
Abstract
Bilateral temporal bone fractures (TBFs) involving the otic capsule are uncommon, but can result in simultaneous severe auditory and vestibular dysfunction. We present the case of a 59 year-old male patient who experienced bilateral hearing loss and vertigo following a backward fall from a height of 2 m. Temporal bone computed tomography scans revealed bilateral fractures involving the otic capsule with hemorrhage in both mastoid cavities. Audiologic evaluation confirmed bilateral profound sensorineural hearing loss, and vestibular testing indicated bilateral vestibular hypofunction. The patient underwent unilateral cochlear implantation (CI) on the left side, resulting in improved aided hearing thresholds (~45 dB HL) and enhanced verbal communication. He also participated in customized vestibular rehabilitation, comprising 4 sessions over 8 weeks. Clinical improvement was observed in balance confidence, visual acuity during head movement, and postural control tests. The Dizziness Handicap Inventory score decreased from 16 to 0, while the Activities-Specific Balance Confidence Score increased from 59% to 78%. This case emphasizes the importance of integrated auditory and vestibular rehabilitation in patients with bilateral TBFs, demonstrating that CI combined with vestibular therapy can facilitate significant functional recovery.
Keywords
Introduction
Temporal bone fractures (TBFs) most commonly result from high-energy blunt head trauma and are associated with various otologic and neurologic complications. While most TBFs are unilateral and longitudinal in orientation, bilateral fractures are rare and typically occur in the context of severe craniofacial trauma. Among these, fractures that involve the otic capsule are particularly concerning, as they significantly increase the risk of profound sensorineural hearing loss and vestibular dysfunction, both of which can severely impair communication, balance, and overall quality of life.1,2
Cochlear implantation (CI) is recognized as the most effective intervention for bilateral profound hearing loss. However, post-traumatic cases present unique surgical challenges, including distorted cochlear anatomy, ossification, and risks to the cochlear nerve, that may complicate electrode insertion and increase the risk of facial nerve stimulation. 3 Although overall outcomes may be comparable regardless of otic capsule involvement, evidence suggests that early implantation, guided by thorough imaging, can mitigate ossification and improve prognosis in patients with otic capsule–violating injuries. 4
Vestibular dysfunction is also a common consequence of TBF, especially when bilateral, and may lead to debilitating symptoms, including imbalance, oscillopsia, and increased fall risk. Despite its clinical importance, vestibular hypofunction is frequently under-recognized and undertreated in these patients. Vestibular rehabilitation therapy (VRT), including gaze stabilization exercises, postural control training, and dynamic balance tasks, has been shown to facilitate central compensation and improve functional outcomes.5,6 However, reports on the integrated approach combining CI and VRT in bilateral TBF cases remain limited.
This report presents a rare case of a patient with bilateral TBFs resulting in complete hearing loss and bilateral vestibular hypofunction (BVH). We describe the clinical course and outcomes following unilateral CI and structured vestibular rehabilitation, emphasizing the importance of coordinated auditory and balance rehabilitation in such complex cases.
Case Presentation
A 59-year-old male presented to the emergency department after falling backward from a height of approximately 2 m from a delivery truck. He sustained a traumatic head injury and reported immediate bilateral hearing loss and vertigo. On physical examination, both tympanic membranes appeared normal; however, further evaluation, including assessment for spontaneous nystagmus, could not be performed due to the patient’s lack of cooperation. Brain computed tomography (CT) revealed an intracranial hemorrhage, and temporal bone CT demonstrated bilateral TBFs involving both vestibular systems, along with hemorrhage within the mastoid air cells (Figure 1). Following the trauma, physical examination revealed intact bilateral facial nerve function without any evidence of weakness or asymmetry. The patient was admitted under the neurosurgery team for conservative management of associated intracranial hemorrhage. Subsequent evaluation by the otolaryngology department included comprehensive audiologic and vestibular assessments.
