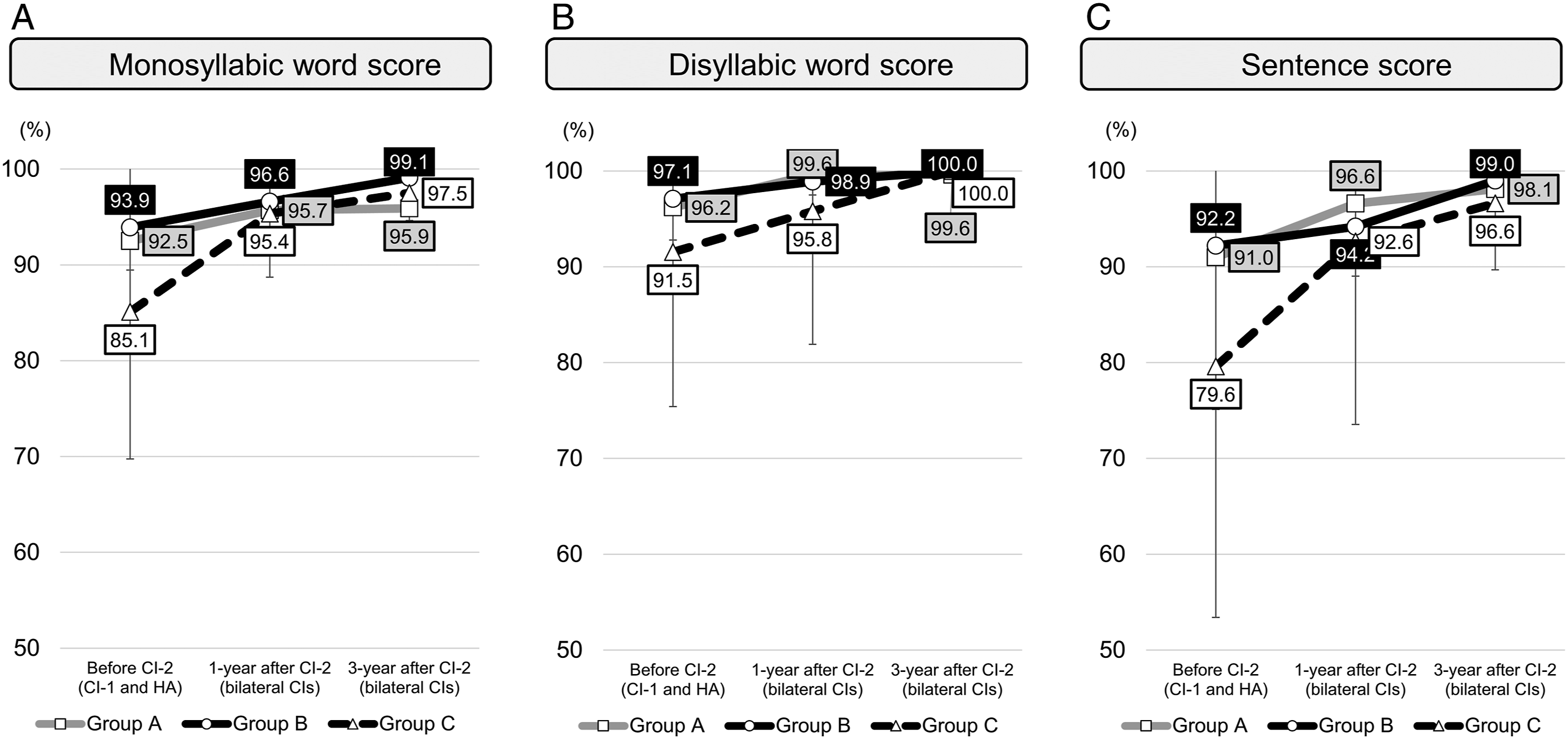
Performances in “CI-1 only” and “CI-2 only” conditions in Groups A and B
In the bilateral CI condition, there were no differences in speech test results between Groups A and B (Figure 2). However, when the tests were performed in the bilateral CI condition, it remained unclear whether the results were from simultaneous binaural hearing using both CIs or from one better hearing ear with CI. Therefore, the results of the test were compared again in each condition of the “CI-1 only” and “CI-2 only” (Figure 3). Comparison of speech intelligibility test results between the first and second cochlear implantations (CIs) in each CI-only condition. (A) Monosyllabic word score in Group A. (B) Monosyllabic word