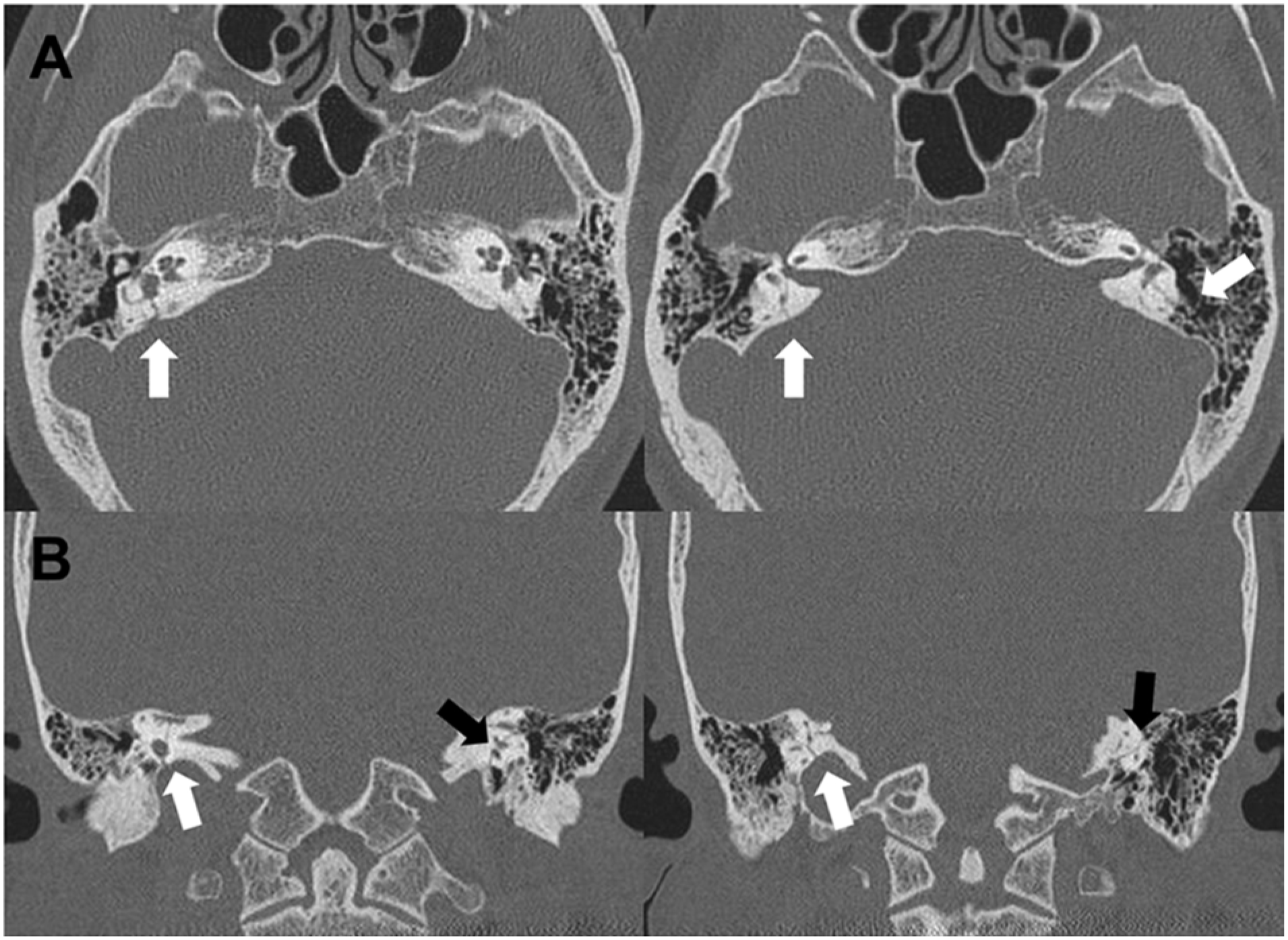
Preoperative temporal bone CT findings. Axial (A) and coronal (B) CT images reveal bilateral otic capsule–violating temporal bone fractures. White arrows indicate fracture lines extending through the vestibular apparatus. CT, computed tomography.
Pure-tone audiometry demonstrated bilateral profound sensorineural hearing loss, consistent with deafness (Figure 2A). The patient also reported severe tinnitus, with a Tinnitus Handicap Inventory (THI) score of 90, which was more pronounced on the left side. Language perception assessment showed a Category of Auditory Performance score of 0, indicating an inability to perceive speech, rendering verbal communication impossible. Caloric testing demonstrated bilateral areflexia across all 4 thermal stimuli, confirming absent lateral semicircular canal responses. Video head impulse testing revealed markedly-reduced vestibulo-ocular reflex (VOR) gain in all 6 semicircular canals (gain range: 0.26-0.36; normal >0.75-0.85), accompanied by overt catch-up saccades, consistent with BVH. Posturography revealed significant balance deficits, showing repeated falls in conditions 4 to 6. The composite score of 27 indicated severely-impaired postural stability under sensory conflict (Figure 2B-D).
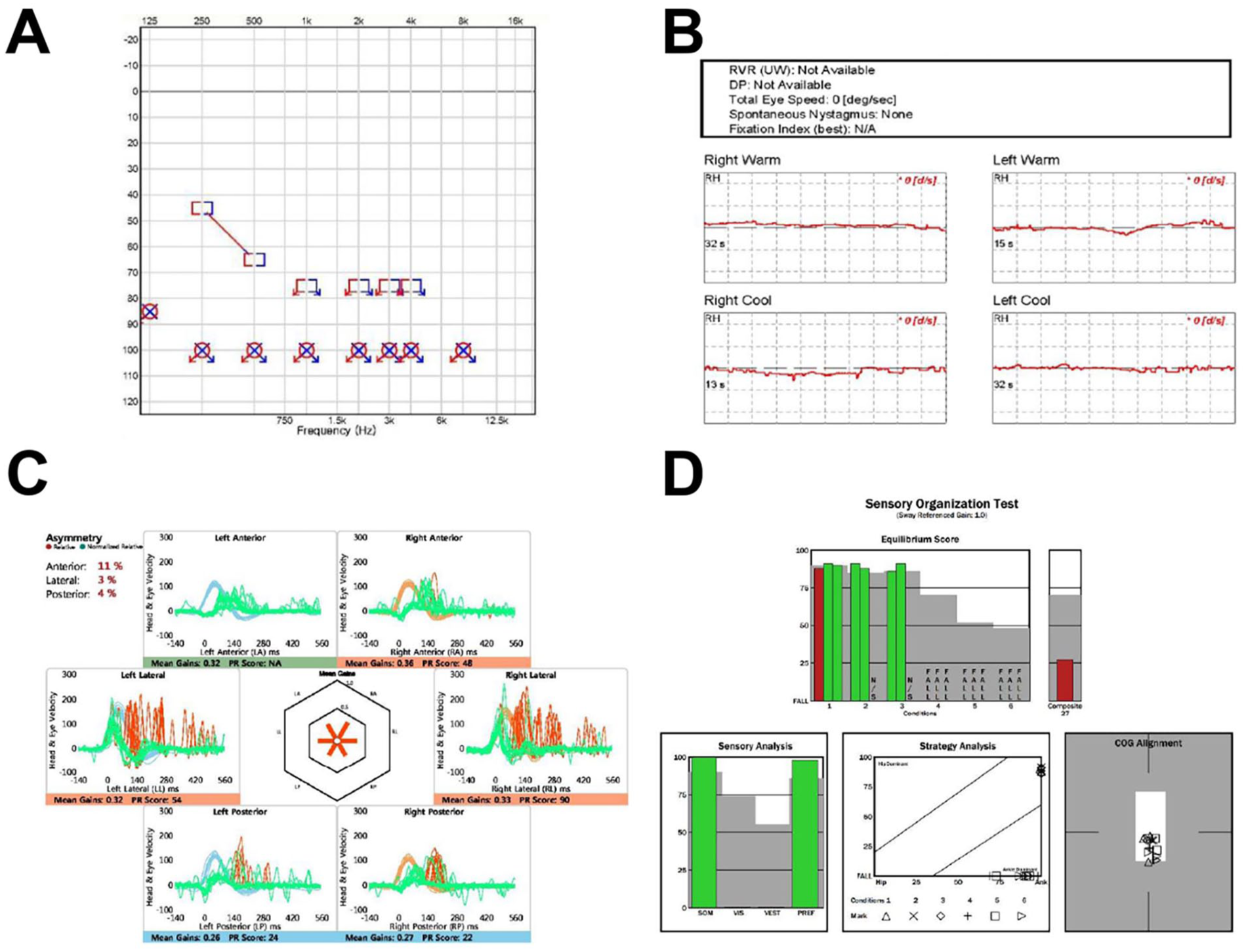
Audiologic and vestibular function assessments. (A) Preoperative pure-tone audiometry showing bilateral profound sensorineural hearing loss across all test frequencies. (B) Caloric testing demonstrated bilateral areflexia across all 4 thermal stimuli, confirming absent lateral semicircular canal responses. (C) Video Head Impulse Test results revealing significantly-reduced vestibulo-ocular reflex gains in both lateral and vertical semicircular canals, consistent with bilateral vestibular hypofunction. (D) Posturography results indicating severe postural instability, particularly under sensory-challenging conditions.