score in Group B. (C) Disyllabic word score in Group A. (D) Disyllabic word score in Group B. (E) Sentence score in Group A. (F) Sentence score in Group B. * P < .05 (Wilcoxon signed-rank test).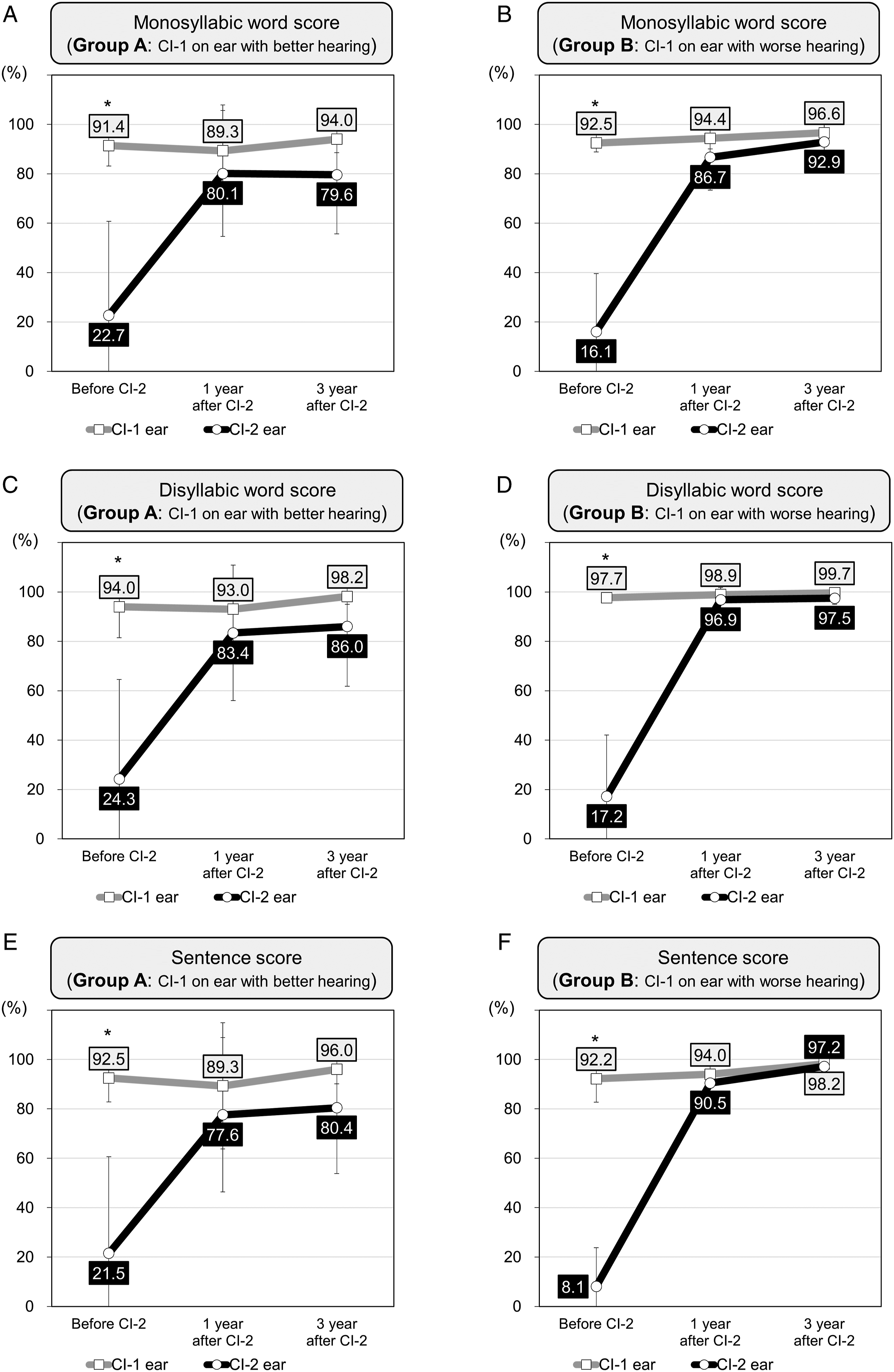
In monosyllabic word scores of Group A, the performances of CI-2 were poorer than those of CI-1. The scores of CI-1 were over 90% (89.3 [± 18.5] % and 94.5 [± 5.5] % at 1- and 3-year after CI-2, respectively), whereas the scores of CI-2 were around 80% (80.1 [± 25.5] % and 79.6 [± 23.9] %) (Figure 3A). On the other hand, Group B showed better results than Group A in monosyllabic word scores. The performances of CI-2 were 86.7 (±13.2) % and 92.9 (±4.8) % at 1- and 3-year after CI-2, respectively, (Figure 3B).