Given the irreversible nature of the hearing loss, CI was planned to restore hearing function in the patient. The patient opted for CI on the left side, as preoperative temporal bone CT revealed relatively-less damage to the left cochlea, and he reported more severe tinnitus on the left side. CI was performed approximately 3 weeks after the trauma. As the patient had no prior history of hearing loss and was in stable condition, early surgery was chosen to initiate auditory rehabilitation promptly. The cochlear implant surgery was performed using a standard round window approach, including cortical mastoidectomy and facial recess opening to access the round window for electrode insertion. Upon opening the facial recess, bony remodeling was noted near the round window niche, which obscured direct visualization of the round window. After careful drilling of the surrounding bone, soft tissue was found covering the round window. These tissues were meticulously removed, enabling atraumatic exposure of the round window membrane. The electrode was then inserted, and the procedure was completed without complications (Figure 3). No evidence of perilymph leakage was observed intraoperatively. The cochlear implant was activated 3 weeks after surgery, and postoperative CI-aided audiometry revealed aided hearing thresholds approximately 45 dB HL across key frequencies, indicating functional benefit from the implant. The patient’s tinnitus improved, with the THI score decreasing to 50. The patient is currently undergoing auditory rehabilitation and has achieved a conversational level of speech understanding, with significant improvement in verbal communication.
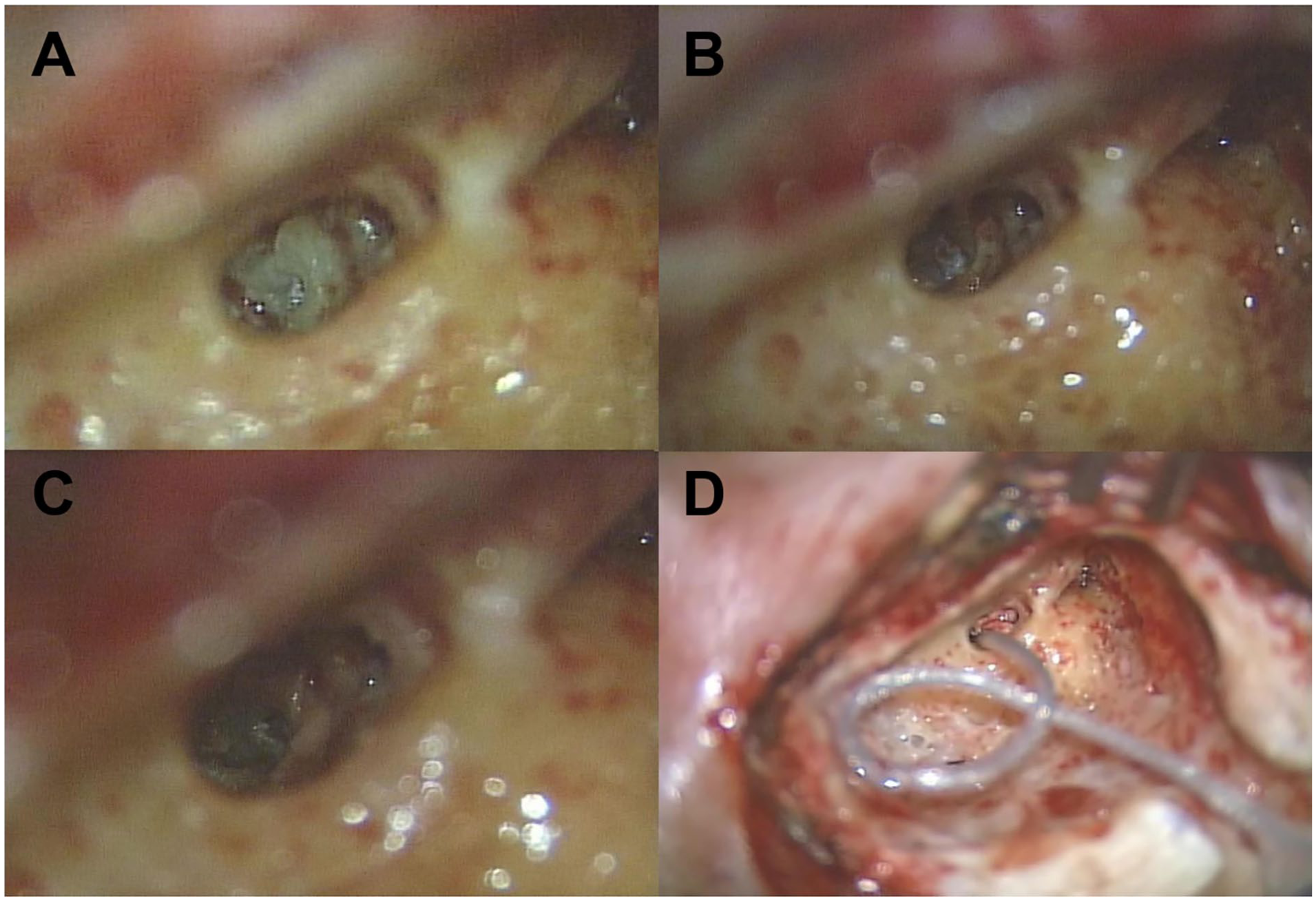
Intraoperative findings during cochlear implantation. (A) The cochlea was not readily visible due to bony remodeling upon opening the facial recess. (B) Partial removal of overlying bone and soft tissue revealed limited exposure of the cochlear and round window. (C) After complete removal of obstructing structures, the round window and cochlea were fully visualized. (D) Electrode array was successfully inserted, and the round window was sealed.
Additionally, the patient was enrolled in a customized vestibular rehabilitation program to improve balance and compensate for bilateral vestibular loss. To design a customized vestibular rehabilitation program, the patient underwent a comprehensive vestibular and balance function assessment. Although self-reported symptoms were relatively mild, with a Vestibular Visual Analog Scale (VAS) score of 1/10 and a Dizziness Handicap Inventory (DHI) total score of 16, the patient reported notable functional limitations. The Disability Scale score was 3 (range 0-4), and the Activities-Specific Balance Confidence (ABC) Scale score was 59%, indicating substantial anxiety and impairment in maintaining balance during daily activities. VOR function was assessed using the Dynamic Visual Acuity (DVA) test, revealing a 10-line drop from static (1.5) to dynamic (0.2) acuity, indicating significant VOR dysfunction. Balance evaluation included the Romberg and modified Clinical Test of Sensory Interaction on Balance (mCTSIB). The patient maintained standard Romberg posture with eyes open and closed, but lost balance after 3 seconds in the sharpened stance and could not perform it with eyes closed. In mCTSIB, balance was stable on a firm surface but not maintained beyond 5 seconds on foam, suggesting marked vestibular dysfunction. Gait was tested using the walking and pivot turn item from the Dynamic Gait Index, showing that the patient could turn and stabilize within 3 seconds.