In disyllabic word scores, the two groups showed similar results as in monosyllabic word scores. In the Group A, the scores of CI-1, 93.0 (±17.8) % and 98.2 (±3.2) %, were about 10% higher than those of CI-2, 83.4 (±27.4) % and 86.0 (±24.2) %, at both 1- and 3-year after CI-2 (Figure 3C). However, in the Group B, the scores of CI-1 and CI-2 were similarly outstanding at both 1- and 3-year after CI-2 (98.9 [± 2.9] % and 99.7 [± .6] % in CI-1; 96.9 [± 4.2] % and 97.5 [± 2.4] % in CI-2) (Figure 3D).
The results of sentence scores were very similar to the other speech tests. The scores of CI-2 were better in Group B than those in Group A (Figure 3E, F).
Correlations between the speech intelligibility scores of CI-2 and other factors
The correlation between the speech intelligibility test scores of CI-2 and other factors was evaluated (Figure 4). The operation age of CI-1 was not correlated with the scores of the speech intelligibility test of CI-2 (Pearson’s r was −.241 in monosyllabic word score, −.248 in disyllabic word score, and −.239 in sentence score). On the other hand, the age at CI-2 was negatively correlated with the performance of CI-2. Both monosyllabic and disyllabic word scores decreased in older age (Pearson’s r was −.408, −.495, and −.437 in monosyllabic word, disyllabic word, and sentence score, respectively). Thus, the inter-implant period also showed negative correlations with the scores of CI-2. The shorter the inter-implant period was, the better results of CI-2 could be expected. Correlations between the speech intelligibility test scores and some factors. Age at CI-2 showed negative correlations with the performance of CI-2. The inter-implant period also demonstrated negative correlations with the scores of CI-2.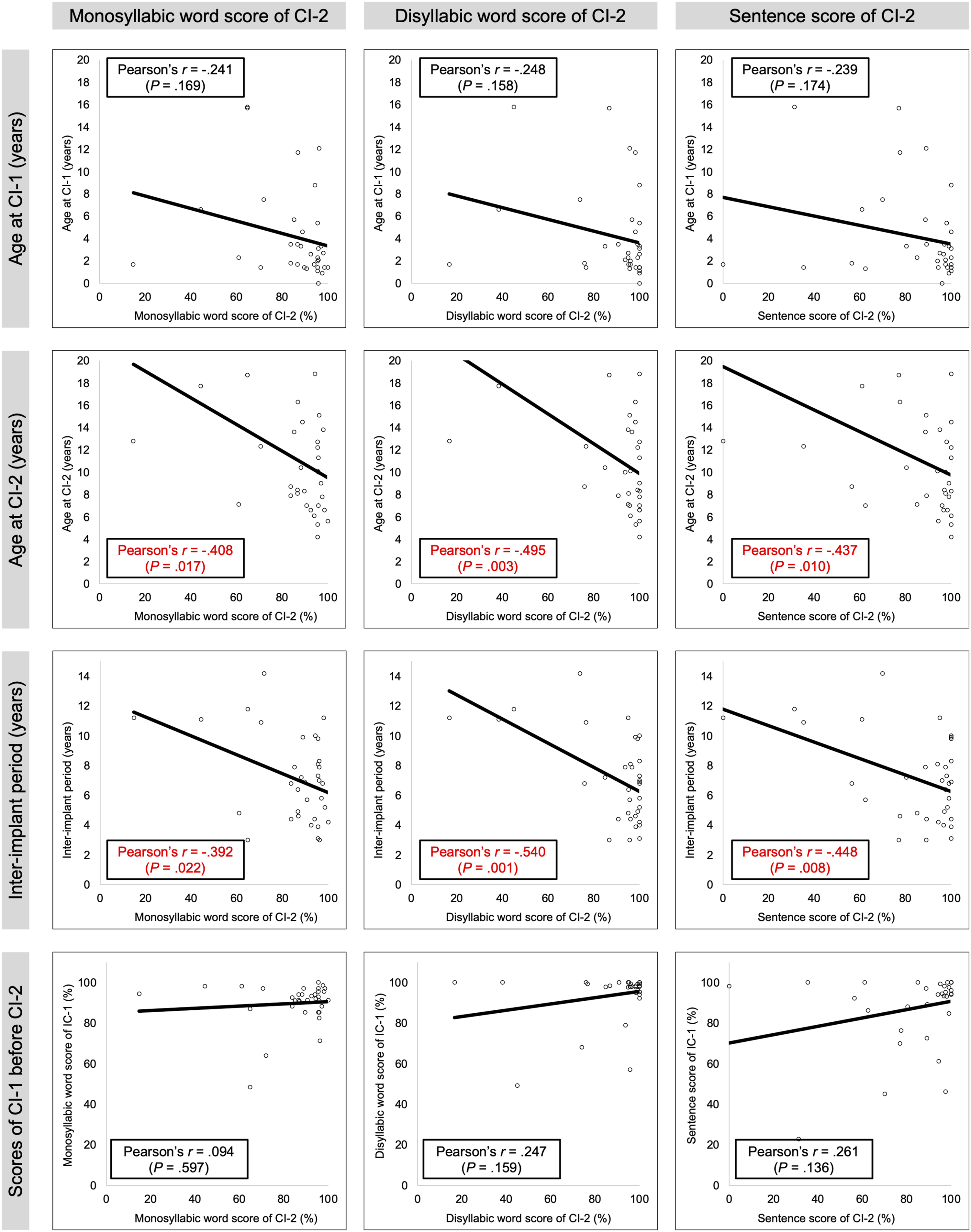
Meanwhile, there was no correlation between the performance of CI-1 and the scores of CI-2 in this study population. Overall, to maximize the speech intelligibility on CI-2-only condition, it may be still important to perform the second implantation as early as possible.