The patient underwent 4 biweekly vestibular rehabilitation sessions. Each session progressively targeted VOR training, postural balance, and gait adaptation. VOR exercises began with seated gaze stabilization and progressed to standing tasks in visually-complex environments. Balance training began with maintaining a wide-based Romberg stance on a firm surface for 30 seconds, gradually advancing to narrow stance tasks on foam. Gait training progressed from straight-line walking to dual-task conditions, such as while turning the head or engaging in conversation, and to walking on uneven or dimly-lit surfaces. Following 4 sessions, the patient reported significant improvements. Vestibular VAS and DHI scores reduced to 0, Disability Scale was 0, and the ABC Scale improved to 78%. Although the DVA test showed no measurable improvement, the patient reported complete resolution of subjective oscillopsia from the third session of the program onward. Sharpened Romberg performance improved to over 30 seconds in the eyes-closed condition. The patient could walk in a straight line without difficulty under normal conditions. Under dual-task conditions, a slight leftward deviation was observed; however, the patient could still walk more than 10 m without falling. The detailed progress in each session is presented in Table 1.
Detailed Progress of the Patient Following Customized Vestibular Rehabilitation Therapy.
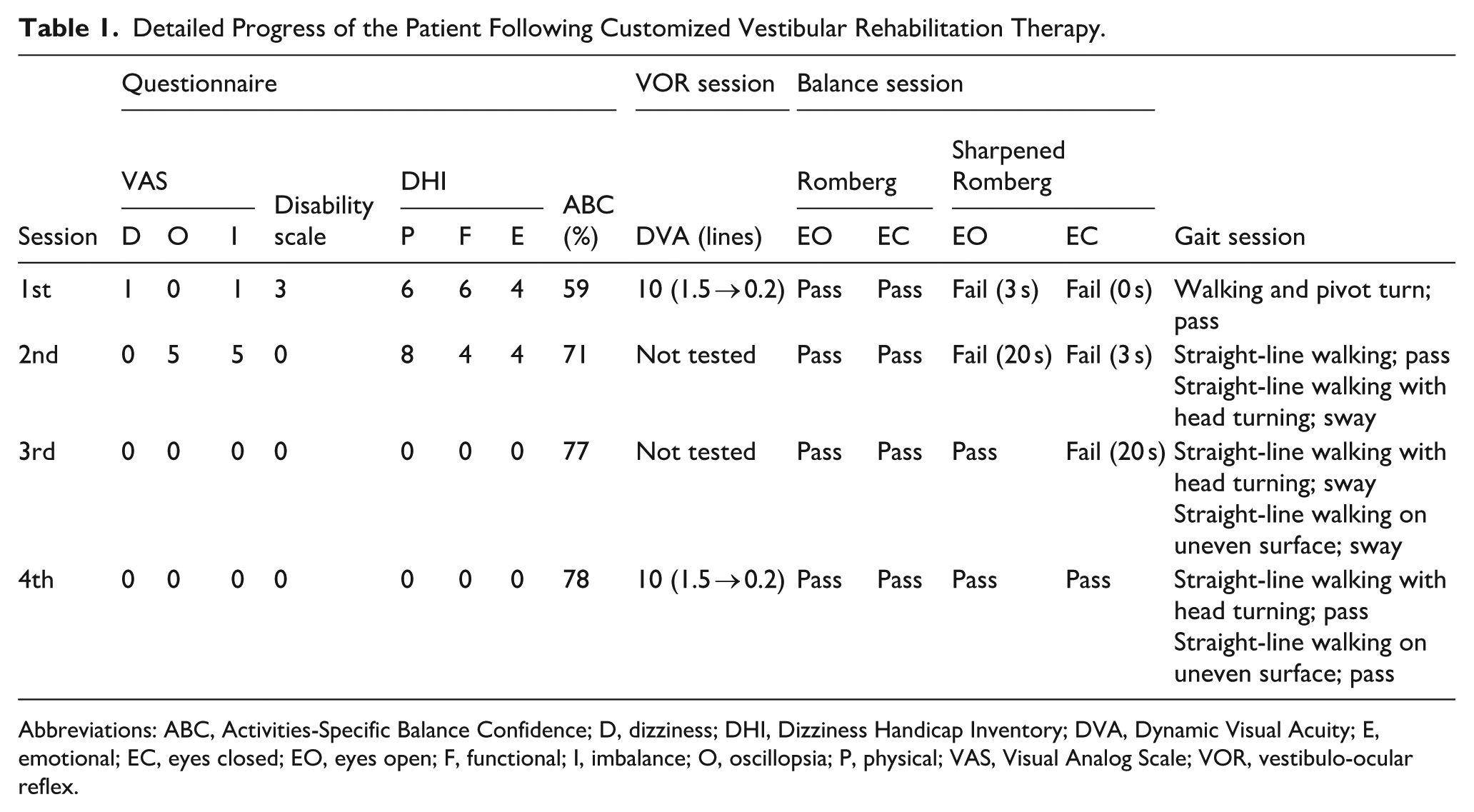
Abbreviations: ABC, Activities-Specific Balance Confidence; D, dizziness; DHI, Dizziness Handicap Inventory; DVA, Dynamic Visual Acuity; E, emotional; EC, eyes closed; EO, eyes open; F, functional; I, imbalance; O, oscillopsia; P, physical; VAS, Visual Analog Scale; VOR, vestibulo-ocular reflex.
Discussion
This case underscores the complex clinical challenges posed by bilateral TBFs, which, while rare, can lead to profound sensorineural hearing loss and bilateral vestibular dysfunction. The combination of these impairments significantly disrupts communication, postural stability, safe ambulation, and overall quality of life, necessitating a multidisciplinary rehabilitation approach.