Discussion
Since it has been well known that receiving CI as early as possible has a positive effect on speech and language development, nowadays most children with congenital bilateral deafness undergo CI before the age of 2.8,10,21,22 The average age of the first CI, however, in this study was about 4-year-old, higher than the recent tendency. It was because most cases of this study had the following different characteristics and social situations. First, many subjects had shown moderate-to-severe or severe hearing loss, not deaf, which was discovered over time. Second, some cases showed progressive hearing loss. Third, the newborn hearing screening program began in the late 2000s nationally. Fourth, in Korea, unilateral CI was begun to be covered by the National Health Insurance Service from 2005. Thus, the economic burden was one of the causes for these delayed implantations.
In addition, bilateral CI has been supported since 2009. Before 2009, due to mainly financial burden, bilateral CI was not that feasible in bilateral severe to profound SNHL pediatrics in Korea. At that time, therefore, it was important to maximize the performance of CI-1. For this purpose, if the hearing of one ear was better, that is, 80 dB in one and >90 dB in another, the first implantation was used to being performed on the ear with the better hearing. Meanwhile, if the hearing of one ear was worth attempting an HA and another was guaranteed to have sufficient spiral ganglion nerve fibers, that is, 65 dB in one and 85 dB in another, the CI-1 was used to being implanted on the ear with the worse hearing. After that, because the National Medical Insurance began to cover bilateral CI and afforded the second implantation to those who underwent the first CI from 2009, bilateral sequential CI with a long inter-implant period (even more than 10 years) could be performed in Korea. This was a background that made it possible to conduct this retrospective study about bilateral sequential CI with a long inter-implant period.