CI remains the most effective method for auditory rehabilitation in patients with bilateral profound hearing loss. CI in patients with profound hearing loss following TBF has been frequently reported. A recent meta-analysis identified 96 cases of CI after TBF from 23 studies, of which 48 involved otic capsule–violating fractures, similar to the present case. 7 However, intraoperative findings in these 48 cases were highly variable. While some cases demonstrated minimal disruption to cochlear anatomy and enabled successful implantation without difficulty,8 -14 others, including the current case, presented with bony remodeling due to fracture or intracochlear fibrosis and ossification, complicating electrode insertion.15 -18 Another case series reporting CI outcomes in 14 patients with TBF also described various intraoperative findings in otic capsule–violating fractures. 19 These differences are likely attributable to the extent of the fracture, the degree of endolymphatic leakage, and the individual inflammatory response at the injury site. Notably, such fibrosis or ossification may not be readily apparent on preoperative CT imaging. 20 Therefore, comprehensive preoperative imaging, including MRI, is essential. Surgeons should also be prepared for altered surgical plans, including the possibility of cochleostomy or insertion via the scala vestibuli in cases where round window access is not feasible.
Outcomes of CI in otic capsule–violating fractures have been reported with considerable variability. One study involving 14 patients with TBF demonstrated significantly-poorer CI outcomes in the otic capsule–violating group than in the sparing group. 19 In contrast, a meta-analysis of 96 cases concluded that overall outcomes in the otic capsule–violating group were generally favorable, even in cases with partial insertion due to ossification or fibrosis, and not significantly different from non-fracture cases. 7 Some studies further suggest that CI outcomes are more strongly associated with the patient’s age at implantation than with the time elapsed since the injury. 19 Considering these findings, it is reasonable to expect that patients with TBFs, even those with otic capsule violation or partial electrode insertion, may still achieve substantial benefit from CI, despite the technical challenges involved.
The patient displayed oscillopsia, imbalance, and gait disturbance, which are typical manifestations of BVH, which were irreversible due to damage to the vestibular structures. Current therapeutic strategies for BVH are primarily symptomatic and rehabilitative rather than curative, due to the limited residual vestibular input. According to the practice parameter published by the American Academy of Neurology, VRT is the only intervention shown to significantly improve function in patients with BVH. 21 VRT aims to restore daily function not by recovering vestibular function itself but by enhancing compensation through other sensory modalities, including visual and proprioceptive inputs. 22 Generic VRTs, such as the Cawthorne-Cooksey, Norré, and Hamid exercises, have long been utilized and shown to improve balance and reduce symptoms in patients with vestibular dysfunction. 23 However, recent clinical evidence suggests that customized VRT, tailored to the individual’s specific impairments and functional goals, leads to superior outcomes compared to generic protocols, particularly in complex cases such as BVH. In patients with BVH, customized VRT has shown consistent benefits. A 6 week program improved dizziness and daily function across lesion sites, especially in severe cases. 24 A systematic review confirmed moderate-to-strong evidence for enhanced gaze and postural stability. 25 Additionally, an 8-week program improved dizziness, balance, daily activities, sleep, and quality of life. 26 These findings support the use of customized VRT in our patient.
Vestibular symptoms are common following TBFs; however, up to 59% of patients have reported symptoms that persist for more than 3 months. 27 Vestibular dysfunction secondary to TBF presents a more complex rehabilitative challenge. Due to the disruption of both the bony labyrinth and associated neural elements, TBFs pose a significantly-greater challenge for vestibular rehabilitation than lesions confined to peripheral vestibular structures, such as in vestibular neuritis. 1 Additionally, fracture-related labyrinthine ossification and fibrosis may hinder compensation and limit the efficacy of rehabilitation. 28 Vestibular injury caused by trauma may be accompanied by various sensory and neurologic deficits, including traumatic brain injury, 29 and some patients may experience persistent difficulties due to post-traumatic dizziness. 30 The patient achieved substantial symptom resolution by 1 month post-injury through customized VRT. By progressively advancing through gaze stabilization exercises, postural control training, and dynamic balance tasks tailored to symptom severity, the patient could attain function improvement despite the absence of vestibular function recovery.
This case highlights the clinical value of a multidisciplinary approach in managing bilateral TBFs with combined auditory and vestibular loss. Despite the structural disruption of the cochlea and vestibular apparatus, early CI and individually-tailored vestibular rehabilitation enabled the patient to regain meaningful auditory communication and functional mobility. The integration of precise preoperative imaging, meticulous surgical planning, and symptom-oriented, progressive VRT not only facilitated recovery but also highlighted the importance of compensatory mechanisms in the absence of neural restoration. This underscores the potential of coordinated interventions to maximize functional outcomes even in anatomically-complex and neurologically-compromised cases.
Conclusion
Bilateral TBFs involving both the cochlea and vestibular system are rare but profoundly disabling. This case highlights that early CI, combined with customized vestibular rehabilitation, can lead to meaningful recovery of communication and balance function even in the absence of structural recovery. An individualized, multidisciplinary approach is key to optimizing outcomes in such complex cases.
Footnotes
Ethical Considerations
This case report was conducted in accordance with the Declaration of Helsinki. The study was approved by the Institutional Review Board of Incheon St. Mary’s Hospital (IRB No. OC25ZASI0073), which waived the requirement for informed consent due to the retrospective nature of the report. All data were fully anonymized, and no identifiable patient information is included.
Author Contributions
JML: Data acquisition and writing—original draft. HJL: Performed a surgery and involved in editing and revising the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (NRF-RS-2023-00210073) to HJL.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this case report are available from the corresponding author upon reasonable request.