Although bilateral CI is strongly recommended, these two implantations performed either simultaneously or sequentially within a short interval are not available in all patients. The financial cost may be the most common reason. According to a study conducted in South Africa, the financial cost for the second implant procedure (91.7%) and the cost for the device maintenance (75.0%) were the most common barriers for the second surgery. 19 In addition, some parents do not have certainty for the second CI and do expect other rehabilitation methods that might be developed in the future. 20 Thus, even though physicians recommend bilateral surgeries, some patients and families decide to undergo unilateral CI only. If things change, however, they might decide to receive the second CI several years later. In fact, for example, in Korea, as we described above, when the National Medical Insurance began to support the second one, many underwent CI-2, despite several years of the inter-implant period. Overall, deciding which ear to implement the CI-1 in some cases is still a matter that needs to be considered: 1) Performance of CI-1 should be maximized to provide for the possibility of failure to perform CI-2, and 2) achievement of binaural hearing after surgery of CI-2 after years later should be also deliberated.
The first CI should be recommended to perform on the ear with worse hearing. As illustrated in Figure 1, even with the first CI on a worse hearing ear, its performance never deteriorates, when compared with the patients with the first CI on a better hearing side. It means that even if the patients finally refuse the second one, there may be no functional problem of CI-1. In addition, if they receive the second surgery several years later, it will be likely that the second implant functions better and is used well. In this study, some patients in Group A (CI-1 on the better ear) did not use the second one. This was consistent with previous studies showing that the use of the second CI decreased when the inter-implant period was long.6,15 If unilateral CI use was prolonged, it caused re-organization of the rostral brainstem, which affected another ear. 23 This was why the CI-2 performance of Group B was better in this study. Auditory stimulation through an HA in the opposite ear may slow down the re-organization.
Although the shorter the inter-implant period within 12 months, the better outcomes in bilateral sequential CI,4,6,15–17 even in patients with a long interval, audiological benefits could be achieved from their bilateral CI.24–26 Rather, the performance of the first CI, not the inter-implant period, was the most significant predictor of the binaural benefits.24,25,27 In our study, we investigated factors showing correlations with the performance of the second CI. The earlier the second surgery, that was, the shorter the inter-implant period, the higher scores were observed (Figure 4). If a patient decides to receive the second CI belatedly, it is still reasonable to perform the surgery as soon as possible.
There was one interesting result in Group C. They showed symmetrical hearing levels in both ears when undergoing the first CI. Group C showed the worst performance of CI-1 (Figure 1). After the second CI, on the other hand, their scores of the speech tests sharply increased under the bilateral CI condition (Figure 2.). Some parents of patients in Group C might be reluctant to perform the second CI due to the dissatisfied outcomes of the first one. However, in these cases, it seems more necessary to persuade them to receive the second CI.
There were some limitations of the present study. The study did not include test results that could directly identify the gain of binaural hearing, such as the Hearing In Noise Test or sound localization test. In a few of the patients, the tests could be performed, but they were not analyzed in the study. The number of the subjects who underwent the tests was a little limited to get robust results. Also, socioeconomic status may be important for children’s use of CI. 18 However, detailed information on the status could not be sufficiently investigated, so this study did not include them.
Conclusions
Bilateral CI performed simultaneously or sequentially but with a short inter-implant period is the ideal treatment for children with bilateral severe to profound SNHL. However, if sequential bilateral CI cannot be performed within a short interval, the selection of the first ear for CI may be important in planning surgery. According to our study, we can conclude that the first CI is strongly recommended to be implanted on a worse hearing ear, even if they had different hearing levels between ears. Even with the first CI on a worse hearing ear, its performance never deteriorates. In addition, if they receive the second CI several years later, it will be likely that the second one functions better.
Footnotes
Acknowledgments
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science, and Technology (NRF-2019R1A2C2002384).
Conflicts of Interested Disclosures
The authors declare no conflicts of interest related to the present study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.